

Abstract
Nonspecific 131I uptake may affect both the specificity and the accuracy of whole-body scanning (WBS) performed after 131I administration in the follow-up of thyroid carcinoma after thyroidectomy. We report a newly identified cause of false-positive WBS findings: posttraumatic superficial scabs. Methods: Four patients who underwent thyroidectomy for differentiated thyroid carcinoma were studied after therapeutic administration of 3,700 MBq 131I. Results: WBS revealed an area of uptake in the lower limbs, in a site corresponding to a slight abrasion of the skin that had incidentally occurred between a few hours before and 24 h after radioiodine administration. In 2 patients, a radioiodine concentration in the scab was shown by the disappearance of the radioactivity in the leg after removal of the scab and by detection of radioactivity in the collected material. Conclusion: Posttraumatic superficial scabs may be a cause of false-positive WBS findings. High 131I doses, although providing increased sensitivity, may also increase the number of false-positive results.
- thyroid carcinoma
- 131I
- whole-body scan
- false-positive
- scab
Whole-body scanning (WBS) with 131I and serum thyroglobulin measurement (Tg) are the 2 main investigations used to detect residual thyroid tissue and local or distant metastases after thyroidectomy for differentiated thyroid cancer (DTC). WBS and Tg are usually concordant but in some instances may be discordant. In particular, a negative WBS result in the presence of a positive Tg result is usually interpreted as false-negative because of an insufficient 131I concentration in malignant tissue (1). To increase sensitivity, WBS is frequently performed after therapeutic administration of radioiodine (3,700–5,500 MBq). By this procedure, even small foci of 131I accumulation may be revealed (2).
Several reports have described a variety of tissues or pathologic processes associated with nonspecific 131I uptake (3). Here, we report a newly identified cause of false-positive WBS findings after administration of 3,700 MBq 131I to thyroid cancer patients: A posttraumatic superficial scab resulting from a small cutaneous cut was a site of increased 131I concentration detected on posttherapeutic WBS.
MATERIALS AND METHODS
Four women (age range, 34–59 y) who had undergone thyroidectomy for DTC were studied. The surgery had included paratracheal lymphoadenectomy in patient 1 and paratracheal lymphoadenectomy plus left cervical lymphoadenectomy in patient 2. At histology, patients 1–3 had a papillary carcinoma and patient 4 had a follicular carcinoma. The patients’ clinical data are summarized in Table 1. They were scheduled for our routine DTC follow-up, which includes WBS and Tg after l-thyroxine withdrawal and neck sonography.
Clinical Characteristics of 4 Patients Followed Up After Thyroidectomy for DTC
At the time of the study, all patients were clearly hypothyroid as indicated by their high thyroid-stimulating hormone (TSH) levels (range, 65–98 μU/mL; reference range, 0.3–3.4 μU/mL). All patients received an oral dose of 3,700 MBq 131I (for patients 2 and 4, this was the second radioiodine treatment in their DTC follow-up). WBS was performed on a STARCAM 4000 gamma camera (General Electric Medical Systems, Milwaukee, WI), using a high-energy collimator, 5–7 d after radioiodine administration.
Serum TSH and Tg were measured by immunoradiometric assay, using commercial kits.
Radioactivity in scabs was measured with an automatic γ-counter (Kontron Analytical, Basel, Switzerland) with a counting efficiency of 85%. The coefficient of variation for the measurements was 2.0% on 10 replicates. The sensitivity was 12.3 Bq.
RESULTS
Postsurgical WBS revealed a focus of 131I uptake in the thyroid bed of patient 1, multiple foci of uptake in the neck of patient 2, 1 area of uptake above the suprasternal notch of patient 3, and 2 foci of uptake in the thyroid bed of patient 4. The Tg result was negative in patient 1 (<1.0 ng/mL) and positive in patients 2–4 (range, 11–67 ng/mL; reference range after total thyroidectomy, <3.0 ng/mL). In addition to these areas of uptake, in all 4 patients WBS revealed another focus of 131I accumulation that could not be attributed to a distant metastasis.
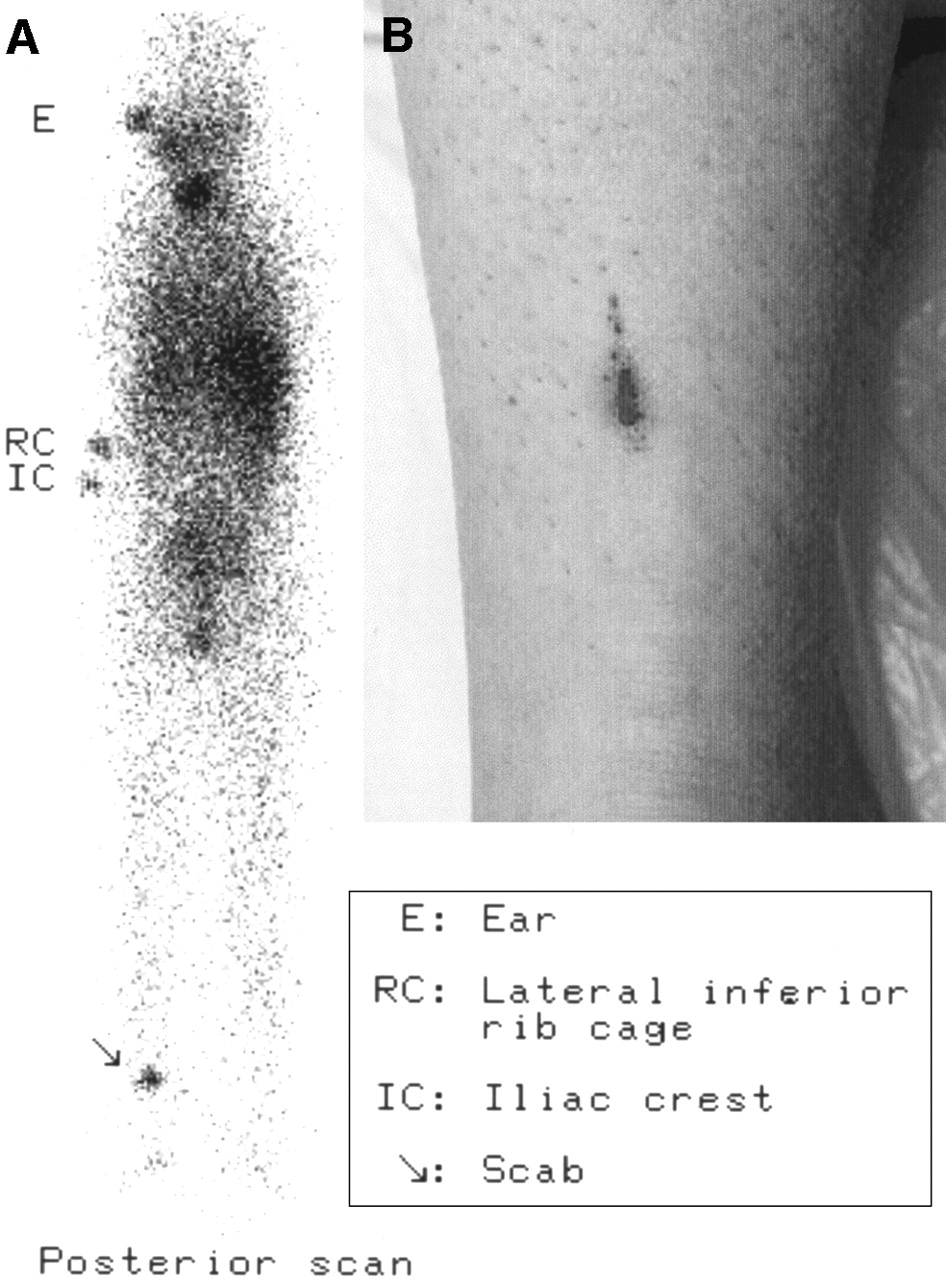
In patient 1, a small area was detected in the left leg and was more evident on the posterior scan (Fig. 1A). Inspection showed a superficial cut with a small, organized scab (Fig. 1B). A few hours after radioiodine administration, the patient had incidentally cut herself there while shaving with a razor. The scab was carefully removed with a surgical blade and collected in a plastic tube. An immediately repeated scan of the leg showed that the positive area had disappeared. Radioactivity counting of the collected material revealed an activity of 74 kBq 131I (0.0031% of the administered dose, corrected for radioisotope decay at the time of WBS).

(A) Posterior scan after 3,700 MBq 131I were administered to patient 1 shows focus of uptake (arrow) in lower third of left leg on lateral side. (B) Photograph shows lateral view of cutaneous lesion in same area.
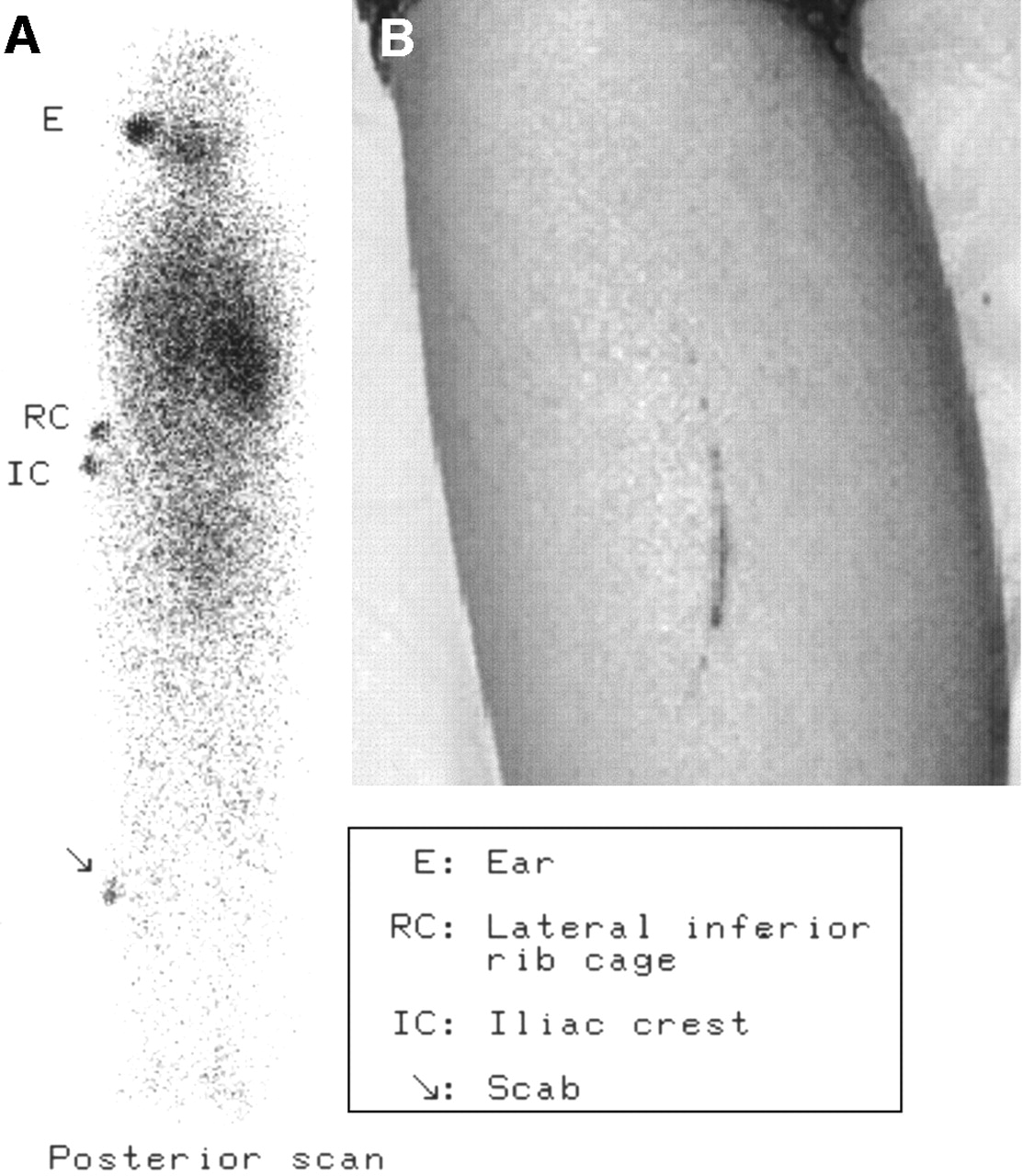
In patient 2, an area of uptake was present in the lower third of the left leg (Fig. 2A). A slight abrasion of the skin, with a thin scab, was visible at this site (Fig. 2B). The patient reported that a thorn from a rosebush had grazed her leg at that site a few hours before she received the 131I. As had been done for patient 1, the scab was removed and collected in a plastic tube. The area of uptake immediately disappeared on WBS, whereas the collected material showed an activity of 111 kBq (0.0046% of the administered dose).
{kind=link}
{kind=link}
(A) Posterior scan after 3,700 MBq 131I were administered to patient 2 shows focus of uptake (arrow) in lower third of left leg. (B) Photograph shows cutaneous lesion in same area.
In patient 3, a positive area was detected at the middle third of the right leg and was more visible on the anterior scan. At inspection, a thin, 2- to 3-cm-long cutaneous reddish scab was visible at this site. Six days earlier (12 h after radioiodine administration), through incidental trauma, the patient had slightly cut herself.
In patient 4, a distinct focus of uptake was detected at the level of the right knee, on the anterior side. Sweat or clothing contamination was ruled out. Clearly visible at that site was a small scab, which had resulted from an incidental fall a few hours before radioiodine administration.
DISCUSSION
False-positive 131I WBS findings mimicking metastases of differentiated thyroid carcinoma have long been reported. In a recent review, Shapiro et al. (3) provided a classification and organization system for artifacts, anatomic and physiologic variants, and nonthyroidal pathologic processes that may cause false-positive 131I WBS results in patients followed up for thyroid carcinoma.
We report here a newly identified cause of false-positive WBS findings: posttraumatic scabs. In all 4 patients described, an abnormal accumulation of radioiodine was observed on the leg after administration of 3,700 MBq 131I. In all patients, the 131I uptake was localized at the site of a superficial skin abrasion that occurred between a few hours before and 12 h after radioiodine administration and was followed by formation of a scab. In all patients, bone metastasis in the leg was unlikely and a nonspecific, artifactual 131I accumulation was readily suspected. Clinical history, imaging findings, and the immediate disappearance of the positive area after scab removal from patients 1 and 2 confirmed that the positive WBS findings had been artifactual. In these 2 patients, a concentration of radioiodine in the collected scab was shown by measuring the radioactivity in it.
Two mechanisms may contribute to the false-positive findings. First, the accumulation of 131I may result from the inflammatory reaction after the trauma. In fact, vasodilation, increased capillary permeability, and humoral and cellular mediators of inflammation may together result in increased delivery of 131I to the injured area (3). Second, the clot giving rise to the WBS artifact may be rich in leukocytes, which have been reported to be able to induce iodide organification by means of a myeloperoxidase (4). Iodination of bacteria may be part of the antibacterial effect of white blood cells (5). Retention of 131I in the leukocytes of posttraumatic clots, therefore, may also explain our false-positive WBS findings. Finally, the possibility of an unidentified iodinated protein involved in the process of blood coagulation cannot be ruled out.
CONCLUSION
Our findings suggest that similar false-positive results are possible when subcutaneous or internal trauma gives origin to ecchymosis or bleeding shortly before or after 131I administration. This condition may not be readily recognizable and may cause serious diagnostic artifacts. This new type of false-positive 131I WBS result should be taken into account to avoid inappropriate diagnostic or therapeutic approaches.
Acknowledgments
The authors thank Euplio Rascunà for his excellent technical assistance.
Footnotes
Received Jul. 19, 2001; revision accepted Oct. 22, 2001.
For correspondence or reprints contact: Concetto Regalbuto, MD, Istituto di Medicina Interna e Malattie Endocrine e del Metabolismo, Ospedale Garibaldi, Università di Catania, Piazza Santa Maria di Gesù, 95123 Catania, Italy.
E-mail: segmeint{at}mbox.unict.it