

Abstract
6-18F-fluorodopa PET depicts the striatal dopaminergic lesion characterizing Parkinson disease (PD); however, striatal uptake of 6-18F-fluorodopa–derived radioactivity can be normal. Supine hypertension (SH) might increase 6-18F-fluorodopa uptake. Methods: We measured putamen, caudate, and occipital cortex 6-18F-fluorodopa–derived radioactivity and supine blood pressure in patients with PD + SH (systolic pressure ≥ 180 mm Hg, n = 8), patients with PD without SH (PD − SH, n = 19), patients with pure autonomic failure (n = 8), and controls (n = 16). Results: Peak putamen radioactivity correlated with supine systolic pressure across all subjects and among PD patients and was higher in PD + SH than in PD − SH (P = 0.01). Both subgroups had rapid fractional declines in radioactivity between the peak and late values (P < 0.0001, compared with controls). Arterial 6-18F-fluorodopa concentrations were similar in the compared groups. Conclusion: In PD, SH is associated with augmented striatal 6-18F-fluorodopa–derived radioactivity. Regardless of SH, retention of 6-18F-fluorodopa–derived radioactivity is markedly reduced. A model-independent approach can identify striatal dopaminergic denervation in PD.
- fluorodopa
- Parkinson
- pure autonomic failure
- orthostatic hypotension
- supine hypertension
PET scanning after intravenous 6-18F-fluorodopa administration provided the first in vivo depiction of the nigrostriatal dopaminergic lesion that characterizes Parkinson disease (PD) (1–3).
It became apparent early on that striatal uptake and peak concentrations of 6-18F-fluorodopa–derived radioactivity can be normal in PD (4). Investigators therefore have applied models based on differential kinetics of radioactivity in dopaminergic and nondopaminergic intracerebral compartments or have used the ratio of 6-18F-fluorodopa–derived radioactivity in the striatum (the putamen and caudate) to that in the cerebellum, occipital cortex, or other control regions devoid of dopaminergic innervation.
Here we provide evidence that a previously unrecognized factor—blood pressure—influences cerebral 6-18F-fluorodopa–derived radioactivity. We came to consider such an influence after comparing PD subgroups with versus without neurogenic orthostatic hypotension. Despite similar severities of parkinsonism, the subgroup with neurogenic orthostatic hypotension had higher putamen 6-18F-fluorodopa–derived radioactivity at all time points than did the subgroup without neurogenic orthostatic hypotension (David S. Goldstein, unpublished data, November 2008). Neurogenic orthostatic hypotension is associated with sometimes severe supine hypertension (SH) (5,6), which might augment cerebral 6-18F-fluorodopa uptake by overcoming cerebrovascular autoregulation or disrupting the blood–brain barrier.
In the present study, we measured concentrations of 6-18F-fluorodopa–derived radioactivity in the putamen, occipital cortex, and caudate and 6-18F-fluorodopa in arterial plasma in subgroups of PD patients who either had or did not have severe SH (supine systolic blood pressure ≥ 180 mm Hg). Comparison groups included patients with pure autonomic failure (PAF) (a Lewy body disease characterized by neurogenic orthostatic hypotension without parkinsonism) and control subjects.
MATERIALS AND METHODS
The subjects in this study gave informed written consent before participating in protocols approved by the Institutional Review Board of the National Institute of Neurological Disorders and Stroke. All studies were performed in the Clinical Center of the National Institutes of Health.
The 6-18F-fluorodopa PET results were reviewed for a total of 51 subjects. There were 27 patients with PD, including 8 with severe SH; 8 patients with PAF; and a control group of 16 subjects, including 8 patients without orthostatic hypotension or PD and 8 middle-aged, healthy volunteers. The clinical diagnosis was supported in each case by the results of cardiac 6-18F-fluorodopamine scanning (7).
Orthostatic hypotension was defined by a fall in systolic pressure of at least 20 mm Hg and in diastolic pressure of at least 10 mm Hg between supine rest for at least 15 min and upright posture for 5 min (unless symptomatic or rapid hypotension necessitated an earlier return to the supine position).
For 6-18F-fluorodopa brain PET, the subject was placed supine headfirst in an Advance scanner (GE Healthcare). Seven millicuries of 6-18F-fluorodopa were infused intravenously over 3 min using an automated syringe pump. Carbidopa pretreatment was not used. In subjects undergoing measurements of arterial plasma concentrations of 6-18F-fluorodopa, a brachial arterial catheter was inserted after local anesthesia of the overlying skin. In most subjects, after the initial static scan had been obtained, the head was scanned in a high-resolution research tomograph. The high-resolution research tomograph produces 207 slices per 3-dimensional data frame, compared with 35 on the Advance scanner, and reconstructed image resolution is 2.5–3 mm, compared with 6–7 mm. Emission data in the high-resolution research tomograph were obtained for 15 min. A final 15-min static scan was obtained in the Advance scanner, ending about 120 min from the time of the beginning of the 6-18F-fluorodopa infusion (midpoint, ∼112 min).
6-18F-fluorodopa brain PET and individual MRI scans were fused using PMOD (PMOD Technologies Ltd.). Regions of interest were placed manually at the perimeters of the putamen, head of the caudate, and occipital cortex on the MRI scans. Tissue concentrations of 6-18F-fluorodopa–derived radioactivity (in nCi/cm3) were adjusted for the dose per unit body mass and expressed in units of kBq-kg/cm3·mCi.
Data were analyzed by factorial analyses of variance with the Fisher protected-least-significant-difference post hoc test, independent means t tests, and linear regression, using KaleidaGraph 4.0.1 (Synergy Software).
RESULTS
The PD + SH subgroup averaged more than a decade older than the PD − SH subgroup (76 ± 2 vs. 58 ± 2 y, P = 0.0002). The PD + SH subgroup had a higher frequency of males (P = 0.01), people of Ashkenazic extraction (P = 0.02), orthostatic hypotension (P = 0.006), orthostatic hypotension beginning before or within 1 y of onset of the movement disorder (P = 0.002), and greater age at onset of the movement disorder (66 ± 4 vs. 54 ± 3 y, P = 0.02), and a greater proportion were treated with fludrocortisone (P = 0.007) or midodrine (P = 0.05). Both subgroups had mild to moderate parkinsonism, as judged by the Unified Parkinson Disease Rating Scale (means, 35 vs. 42 of 176 while not taking levodopa), and the subgroups did not differ in responsiveness to levodopa, urinary symptoms, constipation, altered sweating, depression, dementia, or fatigue.
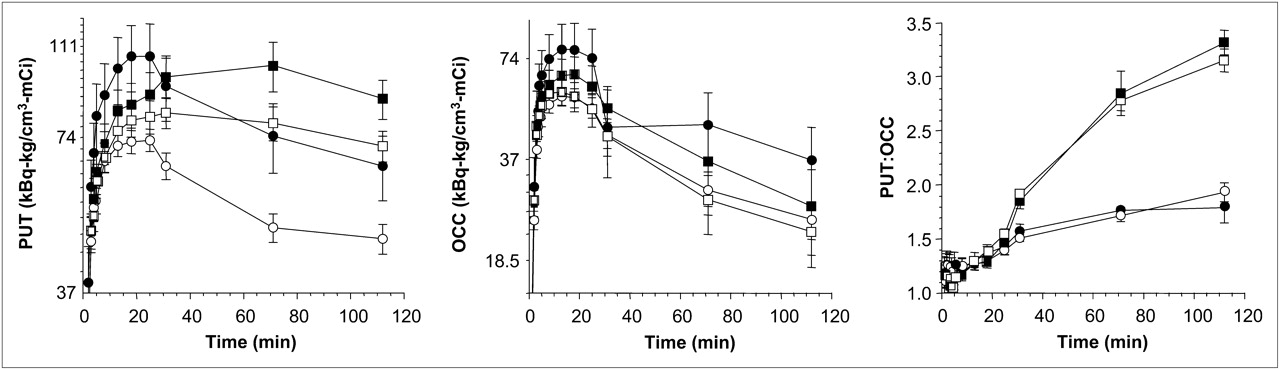
Across all subjects, orthostatic changes in systolic blood pressure correlated negatively with supine systolic blood pressure (r = −0.66, P < 0.0001). Putamen, caudate, and occipital cortex concentrations of 6-18F-fluorodopa–derived radioactivity increased rapidly, with peak concentrations attained about 25 min after cessation of the 3-min infusion (Fig. 1). In the PD and PAF groups, peak radioactivity concentrations correlated positively with supine systolic and mean arterial pressure for the putamen (r = 0.50, P = 0.002), caudate (r = 0.41, P = 0.02), and occipital cortex (r = 0.50, P = 0.003). In the control group, peak radioactivity concentrations were unrelated to supine blood pressure.
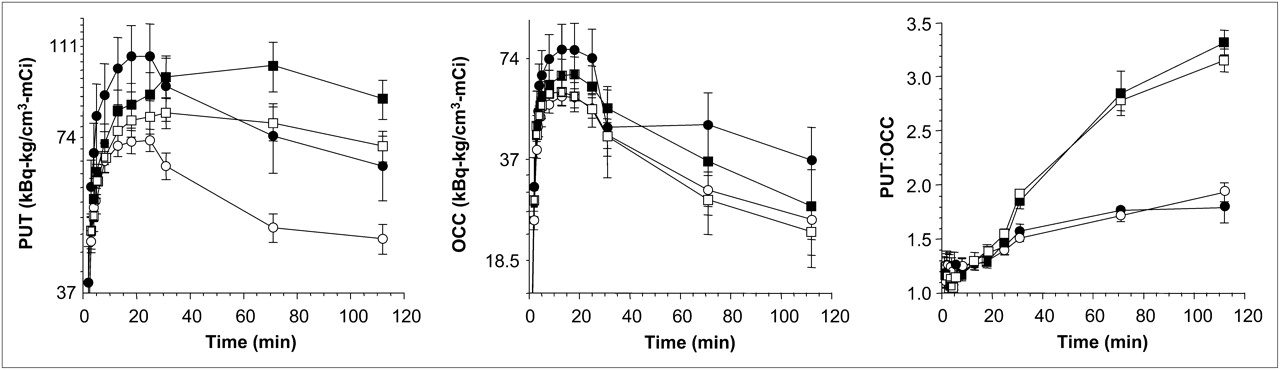
Mean (±SEM) values for tissue concentrations of 6-18F-fluorodopa–derived radioactivity in putamen (PUT) and occipital cortex (OCC) as function of time after initiation of 3-min intravenous infusion of tracer, in patients with PD + SH (•), patients with PD − SH (○), patients with PAF (▪), and control subjects (□). Right panel shows values for putamen-to-occipital cortex ratio.
Peak putamen radioactivity correlated strongly and positively with peak occipital cortex radioactivity (r = 0.88, P < 0.0001). Fractional decreases in occipital cortex radioactivity between the peak and late values were similar in all groups. Putamen-to-occipital cortex ratios of 6-18F-fluorodopa–derived radioactivity rapidly increased with time after tracer administration (Fig. 1).
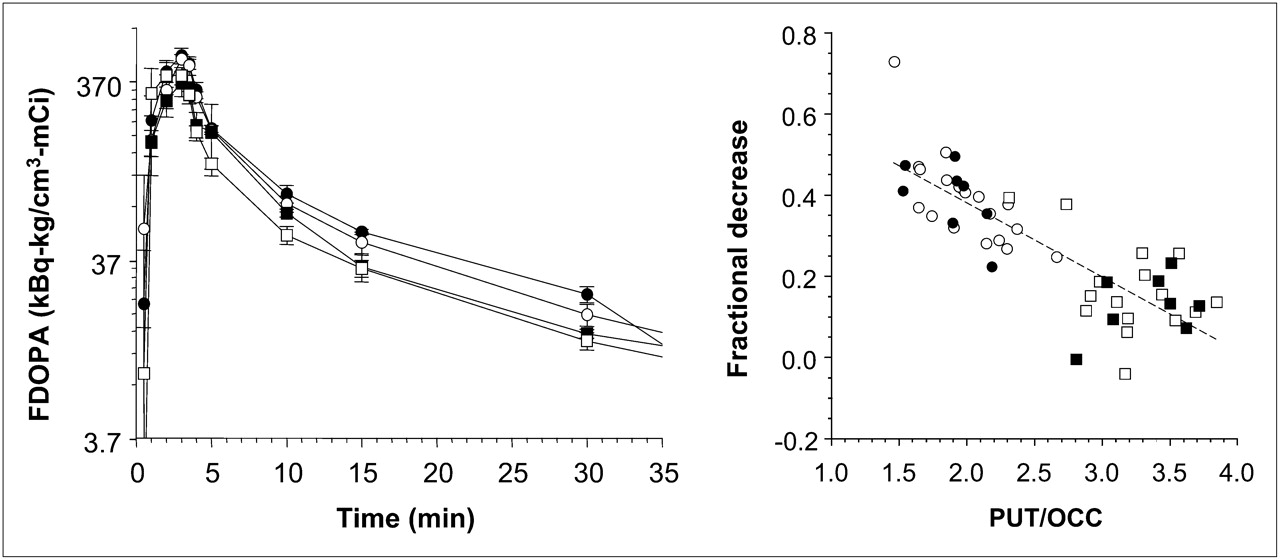
The compared groups did not differ in arterial 6-18F-fluorodopa concentrations, either in terms of mean values at any time point or of integrated arterial 6-18F-fluorodopa concentrations. There were no relationships between peak 6-18F-fluorodopa–derived radioactivity concentrations in the putamen, caudate, or occipital cortex regions and peak arterial 6-18F-fluorodopa concentrations (Fig. 2).

{kind=link}
{kind=link}
Mean (±SEM) values for arterial plasma concentrations of 6-18F-fluorodopa as function of time after initiation of 3-min intravenous infusion of tracer, in patients with PD + SH (•), patients with PD − SH (○), patients with PAF (▪), and control subjects (□). Right panel shows individual values for fractional declines in radioactivity between peak and late values, as a function of putamen-to-occipital cortex ratios.
Among PD patients, individual values for peak putamen concentrations of 6-18F-fluorodopa–derived radioactivity correlated positively with supine systolic pressure (r = 0.55, P = 0.004), and individual values for the ratio of peak occipital cortex 6-18F-fluorodopa–derived radioactivity to peak arterial 6-18F-fluorodopa correlated positively with supine mean arterial pressure (r = 0.76, P = 0.04).
Peak putamen 6-18F-fluorodopa–derived radioactivity was higher in the PD + SH than in the PD − SH subgroup (P = 0.01; Fig. 1). After the peak putamen radioactivity had been attained, the radioactivity decreased more slowly in the PAF and control groups than in either PD subgroup. Between the peak and late (∼112 min) time points, the PD + SH and PD − SH groups had similar fractional declines in 6-18F-fluorodopa–derived radioactivity that were larger than the fractional decreases in the control group (0.40 ± 0.03 and 0.39 ± 0.03 vs. 0.16 ± 0.03, P < 0.0001 each).
At the late time point, the PD − SH subgroup had lower putamen 6-18F-fluorodopa–derived radioactivity than the control group (P = 0.0005), whereas the PD + SH group did not.
Trends in caudate concentrations of 6-18F-fluorodopa–derived radioactivity generally resembled trends in putamen concentrations, but with less statistical significance.
Peak occipital cortex 6-18F-fluorodopa–derived radioactivity was higher in the PD + SH subgroup than in the PD − SH subgroup (P = 0.006) or the control group (P = 0.01). In the PD + SH and PD − SH subgroups, the rate of increase in the putamen-to-occipital cortex ratio was attenuated, and the difference from control increased progressively with time (Fig. 1). At about 112 min after 6-18F-fluorodopa administration, the mean late putamen-to-occipital cortex ratios in the PD + SH and PD − SH subgroups (1.88 ± 0.09 and 1.99 ± 0.07, respectively) were clearly lower than the mean ratio in the normal control group (3.33 ± 0.11, P < 0.0001 each). The PAF group had about the same mean late putamen-to-occipital cortex ratio (3.33 ± 0.11) and fractional decline of radioactivity (0.13 ± 0.03) as did the control group.
Among PD patients and across all subjects, the fractional decline in putamen 6-18F-fluorodopa–derived radioactivity between the peak and late values correlated negatively with the late putamen-to-occipital cortex ratio (r = −0.71, P < 0.0001; r = −0.82, P < 0.0001; Fig. 2).
DISCUSSION
In this study, PD patients who had severe SH (defined by a systolic blood pressure of ≥180 mm Hg) had higher peak striatal concentrations of 6-18F-fluorodopa–derived radioactivity than did PD − SH patients or healthy controls. Across individual PD patients, there were positive correlations of peak putamen, caudate, and occipital cortex 6-18F-fluorodopa–derived radioactivity with supine blood pressure. Increased striatal and occipital cortex radioactivity in the PD + SH subgroup could not be attributed to increased arterial 6-18F-fluorodopa levels, since there were no group differences in mean arterial 6-18F-fluorodopa concentrations. Moreover, individual values for the ratio of peak putamen to peak arterial 6-18F-fluorodopa in PD patients correlated positively with supine blood pressure. These results suggest that elevated striatal radioactivity concentrations in PD + SH resulted from increased entry of 6-18F-fluorodopa into the brain.
Peak concentrations of 6-18F-fluorodopa–derived radioactivity in the occipital cortex, a control region devoid of dopaminergic innervation, closely paralleled those in the putamen. This parallelism explained similarly blunted increases in putamen-to-occipital cortex ratios over time in the PD + SH and PD − SH subgroups despite the subgroup difference in peak putamen radioactivity. It may also explain why studies based on the pharmacokinetics of 6-18F-fluorodopa–derived radioactivity measured simultaneously in striatal and control compartments have consistently reported a decreased mean rate constant for striatal uptake of 6-18F-fluorodopa–derived radioactivity in PD.
The findings in the PAF group support these interpretations. PAF is a rare Lewy body disease in which neurogenic orthostatic hypotension and SH occur together, as in PD + SH, but without parkinsonism. As in the PD + SH subgroup, across individual PAF patients peak putamen radioactivity correlated positively with supine systolic pressure, even though the PAF patients had normal putamen-to-occipital cortex ratios of 6-18F-fluorodopa–derived radioactivity.
Although commonly used control areas such as the occipital cortex and cerebellum possess scant dopaminergic innervation, they do possess some noradrenergic innervation. Moreover, cerebellar norepinephrine concentrations are decreased in PD (8). 6-18F-fluorodopa taken up in the occipital cortex is stored as unmetabolized tracer and as 6-18F-fluorodopamine (9). If 6-18F-fluorodopa–derived radioactivity were stored both in striatal dopaminergic terminals and in the control tissue, then the extent of striatal dopaminergic denervation could be underestimated.
The present results indicate a contribution of hypertension to peak 6-18F-fluorodopa–derived radioactivity in PD. The association of elevated initial striatal radioactivity with SH in PD may help explain why, considered as a single group, patients with PD do not have subnormal peak or late striatal concentrations of 6-18F-fluorodopa–derived radioactivity. The PD − SH subgroup did have low late striatal concentrations of 6-18F-fluorodopa–derived radioactivity; however, even the PD − SH subgroup did not have lower peak striatal 6-18F-fluorodopa–derived radioactivity than did the control group.
Quantifying retention of 6-18F-fluorodopa–derived radioactivity may provide an alternative, relatively simple, valid means for quantifying striatal dopaminergic deficiency. Although the PD + SH and PD − SH subgroups differed in peak striatal levels of 6-18F-fluorodopa–derived radioactivity, the 2 subgroups had proportionately similar, abnormal, rapid declines in radioactivity after the peaks. Fractional decreases in 6-18F-fluorodopa–derived radioactivity between the peak (at ∼25 min) and late (∼112 min) scans were augmented in PD, independent of SH. Calculation of fractional loss of 6-18F-fluorodopa–derived radioactivity therefore may identify loss of striatal dopaminergic terminals in PD, without adjusting for SH or for 6-18F-fluorodopa–derived radioactivity in a control region.
Ordinarily, cerebrovascular autoregulation limits the effects of alterations in blood pressure on cerebral blood flow; however, in humans, autoregulation is no longer operative above a systolic pressure of about 170 mm Hg (10). In our study, SH above the autoregulatory range could explain increased blood flow and thereby increased 6-18F-fluorodopa delivery to both the striatum and control regions. The role of sympathetic innervation in regulation of cerebral blood flow remains controversial (11–13), and the literature about autoregulatory capacity in autonomic failure is inconsistent (14–18). Because PD with neurogenic hypotension and PAF are associated with evidence of generalized noradrenergic denervation (19), we speculate that patients with Lewy body diseases have a decreased ability to limit entry of 6-18F-fluorodopa into the brain at high blood pressures.
CONCLUSION
Peak striatal concentrations of 6-18F-fluorodopa–derived radioactivity depend not only on dopaminergic innervation but also on delivery of the tracer to the brain by cerebral perfusion and passage through the blood–brain barrier. Patients with PD + SH or PAF have higher peak striatal and occipital cortex radioactivity concentrations than can be accounted for by arterial 6-18F-fluorodopa levels. The effects of hypertension on striatal 6-18F-fluorodopa uptake may contribute to failure of peak radioactivity concentrations alone to indicate striatal dopaminergic denervation in PD. Measurement of local fractional loss of 6-18F-fluorodopa–derived radioactivity can identify striatal dopaminergic deficiency, without use of a particular pharmacokinetic model or adjustment for radioactivity in a control region.
Acknowledgments
We thank Drs. Basil Eldadah, Richard Imrich, and Yehonatan Sharabi; Sandra Pechnik; Tereza Jenkins; and the NIH PET Department. The research described in this report was supported by the intramural research program of the National Institute of Neurological Disorders and Stroke, National Institutes of Health. There are no potential financial conflicts of interest to disclose.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- Received for publication February 3, 2009.
- Accepted for publication May 19, 2009.