

Abstract
The object of this study was to develop a new technique for the quantitative measurement of lymphatic function. The rate of clearance of radiolabeled protein from a subcutaneous depot is supplemented by measurement of the appearance of the protein in venous blood. This initial study was performed on normal arms, with a view to subsequent clinical application such as in the investigation of women with breast cancer–related lymphedema (BCRL). Methods: Fourteen healthy volunteers (12 women, 2 men) and 8 women awaiting surgery for breast cancer were recruited for the study. Each received subcutaneous depot injection of protein solution in the second dorsal web space of each hand, labeled with 111In on one side and with 99mTc on the other side. Human serum albumin (HSA) was the protein used in the first 8 subjects and human polyclonal immunoglobulin G (HIgG) was used thereafter. The activity at each depot was measured at regular intervals using a collimated sodium iodide scintillation detector, and the activity in venous blood sampled from both arms was measured in an automatic sample counter. Results: 99mTc-HSA cleared from the depot consistently faster than 111In-HSA (P = 0.001). The proportions of radionuclide remaining bound to protein in venous blood were higher for 99mTc than for 111In. HIgG displayed improved labeling stability for both nuclides, reflected in equal rates of clearance. Blood activity rose steadily after an early latent phase and for HIgG correlated strongly with the rate of clearance from the depot (P < 0.001). Marked variation between individuals was observed. Conclusion: A dual-isotope technique relies on identical behavior of the 2 radiopharmaceuticals used. This study shows that this is the case with respect to HIgG but not HSA. 99mTc-HSA cleared faster than 111In-HSA and yet displayed better in vivo labeling stability. We conclude that 111In dissociates from HSA in the depot but then becomes locally bound. Using HIgG, a close correlation was observed between the rates of clearance from the depot and the appearance in venous blood. This finding suggests that HIgG would be a suitable marker for subsequent dual-isotope studies on women with BCRL.
- lymphatic function
- lymphedema
- depot clearance
Investigation of lymphatic edema requires a reliable method for assessing lymph flow. This is particularly true in the case of breast cancer–related lymphedema (BCRL), in which evidence increasingly suggests that factors in addition to interruption of lymphatic drainage at the axilla contribute to the development of arm swelling (1). The current mainstay of clinical investigation is lymphoscintigraphy, which provides structural and functional data on the region of the injection depot (uptake into initial lymphatics), along the extremity (transit in large collectors), and over regional lymph nodes (storage) (2). Information can be derived from scintigraphy, which may assist in semiquantification of lymphatic flow but is unable to give an absolute measure of the flow rate. The arrival time at regional lymph nodes after depot injection is a measure of velocity (3) but, because the flow rate is also a function of the cross-sectional area and it is known that lymphatic vessels dilate after proximal obstruction, a reduced velocity may still be associated with a normal or even increased rate of flow. Storage activity in regional lymph nodes has been shown to be a useful diagnostic tool in cases of unexplained edema (4) and has been reported to be the most sensitive marker of lymphatic failure in BCRL (5–7). In a large study conducted by Goltner et al. (8), 100% of patients with arm swelling showed reduced storage activity in the ipsilateral axilla compared with that in the contralateral axilla at 2 y after surgery. However, patients in the study had between 5 and 35 axillary lymph nodes removed during surgery and had subsequent irradiation of the area, such that no meaningful comparison could be made (reduced storage was also found in 90% of postoperative patients with no arm swelling).
After subcutaneous injection, tracer clears from the depot site in an exponential fashion (9,10). Many studies have found measurement of residual depot activity to be of little use in investigation of lymphedema (5,7,8,11) but have often been based on simply measuring depot activity at the time of injection and at a single point thereafter. Because clearance within the first hour has been shown to be variable (12,13) and to be affected by local conditions (14), with edema presumably altering the volume of distribution and initial access to the lymphatic system, it is necessary to take repeated measurements to identify when exponential clearance commences. By then plotting results on a logarithmic scale, it is possible to calculate the removal rate constant k (in % . min−1). The ultimate disposal of lymphatic fluid is into the great veins of the neck, so the appearance of tracer in venous blood should correlate with the exit of lymph from the arm. Therefore, the appearance in the blood of substances carried initially by lymphatics should provide a guide to the function of the lymphatic system; yet, there is a surprising lack of information on this in the literature.
A suitable radiopharmaceutical for lymphatic flow studies should demonstrate stable radionuclide labeling and gain rapid access to the lymphatic vessels after tissue injection but not to blood vessels (11). Most colloid agents used have optimal median particle sizes in the 40- to 50-nm range (15). Because they are particulate with variable particle size and unpredictable access to the lymphatics, colloids are intuitively at a disadvantage compared with a soluble macromolecule. Moreover, because of the retention in nodes and rapid clearance from blood, colloids cannot be used to obtain data on tracer recovery rates in peripheral blood.
This study was designed to assess the possibility of supplementing depot clearance data with the appearance rates of tracer in venous blood using a soluble macromolecule. With a view to applying this technique to the study of patients with BCRL, this method overcomes the problems associated with the above techniques of arrival time at and storage within regional lymph nodes, when the nodes themselves cannot provide a comparable measure. To obtain venous appearance data for both arms, 2 different radionuclides and dual-isotope techniques were used to study healthy volunteers, with the aim of finding a valid dual-isotope technique that could be applied subsequently to simultaneous measurements in both arms of women with BCRL for research and, ultimately, for clinical applications.
MATERIALS AND METHODS
Fourteen healthy volunteers (12 women, 2 men; age, 20–52 y) were recruited for the initial pilot study. They all gave written informed consent. Subsequently, 8 women (age, 39–75 y) with a new diagnosis of breast cancer and with no clinical evidence of axillary lymph node involvement were investigated preoperatively. The Local Research Ethics Committee approved this project. In the first 8 studies, 99mTc-labeled human serum albumin (HSA) was injected subcutaneously through a 25-gauge needle in the second dorsal web space of one hand and 111In-labeled HSA was injected in the other hand, each in a volume of 0.2 mL. Thereafter, HSA was replaced by human polyclonal immunoglobulin G (HIgG) with the same differential radionuclide labels.
Depot Clearance
The clearance rate from the site of depot injection was measured with a collimated sodium iodide scintillation detector. Pulse height analysis was used with separate windows set for simultaneous detection of 99mTc and 111In. Data were collected immediately after injection and then at frequent intervals for a total of 3 h through a multichannel analyzer interface card and stored to a computer disk for subsequent retrieval and analysis. A standardized exercise protocol (30 fist clenchings) was performed between each set of readings to stimulate lymphatic flow. Measurements were taken from each hand alternately, with subjects grasping a fixed handle to ensure consistent positioning. A long source-to-detector distance of 20 cm was used to minimize the effect of subject movement and repositioning errors. Residual activity was calculated as the percentage of the initial counting rate after injection following dead-time and physical decay correction. The results were plotted as the natural logarithm of this percentage against time. Regression analysis of this plot (by the method of least squares) enabled determination of the removal rate constant k (in % . min−1).
Venous Sampling
In the first 3 subjects, a 20-gauge venous cannula was sited in the medial cubital vein at the antecubital fossa of one arm. In subsequent studies, cannulas were sited in similar positions bilaterally. Venous samples were taken 15 min after depot injection and at frequent intervals up to 3 h. A known volume of whole blood was pipetted into counting tubes and hemolyzed with saponin. All samples were counted in an automatic γ-counter (LKB-Wallac 1282 CompuGamma; Wallac, Turku, Finland) programmed to measure 99mTc and 111In simultaneously. The counting windows were chosen to limit cross talk. Counts were corrected for dead time, instrument background, cross talk between the counting windows, and physical decay of the radionuclides. The counter had been calibrated previously so that counts could be related to absolute activity in the samples. Counts were converted into activity and expressed as a percentage of administered activity per liter of blood. To correct for blood volume differences between individuals, the value for venous activity in the contralateral venous sample taken at 3 h was multiplied by blood volume to give a figure for the total percentage of injected activity present in the blood. Blood volume was predicted from measurements of height, weight, and age in accordance with guidelines of the International Council for Standardization in Hematology. In selected samples, the proportion of protein-bound tracer was determined by a modification of the protein-bound iodine test (17). A total of 1.5 mL 5% trichloroacetic acid was added to 1-mL aliquots of plasma. The tubes were mixed and then centrifuged at 1,000g for 5 min. After decanting the supernatant, the pellet was washed with 2.5 mL 5% trichloroacetic acid and dissolved in 2.5 mL 2N sodium hydroxide. Radioactivities in the supernatant fractions and washings and in the final pellet were measured in the automatic γ-counter, and the percentage activity in the pellet was calculated.
Preparation of Radiopharmaceuticals
99mTc-HSA was prepared by the electrolytic method (18). 99mTc-HIgG was prepared by addition of sodium 99mTc-pertechnetate (∼300 MBq in 4 mL saline, eluted <2 h earlier from a generator eluted within the previous 24 h [Nycomed-Amersham, Little Chalfont, Bucks, U.K.]) to a kit containing 2-iminothiolane-derivatized HIgG (Technescan HIgG; Mallinckrodt, Inc. BV, Petten, The Netherlands). Total activity was measured in an ionization chamber and the product was diluted to 10 MBq/mL with 0.1 mol/L sodium bicarbonate containing 5 mg/mL HIgG (Sandoglobulin; Novartis Pharmaceuticals U.K., Frimley, Surrey, U.K.). HSA and HIgG were derivatized with diethylenetriaminepentaacetic acid and cyclic anhydride and labeled with 111In as described by Hnatowich et al. (19). Labeling efficiencies were determined by instant thin-layer chromatography. The syringe containing the radioisotope was assayed in a CRC15R ionization chamber (Capintec, Inc., Ramsey, NJ), and the time was noted. After the procedure, the residue in the syringe was also assayed, and the net decay-corrected administered activity was calculated. A correction factor of 0.8 was applied when measuring 111In in a plastic syringe. The nominal injected activity was 2 MBq 99mTc and 1 MBq 111In.
Statistics and Analysis
Statistical analysis comparing mean values was performed using the paired Student t test to give a 2-tailed probability value, P. Regression analysis, using the method of least squares, provided a Pearson correlation coefficient, r.
RESULTS
Labeling efficiency (mean ± SD; n = 5) was 97.3% ± 0.6% for 99mTc-HSA and 95.2% ± 3.3% for 111In-HSA at the time of dispensing. The corresponding values for 99mTc-HIgG and 111In-HIgG were 97.1% ± 1.3% and 97.4% ± 0.1%, respectively (n = 3).
Depot Clearance
HSA.
Eight subjects received bilateral depot injections of HSA. In the first subject, problems with venous sampling necessitated the intermittent use of a tourniquet on one arm. Because clearance of 99mTc-HSA from this arm was irregular and reduced compared with that of the other side, the results from this arm were not used for further analysis. A tourniquet was not used in any subsequent studies. In all 7 subjects analyzed, clearance of 99mTc-HSA was faster than that of 111In-HSA. The activity remaining at the depot at 3 h after injection was 58.1% ± 6.4% for 99mTc-HSA and 74.5% ± 8.4% for 111In-HSA (P = 0.008). The rate constant of removal, k, was consistently higher for 99mTc-HSA (0.31% . min−1 ± 0.05% . min−1) than for 111In-HSA (0.17% . min−1 ± 0.06% . min−1) (P = 0.001). Pooling the data gave k values of 0.32% . min−1 for 99mTc-HSA and 0.16% . min−1 for 111In-HSA (Fig. 1A). As well as differences in the behavior of the radionuclides, a marked variation was also found between individuals. Values for k ranged from 0.25% . min−1 to 0.39% . min−1 for 99mTc-HSA and from 0.09% . min−1 to 0.23% . min−1 for 111In-HSA. The age of the subject had no influence on this variation.
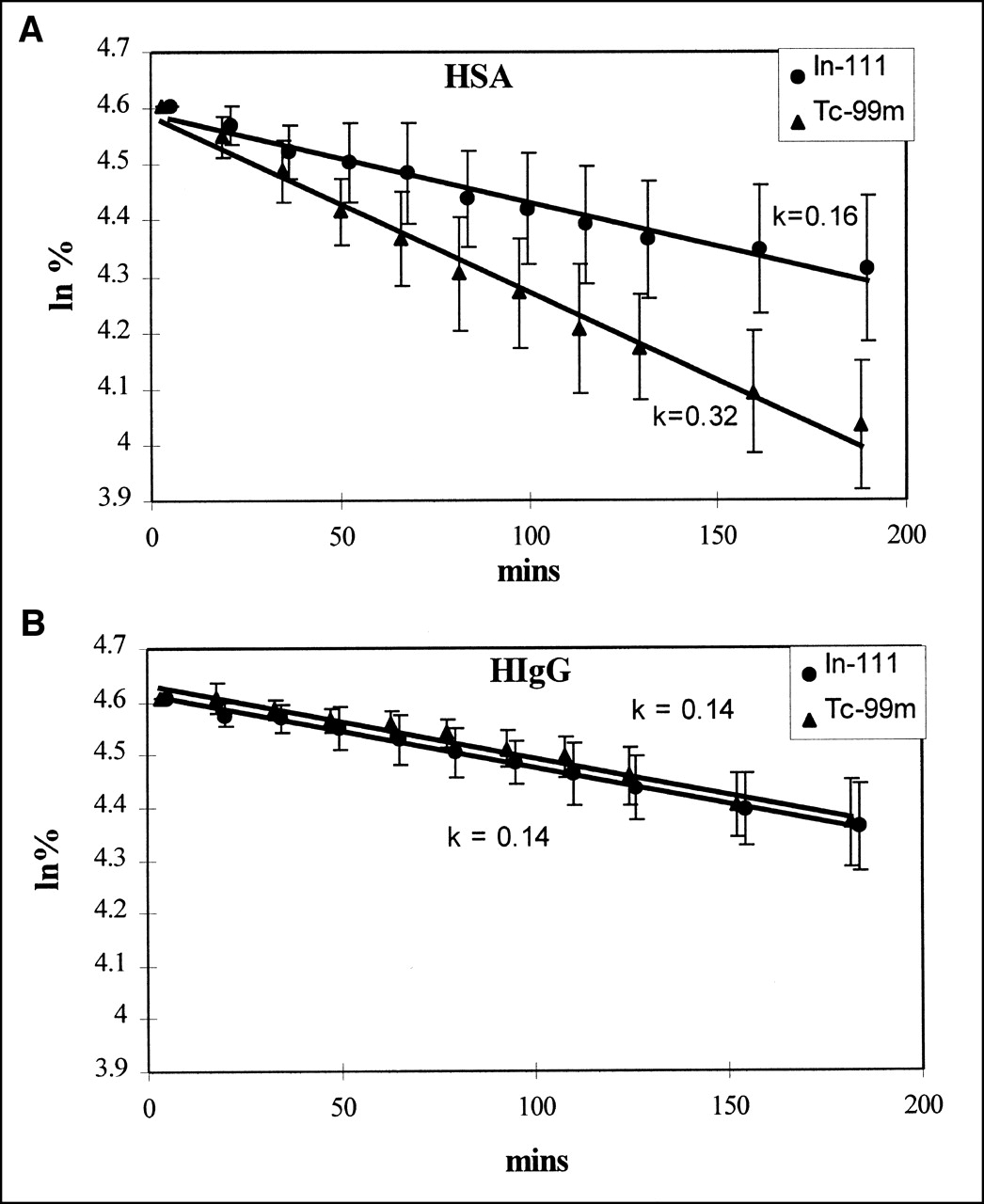
Pooled depot clearance data (plotted as mean natural logarithm [ln] of remaining activity) with trend lines from which rate removal constant k (% . min−1) is calculated for HSA (n = 6) (A) and HIgG (n = 12) (B) with error bars showing 1 SD.
HIgG.
In 1 subject who received HIgG in the pilot study, there was suspicion at the time of depot injection that this had been placed intradermally on one side. Clearance was noted subsequently to be markedly slower from this hand (k = 0.03% . min−1 and k = 0.14% . min−1 from the other hand), with correspondingly reduced blood activity. In another subject, the 99mTc-HIgG labeling was unstable. Although labeling efficiency before injection was confirmed as 97%, there was subsequent rapid dissociation such that the depot cleared very rapidly. In the remaining 4 pilot subjects and 8 preoperative patients, clearance was very similar for both nuclides and consistently slower than had been the case for HSA (99mTc-HIgG, k = 0.14% . min−1 ± 0.05% . min−1; 111In-HIgG, k = 0.14% . min−1 ± 0.04% . min−1). Pooling the data gave k values of 0.14% . min−1 for 99mTc-HIgG and 111In-HIgG (Fig. 1B). Inclusion of the subject with suspected intradermal injection still gave mean k values of 0.14% . min−1 for both radionuclides. Although clearance of both radionuclides was very similar in all subjects other than the 2 cases cited above, marked variation in the clearance rate between individuals again was found (99mTc-HIgG, 0.06% . min−1 to 0.22% . min−1; 111In-HIgG, 0.07% . min−1 to 0.21% . min−1), which did not correlate with age.
Venous Appearance
In the first 3 subjects, venous samples were taken from only one arm so that mixed venous blood activity data (in the contralateral venous sample) were available for only 1 nuclide. Thereafter, bilateral venous samples were taken. After blood volume correction, total activity in venous blood at 3 h as a percentage of injected activity was 11.0% ± 4.4% for 99mTc-HSA and 12.9% ± 4.1% for 111In-HSA (no significant difference). Slightly lower figures were found for 99mTc-HIgG (10.4% ± 3.3%) and 111In-HIgG (9.8% ± 3.6%) (no significant difference). Inclusion of the subject with suspected intradermal injection did not significantly alter the mean values (99mTc-HIgG, 10.6%; 111In-HIgG, 9.7%). Pooled data for mixed venous activity against time for all subjects in whom bilateral samples were taken are shown in Figure 2 for HSA and HIgG. Again, marked variation was seen between individuals (99mTc-HSA, 6.3%–16.5%; 111In-HSA, 6.8%–16.9%; 99mTc-HIgG, 3.1%–14.9%; 111In-HIgG, 3.4%–15%).

Pooled venous activity profiles for HSA (n = 6) (A) and HIgG (n = 12) (B). %/l = percentage of administered activity per liter of blood.
Depot Clearance Versus Appearance in Blood
To assess correlation between the depot clearance and appearance in blood, graphs of k against the total percentage of injected activity in the blood at 3 h were plotted for HSA and HIgG (Figs. 3A–3D). A positive correlation was noted for 99mTc-HSA (r = 0.75, n = 6, P = 0.15) but not for 111In-HSA (r = 0.33, n = 6, P = 0.52). 99mTc-HIgG and 111In-HIgG displayed a significant positive correlation between k and total 3-h venous activity (99mTc-HIgG: r = 0.83, n = 13, P < 0.001; 111In-HIgG: r = 0.92, n = 14, P < 0.001).

{kind=link}
{kind=link}
{kind=link}
Rate removal constant, k (in % . min−1), plotted against total venous activity at 3 h (% injected activity) for HSA (A and B) and HIgG (C and D). • = 111In in healthy volunteers; ○ = 111In in preoperative patients; ▴ = 99mTc in healthy volunteers; ▵ = 99mTc in preoperative patients.
Proportions of Bound Tracer in Venous Samples
In selected subjects, early and late venous samples were tested for the proportion of radionuclide in blood sampled contralateral to the depot that remained bound to protein. Results are shown in Table 1 (in 2 subjects, activity in early venous samples using HIgG were too low for accurate measurement). At early time points a substantial proportion of free radionuclide is in circulation, whereas at late time points most of the circulating radionuclide is bound to protein. However, 111In-HSA and 111In-HIgG are somewhat unstable during the process of separation.
Proportions of Protein-Bound Radionuclide in Venous Blood Samples
DISCUSSION
In this study, depot clearance rates of HSA were consistently different between the 2 arms. This difference was related to the label used, with 99mTc-HSA clearing faster than 111In-HSA. Although the purity of the samples before injection was good (95%–97%), subsequent analysis of activity in venous samples revealed high levels of free label. 99mTc-HSA cleared faster than 111In-HSA and yet a greater proportion remained bound to protein in venous blood. The most likely explanation for this observation is that the in vivo stability of 111In-HSA is lower than that for 99mTc-HSA, but having dissociated from HSA, 111In becomes bound locally at the depot site and is subsequently cleared more slowly. This explanation is supported by the finding of a positive correlation between the depot clearance and appearance in blood for 99mTc-HSA but not for 111In-HSA. The behavior of the 2 radionuclides was virtually identical using HIgG, although the in vivo stability appeared only slightly improved. Clearance curves often diverged in the early period after injection, with the depot activity of 99mTc often exceeding 100% of initial activity, but then came together subsequently. This early behavior of 99mTc-HIgG has been observed previously (11,12) and is thought to be associated with diffusion of free label away from the site of depot injection, in part toward the skin surface such that measured activity is increased. Clearance rates were consistently slower for HIgG than for HSA.
The in vivo instability of 111In-HSA was unexpected. 111In-HSA and 111In-HIgG showed similar stability in vitro in saline and in human serum at 37°C and behaved comparably on challenge with excess free diethylenetriaminepentacetic acid. Both were somewhat unstable in the presence of trichloroacetic acid during the protein-bound radionuclide test, and control samples were run on each occasion to allow correction for this instability.
The appearance of tracer in venous blood was again more consistent between nuclides for HIgG than for HSA, with curves from pooled data suggesting a latent phase of approximately 20 min (as protein is carried up lymphatic vessels before draining into the venous system in the neck) followed by a steady increase in activity. Rates of appearance in blood were similar for HIgG and HSA, as observed previously (11), suggesting that the more rapid clearance of HSA from the depot is the result of poorer binding stability rather than the greater molecular size of HIgG (HSA vs. HIgG: molecular size, 69,000 Da vs. 150,000 Da, respectively; Stokes–Einstein radius, 3.55 nm vs. 5.5 nm, respectively).
Considering the future use of this technique for investigation into the pathophysiology of BCRL, studies of women with established edema are again hampered by the fact that a dilated lymphatic system will delay the appearance of protein in the blood even if lymphatic flow rate is unaltered; however, a subsequent rate of increase in activity should still provide useful information. The technique may prove more valuable in the prospective investigation of women undergoing surgery for breast cancer. Studies performed before and after surgery may identify changes in lymphatic behavior that, even in the absence of arm swelling, may reflect the degree of lymphatic compensation and predict the subsequent development of edema. Given the striking degree of variation between individuals observed in this study, with a >3-fold difference between the highest and lowest rates of depot clearance and appearance in venous blood, it also will be interesting to investigate the possible predictive value of preoperative lymphatic clearance rates.
CONCLUSION
A dual-isotope technique relies on identical behavior of the 2 radiopharmaceuticals used. This study shows that this is the case with respect to HIgG but not HSA. 99mTc-HSA cleared faster than 111In-HSA and yet displayed better in vivo labeling stability. We conclude that 111In dissociates in the depot but then becomes locally bound. Using HIgG, a close correlation was observed between the rates of clearance from the depot and appearance in venous blood for 99mTc and 111In. This finding suggests that HIgG would be a suitable marker for subsequent dual-isotope studies on women with BCRL.
Acknowledgments
The authors are grateful to The Addenbrooke’s Charities Trust for financial support of this project.
Footnotes
Received Jul. 17, 2001; revision accepted Nov. 12, 2001.
For correspondence or reprints contact: Simon J. Pain, MA, Cambridge Breast Unit, Box 97, Addenbrooke’s Hospital, Hills Rd., Cambridge CB2 2QQ, United Kingdom.
E-mail: amy.byrtus{at}addenbrookes.nhs.uk