
Abstract
Background
Catheter ablation is of growing importance in patients with an ischemic cardiomyopathy and recurrent episodes of ventricular tachyarrhythmias. Most ablation strategies in these patients are based on the detection of areas of scar and border zones to normal myocardium. However, the mapping criteria for identifying these areas have not been validated sufficiently so far. Therefore, we have performed a comparison between electroanatomical bipolar voltage maps obtained during substrate-based VT ablation procedures and [18 F]fluoro-2-deoxyglucose PET studies performed prior to these procedures.
Methods
Seven patients suffering from severe coronary artery disease and repetitive ventricular tachycardias were enrolled in this study. In all patients, there was a history of myocardial infarction and the left ventricular function was severely impaired. A FDG PET was performed at least 1 day prior to the ablation procedure in all patients. Then, a substrate-based VT ablation procedure was performed using the CARTO system (Biosense Webster, Diamond Bar, CA, USA). Finally, the FDG PET images and the bipolar voltage maps were compared in all patients.
Results
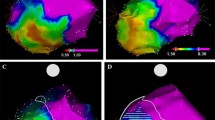
The ablation procedures could be performed successfully in all patients and 1–5 monomorphic VTs could be eliminated in each patient. There were no major complications. At 1-year follow-up, five out of seven patients (71.4%) remained free from any arrhythmia recurrence. In all patients, there were extensive areas of scar and adjacent low-voltage areas could be identified in the CARTO bipolar voltage maps. In areas commonly defined as “dense scar” (bipolar voltage amplitude <0.5 mV), the mean FDG uptake was 43.1% (SD ±18.2%) indicating predominantly scar tissue. In the so-called low-voltage border zones the mean FDG uptake ranged between 49.5% [(SD ±15.8%); >0.5–1 mV] and 60.1% [(SD ±14.8%); >1–1.5 mV], thereby indicating the presence of predominantly viable myocardium. In areas with a bipolar voltage amplitude >1.5 mV the presence of viable myocardium was confirmed by a mean FDG uptake of approximately 60%.
Conclusions
The results of our study demonstrate that there is a significant amount of viable myocardium in the low-voltage border zones of scars frequently targeted as ablation sites. Therefore, RF current delivery in these areas should be restricted to the minimum assumed to be necessary for successful catheter ablation because extensive RF applications might result in a further deterioration of the left ventricular function. Larger studies are needed to validate our results and to develop more reliable criteria for distinguishing areas of scar from viable myocardium in CARTO bipolar voltage maps.


Similar content being viewed by others


Abbreviations
- BMI:
-
Body mass index
- ECG:
-
Electrocardiogram
- EP:
-
Electrophysiology
- FDG:
-
[18 F]fluoro-2-deoxyglucose
- ICD:
-
Implantable cardioverter defibrillator
- PET:
-
Positron-emission tomography
- RF:
-
Radiofrequency
- SD:
-
Standard deviation
- TIA:
-
Transient ischemic attacks
- VF:
-
Ventricular fibrillation
- VT:
-
Ventricular tachycardia
References
Marchlinski F, Callans D, Gottlieb C (2000) Zado E: Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation 101:1288–1296
Callans D, Ren J, Michele J, Marchlinski F (1999) Dillon S: Electroanatomic left ventricular mapping in the porcine model of healed anterior myocardial infarction Correlation with intracardiac echocardiography and pathological analysis. Circulation 100:1744–1750
Kornowski R, Hong M, Gepstein S, Goldstein S, Ellahham S, Ben-Haim S, Leon M (1998) Preliminary animal and clinical experiences using an electromechanical endocardial mapping procedure to distinguish infarcted from healthy myocardium. Circulation 98:1116–1124
Callans D, Zado E, Sarter B, Schwartzman D, Gottlieb C, Marchlinski F (1998) Efficacy of radiofrequency catheter ablation for ventricular tachycardia in healed myocardial infarction. Am J Cardiol 82:429–432
Schreieck J, Zrenner B, Deisenhofer I, Schmitt C (2005) Rescue ablation of electrical storm in patients with ischemic cardiomyopathy: a potential-guided ablation approach by modifying substrate of intractable, unmappable ventricular tachycardias. Heart Rhythm 2:10–14
Schreieck J (2006) Ventricular tachycardia. In: Schmitt C, Deisenhofer I, Zrenner B (eds) Catheter ablation of cardiac arrhythmias, 1st edn. Steinkopff/Springer, Darmstadt/Germany, pp 183–210
Reddy V, Reynolds M, Neuzil P, Richardson A, Taborsky M, Jongnarangsin K, Kralovec S, Sediva L, Ruskin J, Josephson M (2007) Prophylactic catheter ablation for the prevention of defibrillator therapy. N Engl J Med 357:2657–2665
Antz M, Berodt K, Baensch D, Ernst S, Chun K, Satomi K, Schmidt B, Boczor S, Ouyang F, Kuck K (2008) Catheter ablation of ventricular tachycardia in patients with coronary artery disease: influence of the endocardial substrate size on clinical outcome. Clin Res Cardiol 97(2):110–117
Kettering K, Kampmann C, Mollnau H, Kreitner F, Muenzel T, Weiss C (2009) Catheter ablation of an incessant ventricular tachycardia originating from the left aortic sinus cusp in an adolescent with subacute myocarditis. Clin Res Cardiol 98(1):66–70
Acknowledgments
The study was supported by the German Research Foundation [Deutsche Forschungsgemeinschaft (DFG); Sonderforschungsbereich/Transregio—19: “Inflammatorische Kardiomyopathie—Molekulare Pathogense und Therapie”].
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kettering, K., Weig, H.J., Reimold, M. et al. Catheter ablation of ventricular tachycardias in patients with ischemic cardiomyopathy: validation of voltage mapping criteria for substrate modification by myocardial viability assessment using FDG PET. Clin Res Cardiol 99, 753–760 (2010). https://doi.org/10.1007/s00392-010-0182-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-010-0182-2