
Abstract
Purpose
While CT/MR enteroclysis provides excellent anatomical details, it fails to provide information on metabolic activity of the inflammatory lesions of the intestine. We conceptualized a fusion of metabolic imaging techniques such as PET and an anatomical imaging modality such as CT enteroclysis to derive information both on morphological details and functional activity of lesions at the same time.
Patients and methods
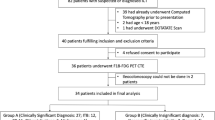
In a prospective study, we included 17 adult patients with newly diagnosed inflammatory diseases of the intestine. Low dose whole body PET-CT scan was obtained first, which began at approximately 60 min after injection of 10 mCi of 18fluoro-deoxyglucose (FDG). Subsequently, PET-CT enteroclysis of the abdomen was performed after infusion of 2 l of 0.5% methylcellulose through a naso-jejunal catheter.
Results
Fourteen patients had abnormal and three had normal PET-CT enteroclysis studies. Twenty-three segments of small intestine and 27 segments of large intestine showed increased FDG uptake. The detection rate of PET-CT enteroclysis was significantly higher (total =50 segments, 23 segments of small intestine and 27 segments of large intestine) as compared with barium studies (16 segments of small intestine) and colonoscopy (17 segments of large intestine) combined together (total =33 segments). In addition PET-CT enteroclysis showed extra-luminal FDG uptake (lymph nodes in two, sacroilitis in two, and mesenteric fat proliferation in five).
Conclusions
As a single investigation, PET-CT enteroclysis detects a significantly higher number of lesions both in the small and large intestine in comparison to that detected by conventional barium and colonoscopy combined together. This technique is non-invasive, feasible and very promising.



Similar content being viewed by others


References
Sailer J, Peloschek P, Schober E, Schima W, Reinisch W, Vogelsang H, et al. Diagnostic value of CT enteroclysis compared with conventional enteroclysis in patients with Crohn’s disease. Am J Roentgenol 2005;185:1575–81.
Mackalski BA, Bernstein CN. New diagnostic imaging tools for inflammatory bowel disease. Gut 2006;55:733–41.
Abdel-Nabi H, Doerr RJ, Lamonica DM, Cronin VR, Galantowicz PJ, Carbone GM, et al. Staging of primary colorectal carcinomas with fluorine-18 fluorodeoxyglucose whole-body PET: correlation with histopathologic and CT findings. Radiology 1998;206:755–60.
Kim JH, Czernin J, Allen-Auerbach MS, Halpern BS, Fueger BJ, Hecht JR, et al. Comparison between 18F-FDG PET, in-line PET/CT, and software fusion for restaging of recurrent colorectal cancer. J Nucl Med 2005;46:587–95.
Larson SM, Schoder H, Yeung H. Positron emission tomography/computerized tomography functional imaging of esophageal and colorectal cancer. Cancer J 2004;10:243–50.
Zhuang H, Alavi A. 18-fluorodeoxyglucose positron emission tomographic imaging in the detection and monitoring of infection and inflammation. Semin Nucl Med 2002;32:47–59.
Kresnik E, Mikosch P, Gallowitsch HJ, Heinisch M, Lind P. F-18 fluorodeoxyglucose positron emission tomography in the diagnosis of inflammatory bowel disease. Clin Nucl Med 2001;26:867.
Skehan SJ, Issenman R, Mernagh J, Nahmias C, Jacobson K. 18F-fluorodeoxyglucose positron tomography in diagnosis of paediatric inflammatory bowel disease. Lancet 1999;354:36–837.
Bicik I, Bauerfeind P, Breitbach T, von Schulthess GK, Fried M. Inflammatory bowel disease activity measured by positron-emission tomography. Lancet 1997;350:262.
Prabhakar HB, Sahani DV, Fischman AJ, Mueller PR, Blake MA. Bowel hot spots at PET-CT. Radiographics 2007;27:145–59.
Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut 2006;55:749–53.
Yoshida EM. The Crohn’s Disease Activity Index, its derivatives and the Inflammatory Bowel Disease Questionnaire: a review of instruments to assess Crohn’s disease. Can J Gastroenterol 1999;13:65–73.
Bischofdelaloye A, Wahl RL. How high level of FDG abdominal activity is considered normal? (abstract). J Nucl Med 1995;36 Suppl:106P
Kumar R, Xiu Y, Yu JQ, Takalkar A, El-Haddad G, Potenta S, et al. F18-FDG-PET in evaluation of adrenal lesions in patients with lung cancer. J Nucl Med 2004;45:2058–62.
Minordi LM, Vecchioli A, Guidi L, Mirk P, Fiorentini L, Bonomo L. Multidetector CT enteroclysis versus barium enteroclysis with methylcellulose in patients with suspected small bowel disease. Eur Radiol 2006;16:1527–36.
Goldberg HI, Gore RM, Margulis AR, Moss AA, Baker EL. Computed tomography in the evaluation of Crohn’s disease. Am J Roentgenol 1983;140:277–82.
Gore RM, Balthazar EJ, Ghahremani GG, Miller FH. CT features of ulcerative colitis and Crohn’s disease. Am J Roentgenol 1996;167:3–15.
Wittenberg J, Harisinghani MG, Jhaveri K, Varghese J, Mueller PR. Algorithmic approach to CT diagnosis of the abnormal bowel wall. RadioGraphics 2002;22:1093–1109.
Zhuang H, Pourdehnad M, Lambright ES, Yamamoto AJ, Lanuti M, Li P, et al. Dual time point 18F-FDG PET imaging for differentiating malignant from inflammatory processes. J Nucl Med 2001;42:1412–17.
Abouzied MM, Crawford ES, Nabi HA. 18FFDG imaging: pitfalls and artifacts. J Nucl Med Technol 2005;33:145–55.
Subhas N, Patel PV, Pannu HK, Jacene HA, Fishman EK, Wahl RL. Imaging of pelvic malignancies with in-line FDG PET-CT: case examples and common pitfalls of FDG PET. RadioGraphics 2005;25:1031–43.
Tatlidil R, Mandelkern M. FDG-PET in the detection of gastrointestinal metastases in melanoma. Melanoma Res 2001;11:297–301.
Rohren EM, Turkington TG, Coleman RE. Clinical applications of PET in oncology. Radiology 2004;231:305–32.
Israel O, Yefremov N, Bar-Shalom R, Kagana O, Frenkel A, Keidar Z, et al. PET/CT detection of unexpected gastrointestinal foci of 18F-FDG uptake: incidence, localization patterns, and clinical significance. J Nucl Med 2005;46:758–62.
Pandit-Taskar N, Schoder H, Gonen M, Larson SM, Yeung HW. Clinical significance of unexplained abnormal focal FDG uptake in the abdomen during whole-body PET. Am J Roentgenol 2004;183:1143–7.
Tatlidil R, Jadvar H, Bading JR, Conti PS. Incidental colonic fluorodeoxyglucose uptake: correlation with colonoscopic and histopathologic findings. Radiology 2002;224:783–7.
Gutman F, Alberini JL, Wartski M, Vilain D, Le Stanc E, Sarandi F, et al. Incidental colonic focal lesions detected by FDG PET/CT. Am J Roentgenol 2005;185:495–500.
Kresnik E, Gallowitsch HJ, Mikosch P, Wurtz F, Alberer D, Hebenstreit A, et al. (18)F-FDG positron emission tomography in the early diagnosis of enterocolitis: preliminary results. Eur J Nucl Med Mol Imaging 2002;29:1389–92.
Almer S, Granerus G, Strom M, Olaison G, Bonnet J, Lemann M, et al. Leukocyte scintigraphy compared to intraoperative small bowel enteroscopy and laparotomy findings in Crohn’s disease. Inflamm Bowel Dis 2007;13:164–74.
Lantto E, Jarvi K, Krekela I, Lantto T, Taavitsainen M, Vedenkangas H, et al. Technetium-99m hexamethyl propylene amine oxine leucocytes in the assessment of disease activity in inflammatory bowel disease. Eur J Nucl Med 1992;19:14–18.
Sciarretta G, Furno A, Mazzoni M, Basile C, Malaguti P. Technetium-99m hexamethyl propylene amine oxime granulocyte scintigraphy in Crohn’s disease: diagnostic and clinical relevance. Gut 1993;34:1364–9.
Lemberg DA, Issenman RM, Cawdron R, Green T, Mernagh J, Skehan SJ, et al. Positron emission tomography in the investigation of pediatric inflammatory bowel disease. Inflamm Bowel Dis 2005;11:733–8.
Loffler M, Weckesser M, Franzius C, Schober O, Zimmer KP. High diagnostic value of 18F-FDG-PET in pediatric patients with chronic inflammatory bowel disease. Ann N Y Acad Sci 2006;1072:379–85.
Neurath MF, Vehling D, Schunk K, Holtmann M, Brockmann H, Helisch A, et al. Noninvasive assessment of Crohn’s disease activity: a comparison of 18F-fluorodeoxyglucose positron emission tomography, hydromagnetic resonance imaging, and granulocyte scintigraphy with labeled antibodies. Am J Gastroenterol 2002;97:1978–85.
Pio BS, Byrne FR, Aranda R, Boulay G, Spicher K, Song MH. Noninvasive quantification of bowel inflammation through positron emission tomography imaging of 2-deoxy-2-[18F] fluoro-D-glucose-labeled white blood cells. Mol Imaging Biol 2003;5:271–7.
Nolan DJ. The small intestine. In: Grainger RG, editor. Grainger and Allison’s text book of diagnostic radiology. 4th ed. London: Churchill Livingstone; 2001. pp. 1075–98.
Towson JEC. Radiation protection and dosimetry in PET and PET/CT. In: Valk PE, Bailey DL, Townsend DW, Maisey MN, editors. Positron emission tomography basic science and clinical practice. London: Springer; 2003. pp. 265–82.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial disclosure:
All the authors of this study declare no conflict of interest and financial obligation.
Rights and permissions
About this article
Cite this article
Das, C.J., Makharia, G., Kumar, R. et al. PET-CT enteroclysis: a new technique for evaluation of inflammatory diseases of the intestine. Eur J Nucl Med Mol Imaging 34, 2106–2114 (2007). https://doi.org/10.1007/s00259-007-0525-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-007-0525-z