
Background and Purpose:
Different factors influence glioblastoma patients' prognosis. The aim of this retrospective, explorative analysis was to define the role of recent treatment strategies and to examine the value of different prognostic factors.
Patients and Methods:
A total of 110 patients was analyzed. Complete resection, partial resection, and biopsy was accomplished in 69, 22, and 19 patients, respectively. 56 patients received conventionally fractionated radiotherapy with a median total dose of 60 Gy, 2 Gy daily. 54 patients received hyperfractionated accelerated radiotherapy with a median total dose of 54 Gy, 2 × 1.8 Gy daily. 20 patients had concomitant temozolomide (50–75 mg/m2/d), and 20 patients concomitant topotecan (0.5 mg/m2 as continuous venous infusion over 21 days). 37 patients received temozolomide as salvage therapy.
Results:
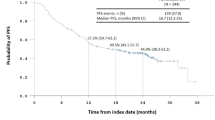
Median overall (OS) and disease-free survival (DFS) were 8.7 and 4.8 months. After complete resection, partial resection, and biopsy, OS was 9.5, 8.5, and 5.5 months, respectively. OS was 8.5, 13.8, and 8.2 months for radiotherapy alone, concomitant temozolomide, and concomitant topotecan, respectively. Hazard ratio was 0.29 (OS; p = 0.002) and 0.32 (DFS; p = 0.003) for concomitant temozolomide compared to radiotherapy alone. Topotecan led to an increased toxicity. With 9.7 months for conventionally fractionated radiotherapy and 8.1 months for hyperfractionated radiotherapy, OS differed significantly (p = 0.003, log-rank test). OS in patients with RPA (recursive partitioning analysis) score III, IV, V, and VI was 14.1, 10, 9.5, and 5.8 months (p = 0.003, log-rank test). In the univariate (p = 0.0001, log-rank test) and multivariate analysis (p = 0.002, Cox regression), salvage temozolomide led to a statistically significant survival benefit (10.6 vs. 7.7 months).
Conclusion:
Concomitant topotecan or the use of hyperfractionated radiotherapy did not show to be superior in outcome in this retrospective analysis. Topotecan led to an increased toxicity. An attempt at complete resection is justified. Temozolomide should be integrated in therapy initially. As salvage therapy, temozolomide is also effective.
Hintergrund und Ziel:
Verschiedene therapie- und patientenbezogene Faktoren beeinflussen die Prognose von Glioblastompatienten. Das Ziel dieser retrospektiven, explorativen Analyse war, die Rolle verschiedener Behandlungsstrategien und den Wert unterschiedlicher prognostischer Parameter zu untersuchen.
Patienten und Methodik:
110 Patienten gingen in die Analyse ein. Eine komplette Resektion, eine partielle Resektion und eine Biopsie erhielten 69, 22 und 19 Patienten. Bei 56 Patienten wurde eine konventionell fraktionierte Bestrahlung mit 2 Gy täglich, mediane Gesamtdosis 60 Gy, und bei 54 Patienten eine hyperfraktioniert-akzelerierte Bestrahlung mit 2 × 1,8 Gy täglich, ad 54 Gy, durchgeführt. Jeweils 20 Patienten erhielten simultan Temozolomid (50–75 mg/m2/d) oder Topotecan (0,5 mg/m2, kontinuierlich i.v. über 21 Tage). 37 Patienten erhielten eine Rezidivtherapie mit Temozolomid.
Ergebnisse:
Medianes Gesamtüberleben (OS) und rezidivfreies Überleben (DFS) lagen bei 8,7 und 4,8 Monaten. Nach kompletter Resektion, partieller Resektion und Biopsie lag das OS bei 9,5, 8,5 und 5,5 Monaten. Nach alleiniger Radiotherapie, simultaner Temozolomid- und Topotecanapplikation betrug das OS 8,5, 13,8 und 8,2 Monate. Die simultane Gabe von Temozolomid führte zu einer signifikanten Risikoreduktion bezüglich des OS (Hazard-Ratio 0,29; p = 0,002) und des DFS (Hazard-Ratio 0,32; p = 0,003). Unter paralleler Topotecangabe zeigte sich eine erhöhte Toxizität (45% Grad 3/4). Das OS lag nach hyperfraktionierter gegenüber konventionell fraktionierter Radiotherapie signifikant niedriger (8,1 vs. 9,7 Monate; p = 0,003, Log-Rank-Test). Für Patienten mit einem RPA-Score („recursive partitioning analysis“) von III, IV, V und VI lag das OS bei 14,1, 10, 9,5 und 5,8 Monaten (p = 0,003, Log-Rank-Test). Eine Salvage-Therapie mit Temozolomid führte, univariat (p = 0,0001, Log-Rank-Test) wie auch multivariat (p = 0,002) analysiert, zu einem signifikanten Überlebensvorteil (10,6 vs. 7,7 Monate).
Schlussfolgerung:
Eine parallele Topotecangabe oder eine Hyperfraktionierung führte in dieser retrospektiven Analyse nicht zu einer Prognoseverbesserung. Unter simultanem Topotecan stieg die Toxizität deutlich an. Eine komplette Resektion sollte versucht werden. Temozolomid ist ein wichtiger Bestandteil des Therapiekonzepts. Auch in der Rezidivsituation ist Temozolomid effektiv.
Similar content being viewed by others


Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Piroth, M.D., Gagel, B., Pinkawa, M. et al. Postoperative Radiotherapy of Glioblastoma Multiforme. Strahlenther Onkol 183, 695–702 (2007). https://doi.org/10.1007/s00066-007-1739-5
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00066-007-1739-5