

Abstract
Early discrimination between benign and malignant pleural diseases is vital for the treatment and prognosis of a patient. Imaging is traditionally performed with CT or MRI, with an accuracy of 50%–75%. PET has proven to be superior as a diagnostic tool in several malignancies. In this prospective study, PET results in patients with pleural abnormalities on CT were compared with histologic results. Methods: Eligible patients had pleural thickening on CT and were medically fit for surgical diagnostic procedures. All patients underwent PET. Qualitative assessment led to a PET score of 1 (definitely normal), 2 (probably normal), 3 (probably abnormal), or 4 (definitely abnormal). PET scores of 1 or 2 indicated a negative PET finding, whereas PET scores of 3 or 4 indicated a positive PET finding. Pathologic verification techniques included thoracocentesis, thoracoscopy, or open pleural biopsy at thoracotomy. Results: Thirty-two patients were enrolled, 19 with malignant and 13 with benign pleural disease. PET was true positive in 18 and true negative in 12 patients, with an accuracy and negative predictive value of 94% and 92%, respectively. PET was false negative in a patient with a slowly growing malignant solitary fibrous tumor and false positive in a patient with infectious pleuritis. Median standardized uptake values calculated for 7 patients with malignant and benign pleural diseases were 6.28 and 1.69, respectively. Patients with a PET score of 1 or 2 survived significantly longer than patients with a PET score of 3 or 4. Conclusion: Qualitative assessment of pleural thickening with PET accurately discriminates between malignant and benign pleural thickening, with a high accuracy and negative predictive value.
- PET
- 18F-FDG
- pleural diseases
- mesothelioma
Determining the etiology of pleural thickening remains a challenging clinical problem. Early discrimination between benign and malignant pleural diseases is vital for treatment and prognosis. In particular, malignant pleural mesothelioma (MPM) has to be distinguished from other causes of pleural thickening. MPM has an unfavorable median survival of 4–12 mo, because of a usually long interval between presentation and diagnosis and the local aggressiveness of the tumor (1). However, a few selected patients may benefit from chemotherapy or trimodality treatment (2).
Traditionally, pleural diseases can be imaged by chest radiography, CT, and MRI. CT is more accurate than chest radiography (3) and has been used for the assessment of MPM for more than 15 y. In several studies, CT and MRI performed equally well in the staging of MPM, with an overall staging accuracy of 50%–75% (3–5).
Whole-body PET with 18F-FDG is a noninvasive metabolic imaging technique and an accurate diagnostic and staging tool for several types of malignant disease (6). In particular, PET has proven accuracy in the diagnosis of solitary pulmonary nodules and the preoperative staging of non–small cell lung cancer (7,8). A few reports are available on PET in the evaluation of malignant pleural diseases (9–13). These reports show an overall accuracy of 88%–92% for PET. Only 2 limited studies could be found that evaluated PET in the differential diagnosis of pleural diseases (9,14). Therefore, we prospectively evaluated the feasibility of PET in the diagnosis of pleural thickening on CT, with pathologic results as the gold standard.
MATERIALS AND METHODS
Patients
Consecutive patients who had pleural abnormalities and presented at the pulmonary outpatient department of the Groningen University Hospital were evaluated by history, physical examination, complete blood cell count, renal and liver function tests, chest radiography, chest CT, and bronchoscopy. Eligibility criteria for this study were pleural thickening on chest CT, medical fitness for surgical diagnostic procedures (thoracoscopy, open pleural biopsy, thoracotomy), and an age of at least 18 y. Patients were excluded if they had hyperglycemia (serum glucose > 10 mmol/L) (15).
Thirty-two patients were included. All patients gave informed consent before enrollment. The study was approved by the Medical Ethics Committee of the Groningen University Hospital.
PET
Patients had to fast for 6 h before PET scanning, but they were allowed to drink water and take their usual medications. 18F-FDG was synthesized according to the method of Hamacher et al. by an automated computer-controlled synthesis module (16,17). Whole-body PET was performed 90 min after intravenous injection of 400–600 MBq of 18F-FDG, with either an ECAT 951/31 or an ECAT HR+ camera (Siemens/CTI). Fields of view were 10.8 and 15.0 cm, respectively, with respective resolutions of 6 and 5 mm in full width at half maximum. Attenuation correction of the 18F-FDG activity was obtained by transmission scanning with a 68Ge/68Ga source, to enable calculation of a standardized uptake value (SUV) for semiquantitative measurement of the 18F-FDG activity. PET images were reconstructed into coronal, sagittal, and transverse sections and a rotating projection. 18F-FDG uptake was qualitatively assessed by 2 experienced physicians unaware of clinical data. A hot spot was defined as focally increased 18F-FDG uptake in comparison with the background and not related to physiologic processes. The PET hot spots were assigned a PET score indicating the hot-spot intensity per patient: 1 (definitely normal), 2 (probably normal), 3 (probably abnormal), or 4 (definitely abnormal). PET findings were considered negative if the PET score was 1 or 2 and positive if the score was 3 or 4.
SUV was calculated in the transaxial plane in which the hot spot had the highest activity. To minimize variability in SUV due to body composition, SUV was calculated using the lean body mass (18). Regions of interest for SUV measurement were drawn using the isocontour tool adjusted to 70% of the peak counts of the hot spot. Because of time constraints, only 11 of the 32 patients underwent transmission scanning. In 4 of those 11 patients, no PET hot spot was detected. ECAT/CAPP software (Siemens/CTI) was used for analysis.
Pathologic Examination
The study was performed on an intention-to-diagnose basis; that is, all necessary procedures for a pathologic diagnosis were performed, and patients with benign pleural diseases were followed up for at least 1 y. Diagnostic procedures for pathologic verification included thoracocentesis for cytologic and chemical analysis of pleural effusion, thoracoscopy, or open pleural biopsy at thoracotomy. No treatment was started until all pathologic examinations had been finished. Depending on the diagnosis and the diagnostic procedure, pathologic examination methods consisted of cytology, histology, and immunohistochemistry.
Statistical Analysis
Statistical analysis was performed with SPSS 10 software (SPSS Inc.). Continuous variables are reported as medians and ranges. Operating characteristics are reported with a 95% confidence interval. Differences in SUV were calculated with the Mann–Whitney U test. Survival was measured in months after the day of the admission related to the pleural abnormalities. Survival was analyzed with the Kaplan–Meier method and the log-rank test. Reported P values are 2 sided, and P < 0.05 was considered to indicate significance.
RESULTS
Patients
Thirty-two patients were enrolled from January 1996 to September 2001 (Table 1). Malignant pleural disease was diagnosed in 19 patients, and benign pleural disease in 13 patients.
Characteristics of the 32 Consecutive Patients with Pleural Thickening on CT
A pathologic diagnosis was obtained in 27 patients, by either thoracocentesis (n = 3), thoracoscopy (n = 6), closed pleural biopsy (n = 7), or open pleural biopsy at thoracotomy (n = 11). A pathologic diagnosis was not obtained in 5 patients (1 patient with suspected MPM and 4 with benign diseases). The patient with suspected MPM died 11 mo after his first presentation, because of progressive disease. The diagnoses in the 4 patients with benign diseases were infectious pleuritis (1 patient, with positive cultures), asbestosis (1 patient, with typical radiologic abnormalities), and pleural fibrosis of unknown origin (2 patients). During a minimum follow-up of 22 mo, their pleural abnormalities remained stable.
PET
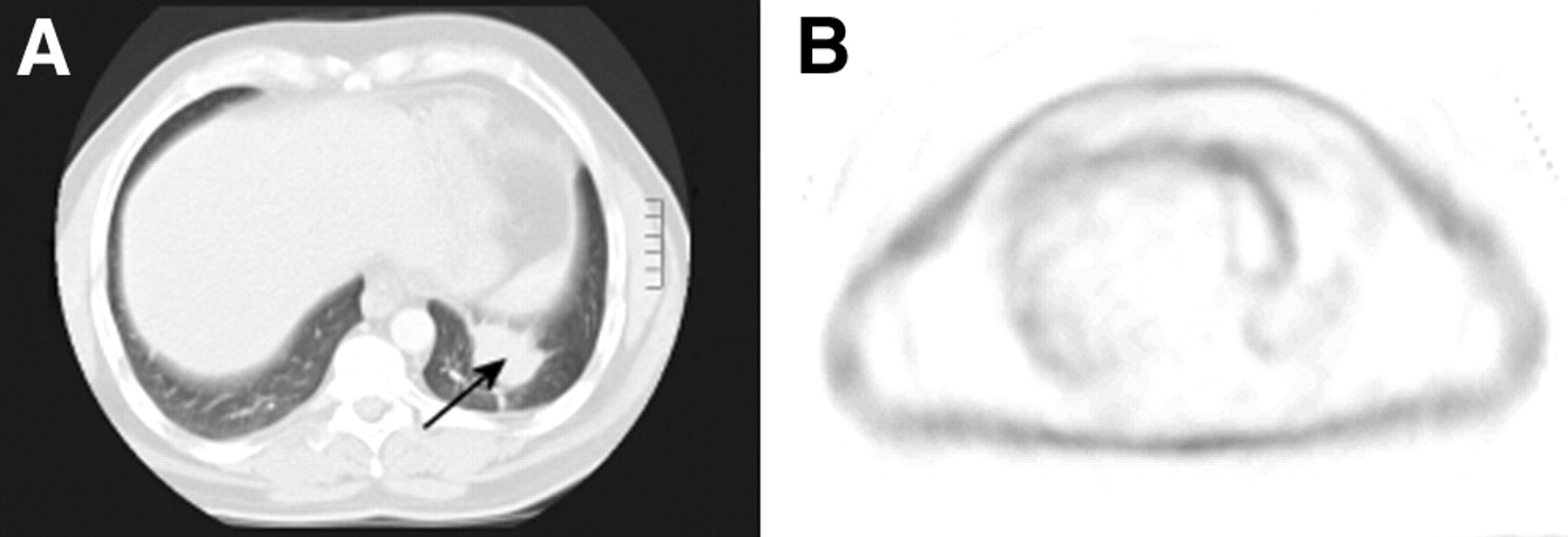
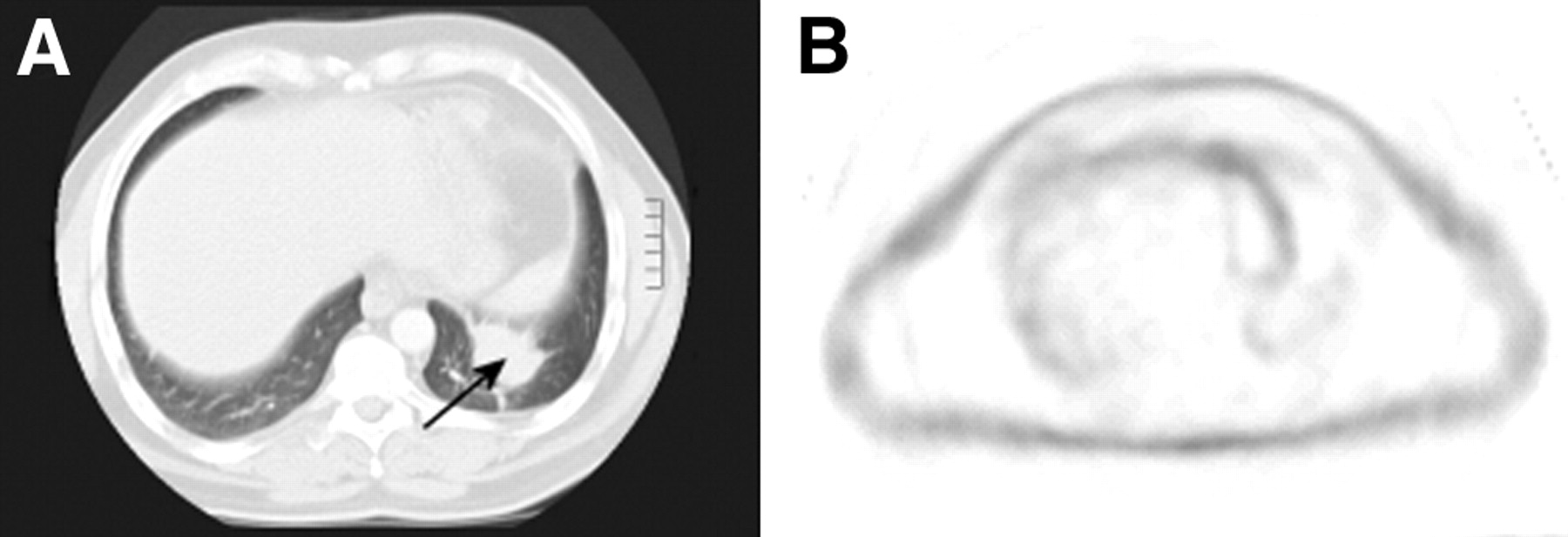
Typical CT and PET images of a patient with MPM and a patient with pleural fibrosis are shown in Figures 1 and 2, respectively. PET results were positive in 19 patients (9 patients with a PET score of 3 and 10 patients with a score of 4) and negative in 13 patients (7 patients with a PET score of 1 and 6 patients with a score of 2). Qualitative assessment of PET resulted in a high sensitivity, specificity, accuracy, positive predictive value, and negative predictive value (Table 2.) PET correctly identified 18 of the 19 patients with malignant pleural disease and 12 of the 13 patients with benign disease. PET was false negative in a patient with a slowly growing malignant solitary fibrous tumor and false positive in a patient with infectious pleuritis. Unfortunately, no SUVs could be calculated for the patients with the false-negative and false-positive PET results.
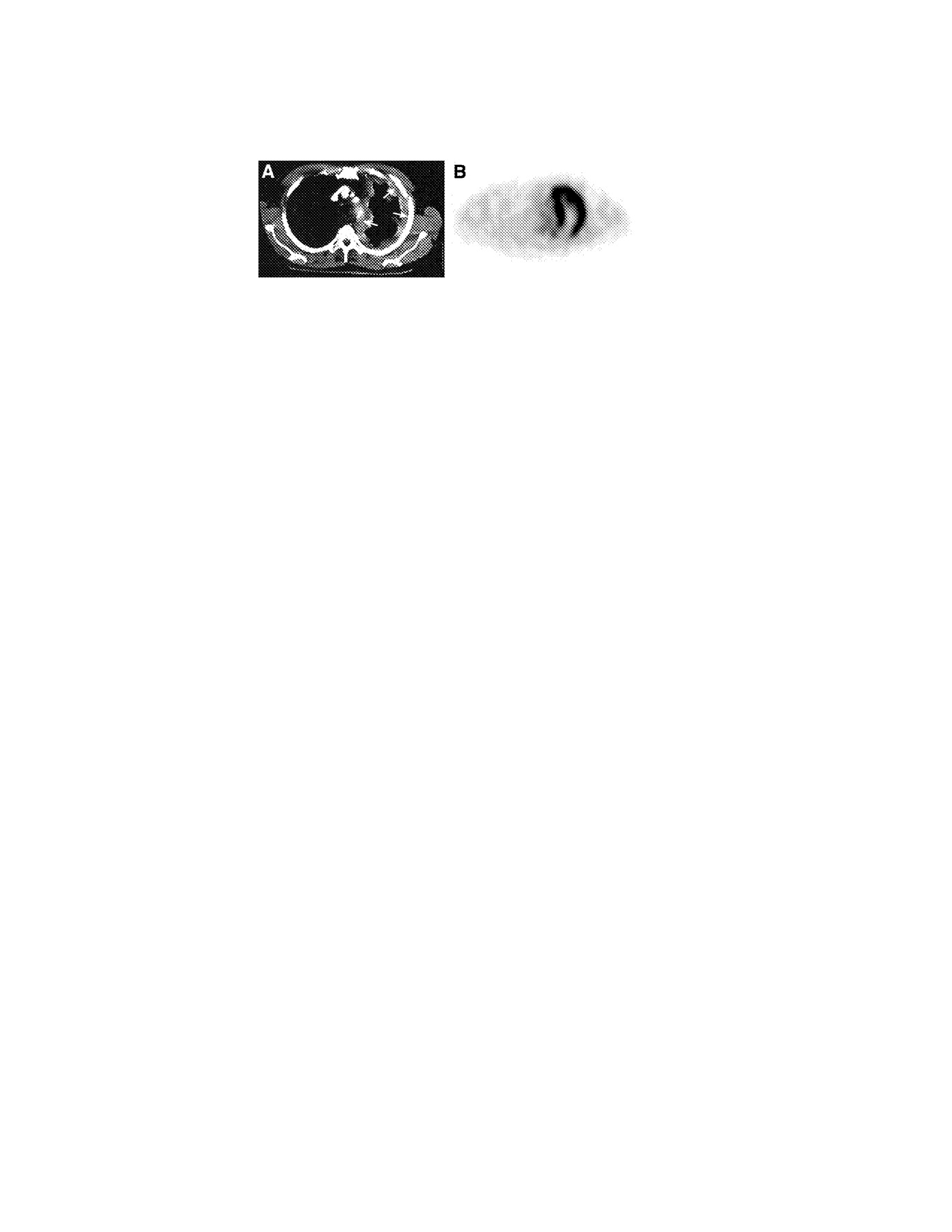
Images of a patient with MPM. (A) CT shows a thickened parietal and mediastinal pleura on the left side (arrows). (B) The corresponding PET image shows 18F-FDG uptake in the ventral parietal and mediastinal pleura, without apparent involvement of mediastinal lymph nodes.
{kind=link}
{kind=link}
Images of a patient with pleural fibrosis. (A) CT shows an abnormality of the left diaphragmatic pleura (arrow). (B) The corresponding PET image shows no hot spot in that region.
Operating Characteristics of PET with Qualitative Assessment of Pleural Thickening on CT
SUV could be calculated in 7 patients, 2 with a PET score of 1 or 2 (both patients had reactive pleuritis) and 5 with a PET score of 3 or 4 (3 patients with MPM, 1 with large cell carcinoma, and 1 with chest wall sarcoma). Patients with a PET score of 1 or 2 had a median SUV of 1.69 (range, 1.37–2.01), whereas patients with a PET score of 3 or 4 had a median SUV of 6.28 (range, 2.46–6.94) (P = 0.053).
Survival
Patients with a PET score of 1 or 2 (group A) had significantly better survival than patients with a PET score of 3 or 4 (group B) (P = 0.0005). One-year survival was 100% in group A and 42% in group B, whereas both 2- and 3-y survivals were 100% in group A and 18% in group B. At the September 2003 analysis, 14 of the 19 patients with malignant pleural disease had died, with a median survival of 9 mo (range, 1–22 mo). Five patients were still alive with a median follow-up of 36 mo (range, 13–46 mo). The diagnoses in these patients were adenocarcinoma of the lung with pleural metastasis, slowly growing malignant solitary fibrous pleural tumor, sarcoma of the chest wall (2 patients), and undifferentiated pleural tumor of unknown origin.
Of the 13 patients with benign pleural disease, 1 had died because of sepsis from diabetic ulceration of his right foot (survival, 4.5 mo). Twelve patients with benign pleural disease were still alive at a median follow-up of 37 mo (range, 16–59 mo), with no signs or symptoms of malignancy.
DISCUSSION
Differentiating MPM and pleural metastases of extrapulmonary malignancies from benign pleural thickening is difficult. Therefore, we examined the feasibility of 18F-FDG PET for evaluation of pleural thickening. We found PET to have a high sensitivity and specificity in the diagnosis of pleural thickening. The high sensitivity is in line with studies examining the diagnostic value of PET in pleural thickening (9,10,12,14). These studies together included 65 patients with malignant pleural disease, mostly MPM. Bénard et al. showed that PET was sensitive for identifying MPM and for determining the extent of disease (10). A disadvantage of their study was that almost all (86%) patients had malignant pleural disease and only 4 (14%) had benign disease, making a comparison of PET in malignant and benign pleural diseases inappropriate. The operating characteristics of PET in the present study (Table 2) are higher, with overall smaller 95% confidence intervals because of a more equal distribution of malignant (59%) and benign (41%) diseases.
The clinically most important result of our study is the 92% negative predictive value of PET. This value implies that patients with pleural thickening and negative PET findings (PET score of 1 or 2) may be followed up using only CT instead of pathologic diagnostic procedures. A positive PET finding (PET score of 3 or 4) should always lead to a procedure for tissue verification.
Two important studies have been performed for the staging of MPM by PET. Flores et al. examined 60 MPM patients before surgical intervention (13). Although this study did not indicate whether PET could differentiate between benign and malignant pleural disease, PET was able to identify or exclude distant metastases (thus precluding surgery for MPM in those patients). All patients in this study showed 18F-FDG uptake by the MPM, with a mean SUV of about 7.0, which is comparable with the median SUV for malignant pleural disease in the present study. Unfortunately, PET was not reliable for staging local tumor growth and mediastinal lymph node metastases (13). Schneider at al. performed a study on 18 patients with MPM (11). They reported that PET failed to image chest wall involvement by MPM, but mediastinal lymph nodes were reliably staged.
A limitation of our study was the relatively small number of patients included, which may hamper straightforward extrapolation of the conclusions to the general MPM population. Furthermore, the number of calculated SUVs was limited. Although SUVs may improve specificity and negative predictive value, there is still no general agreement whether visual assessment of PET is inferior to SUV. In the present study, the PET score was closely associated with SUV, and we demonstrated a clear difference in survival between patients with a high PET score and patients with a low PET score. The SUV threshold of between 2.0 and 2.5 that we found for malignant pleural disease is in line with the SUV threshold of 2.0 described by Bénard et al. (10) However, the role of SUV in the differentiation of malignant and benign disease is still undetermined.
The false-negative PET result in our study was due to a slowly growing malignant solitary fibrous tumor. Three patients with false-negative PET findings in previous studies had epithelioid-type MPM (10,12). Two of these patients had an SUV < 2.0, indicating low tumor metabolism. Epithelioid-type MPM is a slowly growing subtype with a low mitosis rate and a better overall survival than other subtypes of MPM (19,20). In the patient with a false-positive PET result, infectious pleuritis was diagnosed. In previous studies, the same diagnosis was made in 3 patients with false-positive PET findings (9,10). Infectious diseases are known causes of PET positivity in the absence of malignancy (6), again emphasizing the need for pathologic verification of positive PET results.
CONCLUSION
PET provides useful information for the assessment of pleural thickening observed on CT. Qualitative assessment with PET discriminates between malignant and benign pleural thickening with a high accuracy and a high negative predictive value. A significant survival difference was shown between patients with high 18F-FDG uptake and patients with low 18F-FDG uptake. We recommend PET assessment of pleural thickening seen on CT, with pathologic verification of positive PET results.
Acknowledgments
The authors thank Jan Pruim, MD, PhD (nuclear medicine physician, Groningen University Hospital), for serving as an independent observer in the assessment of PET scans.
Footnotes
Received Oct. 29, 2003; revision accepted Jan. 14, 2004.
For correspondence or reprints contact: Henk Kramer, MD, Department of Pulmonary Diseases, Groningen University Hospital, P.O. Box 30 001, 9700 RB Groningen, The Netherlands.
E-mail: h.kramer{at}int.azg.nl