

Abstract
The diagnosis of spondylodiskitis is often challenging. MRI is quite sensitive but lacks specificity, and distinction from erosive osteochondritis is often difficult. We sought to assess the diagnostic value of 18F-FDG PET combined with MRI (combined 18F-FDG PET/MRI) in patients with suspected spondylodiskitis and an inconclusive clinical or MRI presentation. Methods: In a prospective study, 30 patients with previous inconclusive MRI results and suspected spondylodiskitis underwent combined 18F-FDG PET/MRI, including precontrast and postcontrast standard spine MRI sequences. The image datasets were evaluated on dedicated workstations by 2 radiology residents and 1 board-certified nuclear medicine physician independently and then in consensus. Because of severe susceptibility artifacts, only 28 of 30 image datasets were evaluable, with a total of 29 regions of suspected spondylodiskitis. SUV ratios (affected disk/reference disk) were determined. The imaging results were compared with histopathology or clinical follow-up as a reference standard and subjected to statistical analysis. Results: The reference standards identified spondylodiskitis in 12 disks and excluded spondylodiskitis in 17 disks. For MRI alone, the sensitivity was 50%, the specificity was 71%, the positive predictive value was 54%, and the negative predictive value was 67%. Adding the PET data resulted in sensitivity, specificity, positive predictive value, and negative predictive value of 100%, 88%, 86%, and 100%, respectively. In a receiver operating characteristic curve analysis, an SUVmax ratio threshold of 2.1 resulted in 92% sensitivity and 88% specificity (area under the receiver operating characteristic curve, 0.95). Neither the level of C-reactive protein nor the leukocyte count at the time of PET/MRI was related to the reference standard diagnosis of spondylodiskitis. Conclusion: In patients with inconclusive clinical or MRI findings, the use of 18F-FDG PET/MRI significantly increased diagnostic certainty for the detection of spondylodiskitis.
- spondylodiskitis
- 18F-FDG PET/MRI
- PET
- MRI
- osteochondritis
Spondylodiskitis, also known as vertebral osteomyelitis, is a rare but serious destructive infection of the vertebral bodies with involvement of the intervertebral disks. The incidence of this disease is increasing, possibly because of the growing elderly population with chronic and degenerative diseases. Additionally, increases in spinal surgery and instrumentation, in the use of immunosuppressive agents, and in intravenous drug abuse have defined additional risk groups (1,2). Although the mortality from spondylodiskitis has been reported to be less than 5%, the morbidity is high; vertebral infections can result in bone destruction, and the involvement of disks can lead to further instability, chronic back pain, and neurologic deficits.
In addition to clinical examination—including a detailed evaluation of neurologic status, blood samples, or vertebral biopsies—radiologic and nuclear medicine imaging techniques—including conventional radiography, CT, MRI, multiphase bone scintigraphy, leukocyte scintigraphy, PET with 18F-FDG, or PET/CT—have been used. PET/MRI became available only recently, and the determination of its usefulness for imaging spondylodiskitis awaits systematic testing (3–5).
Depending on the disease stage, strict conservative or operative treatment is required for a desirable outcome. Early detection is obviously desirable but often challenging because of nonspecific clinical, laboratory, and radiologic findings.
In the early stages, MRI is currently the method of choice for diagnosing spondylodiskitis, with a reported sensitivity of 96% (2,6,7). MRI can depict the anatomic location and the extent of disease and allows the early detection of disk or bone destruction as well as evaluation of the involvement of neural structures (8). The classic MRI findings of spondylodiskitis are hyperintense signal alterations on T2-weighted images or turbo inversion recovery magnitude (TIRM) sequences in the disk space (often with fluid collections), appearing in both adjacent vertebrae as bone marrow and paravertebral soft-tissue edema. On T1-weighted images, the lesions appear with decreased signal intensity on noncontrast images, with marked contrast enhancement (2,6,9). However, similar findings in the presence of fractures or spinal implants may lead to insufficient specificity. Another well-known MRI problem is the distinction of infectious spondylodiskitis from erosive osteochondritis with Modic type 1 changes, as these entities share similar signal alterations (10,11).
In these equivocal cases, nuclear medicine imaging techniques may play a useful role. Among the nuclear medicine imaging tools mentioned earlier, 18F-FDG PET, with a reported sensitivity of 82%, is useful for detecting or especially excluding spondylodiskitis. Therefore, 18F-FDG PET can differentiate active inflammation and degenerative alterations, such as erosive osteochondritis. 18F-FDG PET/CT or 18F-FDG PET combined with MRI has been shown to have higher diagnostic accuracy than either modality performed alone (12,13) because the combined modalities can overcome the limited spatial resolution of 18F-FDG PET and its limited ability to differentiate between inflammation and malignant tissue (3,4,14).
The combination of the strengths of 18F-FDG PET and MRI in 18F-FDG PET/MRI offers a new type of hybrid imaging that provides highly sensitive metabolic and high-resolution anatomic imaging with excellent soft-tissue contrast. However, this method has not yet been investigated in spondylodiskitis. The aim of our study was to analyze the additive value of MRI performed simultaneously with18F-FDG PET (18F-FDG PET/MRI) in patients with suspected spondylodiskitis and inconclusive findings on clinical examination and MRI alone.
MATERIALS AND METHODS
Patients
In this prospective single-center study, 34 consecutive patients (14 men and 20 women; mean ± SD age, 72 ± 11 y; age range, 49–94 y) with clinically or paraclinically suspected spondylodiskitis with a duration of less than 4 wk were enrolled between March 2014 and August 2015. Informed consent for the use of 18F-FDG and the MRI contrast agent gadobutrol (Gadovist; Bayer Healthcare) was obtained from all patients. This study was approved by the Ethics Committee of the Medical Faculty, University of Leipzig, Leipzig, Germany, and all patients gave written informed consent.
All patients had previously undergone MRI, with results that were either inconclusive or suggestive of spondylodiskitis. In 30 of 34 patients, combined 18F-FDG PET/MRI, including whole-spine 3-T MRI with standard sequences before and after contrast agent administration, was performed. Four patients interrupted the examination because of severe back pain and restlessness.
Whole-Body PET/MRI Protocol
The combined PET/MRI system (mMR-Biograph; Siemens Healthcare) used in this study has a 3-T MRI scanner and an integrated PET scanner.
Whole-body sequential PET/MRI scanning was performed from the upper thigh to the skull with a 5-min acquisition time per bed position. After a fasting period of at least 6 h, image acquisition commenced an average of 75 min (range, 60–105 min) after the intravenous administration of 18F-FDG (4 MBq/kg; range, 149–410 MBq; mean ± SD, 294 ± 64 MBq).
PET images were reconstructed by use of the iterative ordered-subset expectation maximization algorithm with 3 iterations and 21 subsets, a gaussian filter with 4-mm full width at half maximum, and a 256 × 256 image matrix. Attenuation correction of the PET data was performed with a 4-tissue (fat, soft-tissue, air, and background) model attenuation map obtained from a Dixon–volume-interpolated breath-hold examination MR sequence.
Subsequently, whole-spine MRI data were obtained with the integrated spine coil and 2 body phased-array coils covering the region from the occiput to the coccyx in 3 bed positions: cervical, thoracic, and lumbar. Typical sequences were acquired (Table 1).
MRI Sequence Parameters Used in Combined Whole-Body PET/MRI
For contrast-enhanced MRI, a single gadobutrol dose of 0.1 mmol/kg, at a rate of 3 mL/s and flushed with 10 mL of saline, was administered with a power injector (Spectris Solaris; Medrad/Bayer Healthcare).
Image Interpretation
The PET/MRI datasets were evaluated on dedicated workstations (PET/MRI: Syngo.via [Siemens Healthcare]; MRI alone: MagicView 1000 [Siemens Healthcare]). Focal 18F-FDG uptake in spinal disks greater than that in the surrounding tissue (on the basis of a visual qualitative analysis) was considered to be suggestive of spondylodiskitis. For each affected intervertebral disk identified by the TIRM MRI sequence, SUVmean and SUVmax were determined by identifying the disk in the fused PET/MRI dataset and by placing a volume of interest around the disk (SUVmax threshold, 40%). Using this method, we could determine that only disk tissue was part of the volume of interest and exclude artifacts from adjacent osseous processes.
SUVmean and SUVmax were also determined for a healthy reference disk, and SUV ratios (affected disk/reference disk) were calculated.
The datasets for MRI alone from PET/MRI were analyzed independently and in consensus by 2 radiologists with 1.5 y and 5 y of experience using a 5-point Likert scale (where 1 means “spondylodiskitis definitely absent,” 2 means “spondylodiskitis probably absent,” 3 means “neutral,” 4 means “spondylodiskitis probably present,” and 5 means “spondylodiskitis definitely present”). This step was followed by an interdisciplinary analysis—which included a board-certified nuclear medicine physician (8 y of experience in PET image interpretation)—of the complete PET/MRI datasets; this analysis resulted in a consensus decision, dichotomized into “spondylodiskitis” and “no spondylodiskitis.” Except for knowledge about the painful spine level, the interpreters were unaware of the laboratory parameters and histologic results.
Reference Standards
The imaging results were compared with the results of a histopathologic evaluation of surgery or biopsy specimens (n = 6) or clinical follow-up (n = 22) as reference standards. Spondylodiskitis was excluded by clinical follow-up if symptoms were absent or regressed without antibiotic therapy and if inflammation parameters, including white blood cell count and C-reactive protein (CRP) level, were in the reference range (<5 mg/L) or were at a very low level that did not progress during a follow-up period of at least 6 wk. Spondylodiskitis was confirmed by clinical follow-up when signs of inflammation and pain regressed after antibiotic therapy or progressed without antimicrobial therapy during a period of at least 6 wk.
Indications for operative treatment would have been large paraspinal abscesses, sepsis, progressive neurologic impairment, deformities due to destruction of the endplates, and failure of 6 wk of antibiotic treatment. Conservative treatment was used in patients with an aseptic paraclinical constellation, low pain levels, and no vertebral destructive changes on PET/MRI.
Statistical Analysis
The nonparametric Mann–Whitney U test was performed, and interrater agreement was established with a linearly weighted Cohen κ-coefficient.
Diagnostic certainty was determined as the sum of true-positive and true-negative results divided by all results and was reported as a percentage.
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and positive and negative likelihood ratios were calculated for both imaging modalities. The exact McNemar test was used for sensitivity and specificity comparisons.
Correlations between SUVmean or SUVmax and laboratory parameters (CRP level and white blood cell count) were calculated as the Spearman ρ. Receiver operating characteristic curve analysis was performed to assess the diagnostic performance of PET/MRI, and the maximum Youden index was determined to define the optimal cutoff value for the SUV ratio.
If not otherwise indicated, data are given as mean ± SD for quantitative variables. Statistical significance for all tests was set at a P level of less than 0.05. Statistical analysis was done with commercial software (SPSS version 22.0 software package; SPSS Inc.).
RESULTS
The whole-body PET/MRI examination was successfully completed in 30 of 34 patients. In 5 of 30 patients, internal fixation material was found at the level of interest, causing susceptibility artifacts on MR images. Because of severe susceptibility artifacts in 2 of 5 patients, the assessment was significantly restricted on MR images as well on 18F-FDG PET images, and a final evaluation could not be realized. In the other 3 patients, MR images were not evaluable, but a consensus final imaging diagnosis could be made from the PET information.
In total, 28 patients (18 women [64%] and 10 men [36%]) with 29 regions of suspected spondylodiskitis were evaluated (Table 2). Figures 1 and 2 show typical imaging findings. Evaluation of the MRI portion of PET/MRI resulted in 6 of 29 regions with a diagnosis of spondylodiskitis and in 15 of 29 regions with a diagnosis of no spondylodiskitis (Supplemental Table 1) (supplemental materials are available at http://jnm.snmjournals.org). The results for 8 of 29 regions remained inconclusive on MRI. Interrater agreement between the 2 MRI interpreters was moderate, with a weighted Cohen κ of 0.66. When PET information was added, the inconclusive diagnosis changed to spondylodiskitis for 5 of 8 regions and to no spondylodiskitis for 3 of 8 regions. In total, by PET/MRI consensus decision, spondylodiskitis was diagnosed for 14 of 29 regions and excluded for 15 of 29 regions. There were no inconclusive decisions.
Characteristics of 28 Patients with 29 Regions of Suspected Spondylodiskitis
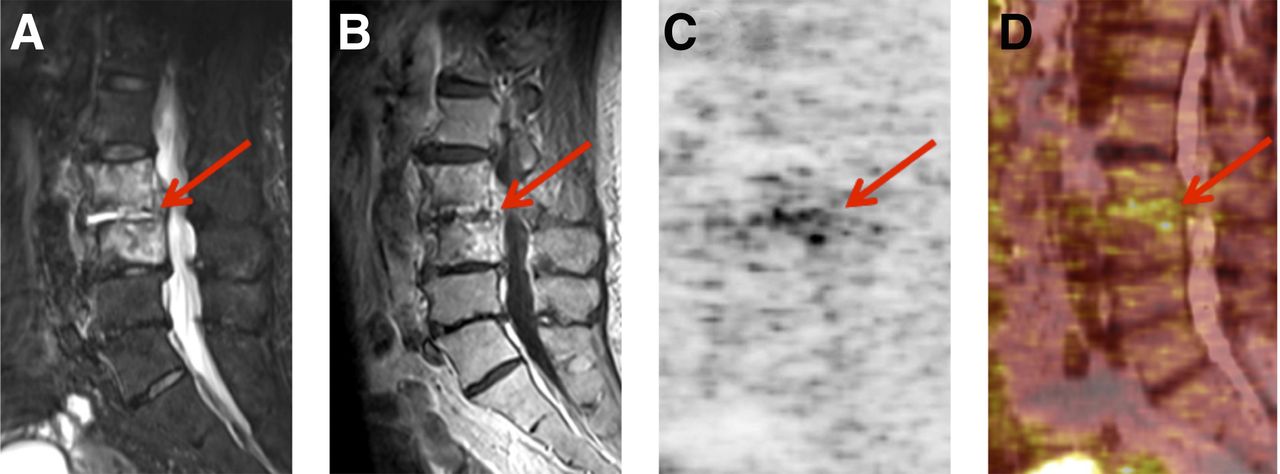
Simultaneous 18F-FDG PET/MRI in 71-y-old female patient with final diagnosis of spondylodiskitis. MRI alone was inconclusive. (A) TIRM with typical hyperintense signal alterations at intervertebral disk level L4–L5 (arrow). (B) Moderate postcontrast signal (arrow) on T1-weighted MRI. (C and D) 18F-FDG PET (C) and combined 18F-FDG PET/MRI (D) show focally elevated uptake in affected disk (arrow; SUVmax, 8.14; SUVmean, 3.99) as sign of active inflammation.

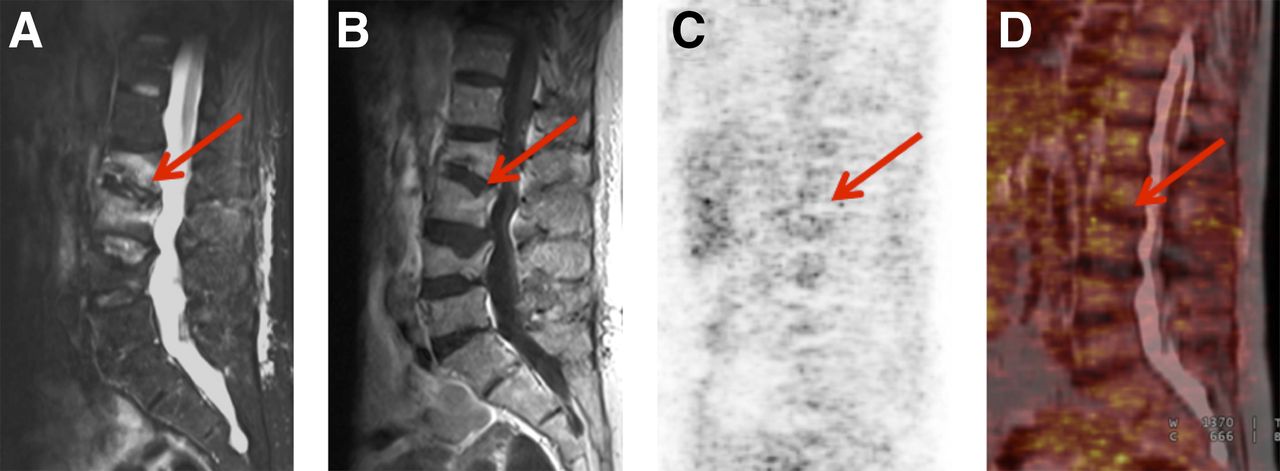
Simultaneous 18F-FDG PET/MRI in 59-y-old female patient with suspected spondylodiskitis at level L2–L3 and final diagnosis of no spondylodiskitis but postfracture changes. MRI alone was inconclusive. (A) TIRM with typical hyperintense signal alterations at intervertebral disk level L2–L3 (arrow). (B) Poor postcontrast signal (arrow) on T1-weighted MRI. (C and D) 18F-FDG PET (C) and fused 18F-FDG PET/MRI (D) show no elevated tracer uptake in disk with suspected spondylodiskitis (arrow; SUVmax, 3.08; SUVmean, 1.77); therefore, active inflammation was excluded.
Histologic confirmation after surgery or percutaneous biopsy was available in 6 of 28 patients. In the remaining 22 patients, clinical follow-up was used as a reference standard to prove or exclude spondylodiskitis.
With the reference standard, 12 cases of spondylodiskitis were finally diagnosed—4 by histopathologic results and 8 by clinical follow-up. In 1 case, the cervical spine was affected; the lumbar spine was involved in the other 11 cases (Table 2). In 17 of 29 spinal regions, spondylodiskitis was excluded (2 by histopathologic results and 15 by clinical follow-up).
Between patients with spondylodiskitis and those without spondylodiskitis there were no significant differences concerning sex, age, CRP level, or leukocyte count (P > 0.05) (Table 2). For MRI, the sensitivity was 50%, the specificity was 71%, the PPV was 54%, and the NPV was 67%. When the PET component was added, the sensitivity, specificity, PPV, and NPV for the PET/MRI data improved, to 100%, 88%, 86%, and 100%, respectively (Table 3). With combined PET/MRI, there were no false-negative results. Diagnostic certainty was significantly higher with combined PET/MRI than with MRI alone (93.1% vs. 62.1%; P < 0.001).
Diagnostic Comparison of MRI Alone and Combined 18F-FDG PET/MRI for Diagnosis of Spondylodiskitis
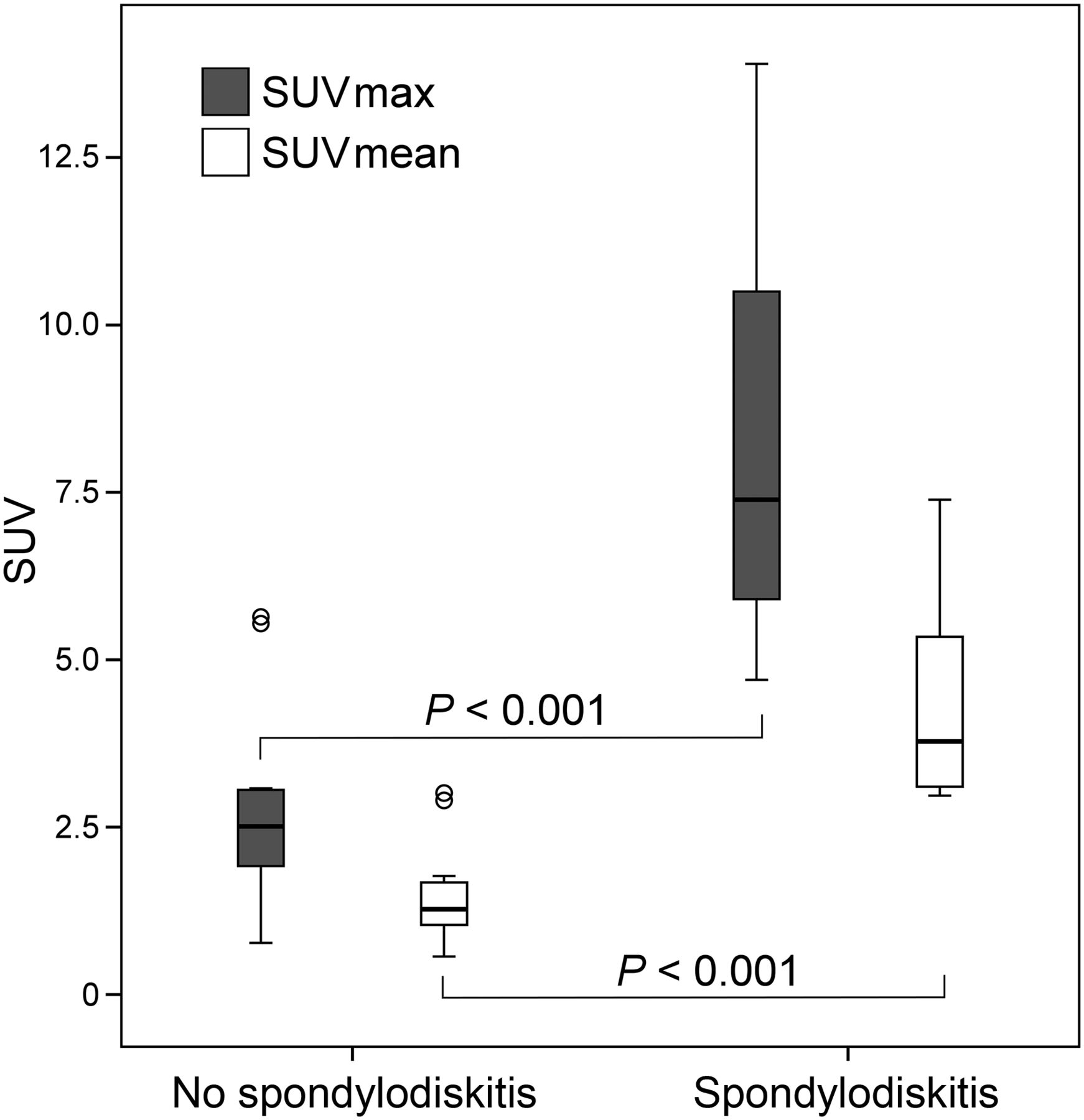
In the receiver operating characteristic curve analysis, an SUVmax ratio threshold of 2.1 resulted in 92% sensitivity and 88% specificity for the correct diagnosis of spondylodiskitis (area under the curve of 0.95) (Fig. 3). In patients with spondylodiskitis, the absolute SUVmax and SUVmean in the affected disk were significantly elevated (SUVmax, 5.07 ± 3.43; SUVmean, 2.68 ± 1.76), compared with the findings in patients with no spondylodiskitis (SUVmax, 2.73 ± 1.29; SUVmean, 1.46 ± 0.67) (P < 0.001) (Fig. 4). There was a significant correlation of the level of CRP with the SUVmax of the affected disk (Spearman ρ, 0.5; P = 0.01) but not with the SUVmax ratio (P = 0.09).

Receiver operating characteristic curve analysis of SUVmax ratio for differentiation of spondylodiskitis and no spondylodiskitis on combined 18F-FDG PET/MRI. SUVmax ratio threshold of 2.1 resulted in 92% sensitivity and 88% specificity for correct diagnosis of spondylodiskitis (area under curve, 0.95).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
18F-FDG PET SUVmax and SUVmean relative to reference standard diagnosis. Ends of boxes represent 25th and 75th percentiles (or first and third quartiles), and center line represents median. 75th percentile minus 25th percentile equals interquartile range (IQR), and ends of whiskers are placed at 1.5 times IQR. Any values lying outside these boundaries are considered outliers.
The results for the MRI portion of 18F-FDG PET/MRI were false-positive in 5 patients—in 2 patients because of osteochondritis, in 1 patient because of spondylitis, in 1 patient because of degenerative disk space narrowing, and in 1 patient because of fracture-associated signal alterations. 18F-FDG PET/MRI results were false-positive in 2 patients; 1 patient had spondylitis, and in the other, erosive osteochondritis was diagnosed by clinical follow-up.
Other main diagnoses in patients without spondylodiskitis were fractures, herniated disks, and spondylolisthesis.
DISCUSSION
The diagnosis of spondylodiskitis usually requires multiple modalities, including clinical examination, laboratory tests (including blood cultures), a combination of imaging techniques, and biopsy samples for pathogen detection. Because of a high reported sensitivity (up to 96%), MRI is currently the method of choice for diagnosing spondylodiskitis, especially in its early stages. Furthermore, MRI is widely available and radiation-free. Compared with CT, MRI is superior in distinguishing bone marrow, vertebrae, intervertebral disks, and neural structures. Nevertheless, there are limitations, especially in patients who have undergone surgery and have metallic implants, which may cause severe susceptibility artifacts. Furthermore, differentiation from degenerative processes, such as erosive osteochondritis, may be difficult with MRI. In these cases, 18F-FDG PET has been reported to be a useful tool for differentiating degenerative from infectious endplate abnormalities found on MRI. However, a lack of anatomic detail and a limited spatial resolution are the main drawbacks of 18F-FDG PET (6,7,15,16).
With the recent development of integrated PET/MRI scanners, new possibilities for multimodal molecular imaging have emerged. PET/MRI and the application of the one-stop-shop principle enable the analysis of simultaneously acquired metabolic and morphologic parameters with excellent soft-tissue contrast and, therefore, may improve diagnostic capabilities in inflammatory processes and other disease entities (3). Besides the improvements in time and patient comfort achieved by use of a single image examination with simultaneous PET/MRI (one-stop-shop), an advantage of simultaneous PET/MRI over sequentially performed PET and MRI is the added value of the excellent soft-tissue contrast of MRI. The main drawback of a single PET scan is the lack of anatomic information, making the distinction between disk and bone tissue difficult. Especially in the setting of spondylodiskitis, often with nearly completely destroyed disks, the distinction between diskitis and spondylitis is nearly impossible without the simultaneously acquired MRI dataset.
Regarding the diagnosis of spondylodiskitis with combined 18F-FDG PET/MRI, the scientific literature is still limited. In a metaanalysis performed by Prodromou et al. (14), diagnostic data on the use of 18F-FDG PET for spondylodiskitis in 12 studies comprising 224 patients were evaluated. The combined sensitivity across these studies was 0.97, and the specificity was 0.88. The authors concluded that 18F-FDG PET is a robust diagnostic test when spondylodiskitis is suspected and is an excellent tool for the exclusion of infectious spondylodiskitis.
In another study, Skanjeti et al. (17) retrospectively included 33 patients with suspected or confirmed spondylodiskitis and compared the usefulness of 18F-FDG PET in the diagnostic work-up of patients with spondylodiskitis with that of MRI alone. For diagnosing spondylodiskitis, the sensitivity, specificity, PPV, NPV, and accuracy of 18F-FDG PET were 92.9%, 50%, 72.2%, 83.3%, and 75%, respectively; for MRI alone, the sensitivity, specificity, PPV, NPV, and accuracy were 100%, 50%, 76.9%, 100%, and 81.3%, respectively. These results indicated similar accuracies of 18F-FDG PET and MRI. Therefore, those authors recommended the use of 18F-FDG PET when MRI is doubtful or unavailable.
Similar accuracies of MRI alone and 18F-FDG PET/CT for diagnosing spondylodiskitis (81% and 84%, respectively) were also reported in a study by Fuster et al. (8). However, that study of 26 prospective patients demonstrated a low specificity (38%) of MRI, reflecting the difficulty in the exclusion of infectious spondylodiskitis.
The present study—which is, to the best of our knowledge, the first study in which combined 18F-FDG PET/MRI has been used for the detection of spondylodiskitis—demonstrated significant improvements in sensitivity, specificity, PPV, and NPV—up to 100%, 88%, 86%, and 100%, respectively—when the PET component was added to the MRI assessment. Compared with the results of other studies (2,6,7), the sensitivity and specificity (50% and 70.6%, respectively) of the MRI portion of combined PET/MRI in the present study seem to be low. We focused on diagnostically difficult cases (patients with inconclusive findings on previously performed MRI). Diagnostic certainty was significantly higher with combined PET/MRI than with MRI alone. The results of the present study also reflected the difficulty of using MRI alone for the exclusion of spondylodiskitis, as indicated by false-positive results in 5 patients because of osteochondritis, spondylitis, degenerative disk space narrowing, and fractures.
With combined PET/MRI, there were no false-negative results, indicating that combined 18F-FDG PET/MRI may be most useful in patients with suspected spondylodiskitis and inconclusive MRI findings. The results of simultaneous 18F-FDG PET/MRI were false-positive in 2 patients, who had spondylitis and erosive osteochondritis. Both patients showed focally elevated 18F-FDG uptake as well as hyperintense T2-weighted and hypointense T1-weighted MRI signals. These MRI signal patterns can also be found in inflammatory processes and degenerative diseases (11,18,19).
Ohtori et al. (12) and Gratz et al. (20) recommended 18F-FDG PET for distinguishing between active inflammation of the spine and degenerative changes. Their findings were confirmed by the present study, as active inflammation was correctly excluded by 18F-FDG PET/MRI in 3 of 4 patients with erosive osteochondritis. Frequent causes of false-positive findings for 18F-FDG PET are healing bone and adjacent tissues after trauma or manipulation after surgery or biopsy (21,22). The induced signal patterns are part of inflammatory processes and can imitate those of primary infections (23). Nevertheless, in those cases (12,20), no histopathologic results were available as a gold standard, so a low level of uncertainty remains.
In contrast to what is seen for CT and MRI, 18F-FDG uptake in PET is not hampered or is minimally hampered by metallic implant–associated artifacts. Therefore, combined 18F-FDG PET/MRI may be advantageous in spondylodiskitis patients with susceptibility artifacts. In the present study, internal fixation material was found at the spine level of interest in 5 patients, rendering the MRI data nonevaluable. Nevertheless, in 3 of the 5 patients, a consensus final imaging diagnosis was achieved as a result of the additional PET information. In the remaining 2 patients, a final evaluation could not be realized because of severe susceptibility artifacts in the region of suspected spondylodiskitis.
Similar to the data of Fuster et al. (8), who demonstrated a statistically significant difference in mean SUVmax between infected and noninfected spondylodiskitis patients (SUVmax, 6.5 and 3.6, respectively), the semiquantitative assessment of 18F-FDG PET in the present study demonstrated significant differences in the absolute SUVmean and SUVmax between affected and nonaffected (i.e., no spondylodiskitis) disks. Additionally, an SUVmax ratio threshold of 2.1 resulted in 92% sensitivity and 88% specificity for the correct diagnosis of spondylodiskitis. For further evaluation of spondylodiskitis patients, these data may help improve discrimination between infected and noninfected spinal disks. As described by Nakahara et al. (13), accurate delineation of areas of active spondylodiskitis infection may also be useful for narrowing the surgical field.
In the present study, the absolute SUVmean and SUVmax were significantly correlated with the level of CRP. However, there were no significant differences in leukocyte count or CRP level between patients with spondylodiskitis and those without spondylodiskitis. Clinical and paraclinical courses as well as imaging patterns of degenerative diseases and low-grade infections can be very similar (11). It is well known that inflammatory markers do not serve as pathognomonic parameters for diagnosing spondylodiskitis (24,25).
A limitation of the present study was the lack of histopathology in all patients because surgery or biopsy was performed in only 6 patients. Some uncertainty remains in the cases with clinical follow-up.
Future spondylodiskitis imaging research should focus on a possible role of 18FDG PET/MRI in early assessment of the response to antibiotic therapy. As demonstrated by Skanjeti et al. (17), 18F-FDG PET was more accurate and more specific than MRI in an assessment of treatment for spondylodiskitis, suggesting that 18F-FDG PET should be preferred over MRI for determining when treatment can be safely discontinued.
Similar results were reported by Nanni et al. (26), who analyzed data from 34 spondylodiskitis patients and determined the SUVmax of a baseline 18F-FDG PET/CT examination (SUV1) and of a second 18F-FDG PET/CT examination after 2–4 wk of therapy (SUV2). 18F-FDG PET was found to be a useful tool for identifying responders. The use of a change in the SUVmax provided the highest sensitivity and specificity (82%) for identifying responders; in contrast, the sensitivity of a change in the CRP level during therapy was only 67%. According to these results, a decrease in the SUVmax of at least 34% is strongly predictive of a complete response. These data may have a strong impact on the clinical management of spondylodiskitis because the initial CRP level is known to be a false-negative finding in a significant percentage of patients.
CONCLUSION
The use of combined 18F-FDG PET/MRI significantly increased diagnostic certainty for the detection of spondylodiskitis, especially in cases with inconclusive MRI findings. Combined 18F-FDG PET/MRI had 100% sensitivity and may be most relevant for the detection of early cases of spondylodiskitis. With this one-stop-shop approach, improved diagnostic certainty and—if needed—the possibility of earlier initiation of proper treatment are the main benefits for spondylodiskitis patients.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
* Contributed equally to this work.
Published online May 19, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- Received for publication December 19, 2015.
- Accepted for publication March 29, 2016.