
Abstract
Purpose
In this study, the potential contribution of Dixon-based MR imaging with a rapid low-resolution breath-hold sequence, which is a technique used for MR-based attenuation correction (AC) for MR/positron emission tomography (PET), was evaluated for anatomical correlation of PET-positive lesions on a 3T clinical scanner compared to low-dose CT. This technique is also used in a recently installed fully integrated whole-body MR/PET system.
Methods
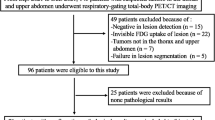
Thirty-five patients routinely scheduled for oncological staging underwent 18F-fluorodeoxyglucose (FDG) PET/CT and a 2-point Dixon 3-D volumetric interpolated breath-hold examination (VIBE) T1-weighted MR sequence on the same day. Two PET data sets reconstructed using attenuation maps from low-dose CT (PETAC_CT) or simulated MR-based segmentation (PETAC_MR) were evaluated for focal PET-positive lesions. The certainty for the correlation with anatomical structures was judged in the low-dose CT and Dixon-based MRI on a 4-point scale (0–3). In addition, the standardized uptake values (SUVs) for PETAC_CT and PETAC_MR were compared.
Results
Statistically, no significant difference could be found concerning anatomical localization for all 81 PET-positive lesions in low-dose CT compared to Dixon-based MR (mean 2.51 ± 0.85 and 2.37 ± 0.87, respectively; p = 0.1909). CT tended to be superior for small lymph nodes, bone metastases and pulmonary nodules, while Dixon-based MR proved advantageous for soft tissue pathologies like head/neck tumours and liver metastases. For the PETAC_CT- and PETAC_MR-based SUVs (mean 6.36 ± 4.47 and 6.31 ± 4.52, respectively) a nearly complete concordance with a highly significant correlation was found (r = 0.9975, p < 0.0001).
Conclusion
Dixon-based MR imaging for MR AC allows for anatomical allocation of PET-positive lesions similar to low-dose CT in conventional PET/CT. Thus, this approach appears to be useful for future MR/PET for body regions not fully covered by diagnostic MRI due to potential time constraints.





Similar content being viewed by others

References
Antoch G, Bockisch A. Combined PET/MRI: a new dimension in whole-body oncology imaging? Eur J Nucl Med Mol Imaging 2009;36:S113–20.
Zaidi H, Mawlawi O, Orton CG. Point/counterpoint. Simultaneous PET/MR will replace PET/CT as the molecular multimodality imaging platform of choice. Med Phys 2007;34:1525–8.
Seemann MD. Whole-body PET/MRI: the future in oncological imaging. Technol Cancer Res Treat 2005;4:577–82.
Antoch G, Vogt FM, Freudenberg LS, Nazaradeh F, Goehde SC, Barkhausen J, et al. Whole-body dual-modality PET/CT and whole-body MRI for tumor staging in oncology. JAMA 2003;290:3199–206.
Fonti R, Salvatore B, Quarantelli M, Sirignano C, Segreto S, Petruzziello F, et al. 18F-FDG PET/CT, 99mTc-MIBI, and MRI in evaluation of patients with multiple myeloma. J Nucl Med 2008;49:195–200.
Angtuaco EJC, Fassas ABT, Walker R, Sethi R, Barlogie B. Multiple myeloma: clinical review and diagnostic imaging. Radiology 2004;231:11–23.
Herholz K, Coope D, Jackson A. Metabolic and molecular imaging in neuro-oncology. Lancet Neurol 2007;6:711–24.
Ruf J, Lopez Hänninen E, Böhmig M, Koch I, Denecke T, Plotkin M, et al. Impact of FDG-PET/MRI image fusion on the detection of pancreatic cancer. Pancreatology 2006;6:512–9.
Schmidt GP, Haug AR, Schoenberg SO, Reiser MF. Whole-body MRI and PET-CT in the management of cancer patients. Eur Radiol 2006;16:1216–25.
Lauenstein TC, Goehde SC, Herborn CU, Goyen M, Oberhoff C, Debatin JF, et al. Whole-body MR imaging: evaluation of patients for metastases. Radiology 2004;233:139–48.
Beer AJ, Eiber M, Souvatzoglou M, Schwaiger M, Krause BJ. Radionuclide and hybrid imaging of recurrent prostate cancer. Lancet Oncol 2011;12:181–91.
Beer AJ, Eiber M, Souvatzoglou M, Holzapfel K, Ganter C, Weirich G, et al. Restricted water diffusibility as measured by diffusion-weighted MR imaging and choline uptake in (11)C-choline PET/CT are correlated in pelvic lymph nodes in patients with prostate cancer. Mol Imaging Biol 2011;13:352–61.
Kinahan PE, Hasegawa BH, Beyer T. X-ray-based attenuation correction for positron emission tomography/computed tomography scanners. Semin Nucl Med 2003;33:166–79.
Zaidi H. Is MR-guided attenuation correction a viable option for dual-modality PET/MR imaging? Radiology 2007;244:639–42.
Catana A, Van Der Kouwe A, Benner T, Hamm M, Michel C, Fischl B, et al. Is accurate bone segmentation required for MR-based PET attenuation correction? Proc Int Soc Magn Reson Med 2009:593.
Delso G, Martinez-Möller A, Bundschuh RA, Ladebeck R, Candidus Y, Faul D, et al. Evaluation of the attenuation properties of MR equipment for its use in a whole-body PET/MR scanner. Phys Med Biol 2010;55:4361–74.
Keereman V, De Deene Y, Lemahieu I, Vandenberghe S. Estimation of attenuation maps from UTE derived R2 image. Proc Int Soc Magn Reson Med 2009:2774.
Hofmann M, Steinke F, Scheel V, Charpiat G, Farquhar J, Aschoff P, et al. MRI-based attenuation correction for PET/MRI: a novel approach combining pattern recognition and atlas registration. J Nucl Med 2008;49:1875–83.
Zaidi H, Montandon M, Slosman DO. Magnetic resonance imaging-guided attenuation and scatter corrections in three-dimensional brain positron emission tomography. Med Phys 2003;30:937–48.
Martinez-Möller A, Souvatzoglou M, Delso G, Bundschuh RA, Chefd’hotel C, Ziegler SI, et al. Tissue classification as a potential approach for attenuation correction in whole-body PET/MRI: evaluation with PET/CT data. J Nucl Med 2009;50:520–6.
Schulz V, Torres-Espallardo I, Renisch S, Hu Z, Ojha N, Börnert P, et al. Automatic, three-segment, MR-based attenuation correction for whole-body PET/MR data. Eur J Nucl Med Mol Imaging 2011;38:138–52. doi:10.1007/s00259-010-1603-1.
Steinberg J, Jia G, Sammet S, Zhang J, Hall N, Knopp MV. Three-region MRI-based whole-body attenuation correction for automated PET reconstruction. Nucl Med Biol 2010;37:227–35.
Boellaard R, O’Doherty MJ, Weber WA, Mottaghy FM, Lonsdale MN, Stroobants SG, et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: version 1.0. Eur J Nucl Med Mol Imaging 2010;37:181–200.
Elstrom RL, Leonard JP, Coleman M, Brown RKJ. Combined PET and low-dose, noncontrast CT scanning obviates the need for additional diagnostic contrast-enhanced CT scans in patients undergoing staging or restaging for lymphoma. Ann Oncol 2008;19:1770–3.
Pfannenberg AC, Aschoff P, Brechtel K, Müller M, Klein M, Bares R, et al. Value of contrast-enhanced multiphase CT in combined PET/CT protocols for oncological imaging. Br J Radiol 2007;80:437–45.
Schaefer NG, Hany TF, Taverna C, Seifert B, Stumpe KDM, von Schulthess GK, et al. Non-Hodgkin lymphoma and Hodgkin disease: coregistered FDG PET and CT at staging and restaging–do we need contrast-enhanced CT? Radiology 2004;232:823–9.
Maki JH, Chenevert TL, Prince MR. The effects of incomplete breath-holding on 3D MR image quality. J Magn Reson Imaging 1997;7:1132–9.
Beyer T, Weigert M, Quick HH, Pietrzyk U, Vogt F, Palm C, et al. MR-based attenuation correction for torso-PET/MR imaging: pitfalls in mapping MR to CT data. Eur J Nucl Med Mol Imaging 2008;35:1142–6.
Horger M, Claussen CD, Bross-Bach U, Vonthein R, Trabold T, Heuschmid M, et al. Whole-body low-dose multidetector row-CT in the diagnosis of multiple myeloma: an alternative to conventional radiography. Eur J Radiol 2005;54:289–97.
Lauenstein TC, Semelka RC. Emerging techniques: whole-body screening and staging with MRI. J Magn Reson Imaging 2006;24:489–98.
Ng S, Yen T, Chang JT, Chan S, Ko S, Wang H, et al. Prospective study of [18F]fluorodeoxyglucose positron emission tomography and computed tomography and magnetic resonance imaging in oral cavity squamous cell carcinoma with palpably negative neck. J Clin Oncol 2006;24:4371–6.
Vanel D, Bittoun J, Tardivon A. MRI of bone metastases. Eur Radiol 1998;8:1345–51.
van den Brekel MW. Lymph node metastases: CT and MRI. Eur J Radiol 2000;33:230–8.
Castelijns JA, van den Brekel MWM. Imaging of lymphadenopathy in the neck. Eur Radiol 2002;12:727–38.
Venkitaraman R, Cook GJR, Dearnaley DP, Parker CC, Khoo V, Eeles R, et al. Whole-body magnetic resonance imaging in the detection of skeletal metastases in patients with prostate cancer. J Med Imaging Radiat Oncol 2009;53:241–7.
Bruegel M, Gaa J, Woertler K, Ganter C, Waldt S, Hillerer C, et al. MRI of the lung: value of different turbo spin-echo, single-shot turbo spin-echo, and 3D gradient-echo pulse sequences for the detection of pulmonary metastases. J Magn Reson Imaging 2007;25:73–81.
Vogt FM, Herborn CU, Hunold P, Lauenstein TC, Schröder T, Debatin JF, et al. HASTE MRI versus chest radiography in the detection of pulmonary nodules: comparison with MDCT. AJR Am J Roentgenol 2004;183:71–8.
Martinez-Möller A, Souvatzoglou M, Navab N, Schwaiger M, Nekolla SG. Artifacts from misaligned CT in cardiac perfusion PET/CT studies: frequency, effects, and potential solutions. J Nucl Med 2007;48:188–93.
Acknowledgments
We thank Brigitte Dzewas and Sylvia Schachoff and the whole PET team for their excellent technical assistance.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Matthias Eiber and Axel Martinez-Möller contributed equally.
Stephan G. Nekolla and Ambros J. Beer share joint senior authorship.
Rights and permissions
About this article
Cite this article
Eiber, M., Martinez-Möller, A., Souvatzoglou, M. et al. Value of a Dixon-based MR/PET attenuation correction sequence for the localization and evaluation of PET-positive lesions. Eur J Nucl Med Mol Imaging 38, 1691–1701 (2011). https://doi.org/10.1007/s00259-011-1842-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-011-1842-9