


Visual Abstract
Abstract
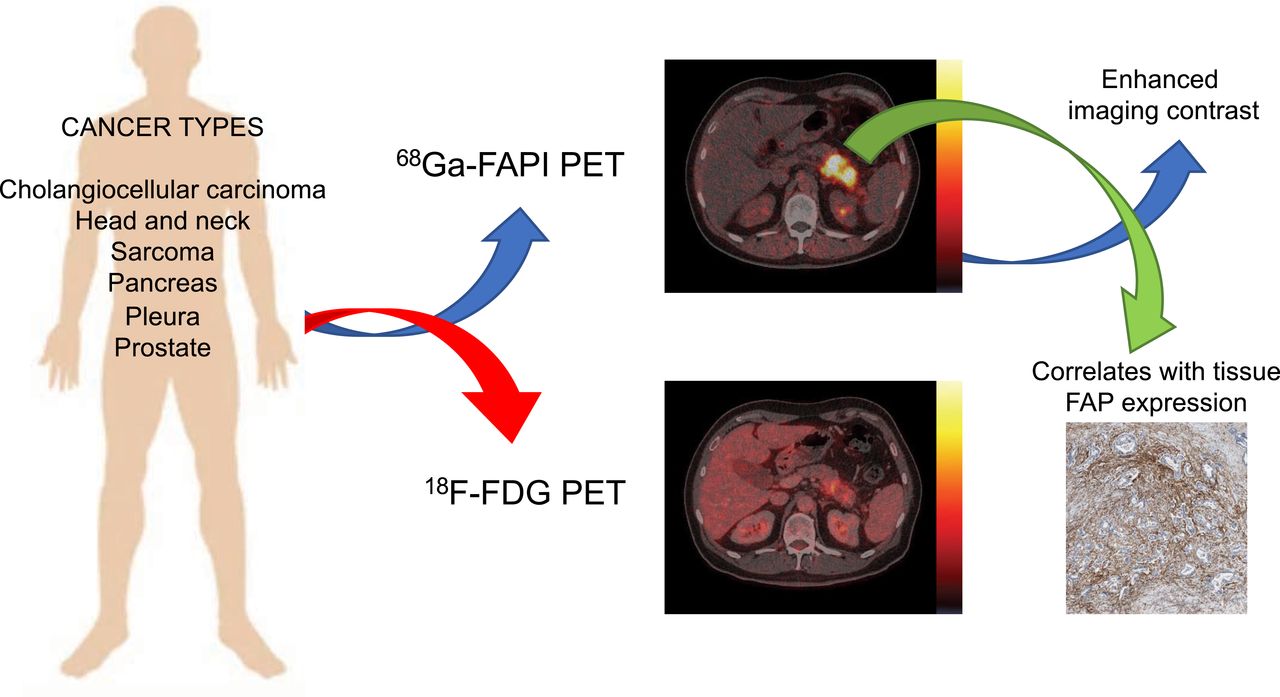
We present an overview of our prospective fibroblast-activation protein inhibitor (FAPI) registry study across a 3-y period, with head-to-head comparison of tumor uptake in 68Ga-FAPI and 18F-FDG PET, as well as FAP immunohistochemistry. Methods: This is an interim analysis of the ongoing 68Ga-FAPI PET prospective observational trial at our department. Patients who underwent clinical imaging with 68Ga-FAPI PET between October 2018 and October 2021 were included. Tracer uptake was quantified by SUVmax for tumor lesions and by SUVmean for normal organs. PET tumor volume (40% isocontour) and tumor-to-background ratios were calculated. Correlation between SUVmax and FAP staining in tissue samples was analyzed. Results: In total, 324 patients with 21 different tumor entities underwent 68Ga-FAPI imaging; 237 patients additionally received 18F-FDG PET. The most common tumor entities were sarcoma (131/324, 40%), pancreatic cancer (67/324, 21%), and primary tumors of the brain (22/324, 7%). The mean primary tumor SUVmax was significantly higher for 68Ga-FAPI than 18F-FDG among pancreatic cancer (13.2 vs. 6.1, P < 0.001) and sarcoma (14.3 vs. 9.4, P < 0.001), and the same was true for mean SUVmax in metastatic lesions of pancreatic cancer (9.4 vs. 5.5, P < 0.001). Mean primary tumor maximum tumor-to-background ratio was significantly higher for 68Ga-FAPI than 18F-FDG across several tumor entities, most prominently pancreatic cancer (14.7 vs. 3.0, P < 0.001) and sarcoma (17.3 vs. 4.7, P < 0.001). Compared with 18F-FDG, 68Ga-FAPI showed superior detection for locoregional disease in sarcoma (52 vs. 48 total regions detected) and for distant metastatic disease in both sarcoma (137 vs. 131) and pancreatic cancer (65 vs. 57), respectively. Among 61 histopathology samples, there was a positive correlation between 68Ga-FAPI SUVmax and overall FAP immunohistochemistry score (r = 0.352, P = 0.005). Conclusion: 68Ga-FAPI demonstrates higher absolute uptake in pancreatic cancer and sarcoma, as well as higher tumor-to-background uptake along with improved tumor detection for pancreatic cancer, sarcoma, and other tumor entities when compared with 18F-FDG. 68Ga-FAPI is a new tool for tumor staging with theranostic potential.
Imaging is critically important in the diagnosis and staging of malignancies, with varying detection rates depending on the tumor entity and diagnostic modality. PET of cancer cells using 18F-FDG PET acquires additional molecular information useful for the management of disease and for improving treatment outcomes (1–3).
Tumor growth and spread are determined not only by cancer cells but also by the tumor microenvironment, which contains several nonmalignant components. Besides immune cells, important constituents are cancer-associated fibroblasts, which are known to be involved in tumor growth, migration, and progression (4). Although heterogeneous in their origin, cancer-associated fibroblasts have common properties that are distinct from normal fibroblasts, expressing proteins not found in their normal counterparts (5). A subpopulation of cancer-associated fibroblasts expresses, among other markers, fibroblast-activation protein (FAP) α (FAPα), which is associated with protumorigenic functions (6–10).
Therefore, these cells represent attractive diagnostic and therapeutic targets. Since 2018, preclinical and clinical data have emerged on a variety of FAP-directed therapies, including radiolabeled, low-molecular-weight FAP inhibitors (FAPIs), further underlining their favorable properties in diagnosis and therapy (11–15).
Data for the superiority of 68Ga-FAPI PET over conventional imaging have been reported previously in small cohorts (13,16). On the basis of the favorable imaging characteristics of 68Ga-FAPI PET, patients were referred for clinical 68Ga-FAPI PET staging both at initial diagnosis and after intervention and were offered enrollment in our prospective observational 68Ga-FAPI registry. Clinical indications for 68Ga-FAPI PET were staging of disease in high-risk patients, evaluation of the localization of tumor lesions before biopsy or surgery, further workup of equivocal imaging results, or evaluation of therapeutic options.
In this report, we present the largest cohort to date (to our knowledge), with an overview of the tumor entities diagnosed and staged with 68Ga-FAPI across a 3-y period, including head-to-head comparison of tumor uptake in 68Ga-FAPI and 18F-FDG PET, as well as FAP immunohistochemistry.
MATERIALS AND METHODS
Study Design and Participants
Patients underwent imaging with 68Ga-FAPI PET between October 2018 and October 2021 at the Department of Nuclear Medicine at the University Hospital Essen. This is an interim analysis of the ongoing 68Ga-FAPI PET observational trial conducted at the University Hospital Essen (NCT04571086). Until October 2021, adult patients who underwent clinical 68Ga-FAPI PET were offered the possibility to consent to a prospective observational trial for correlation and clinical follow-up of PET findings. Evaluation of data was approved by the ethics committee of the University Duisburg–Essen (approvals 20-9485-BO and 19-8991-BO). Patient subgroups have been reported in previous publications (n = 47 (17), n = 69 (18), and n = 91 (19)).
Details of data collection (20–22); imaging and administration of radioligands (18,23,24); imaging analysis, immunohistochemistry, and FAP scoring (17,25); and statistical analysis (26) are provided in the supplemental materials (available at http://jnm.snmjournals.org).
RESULTS
Patient Characteristics
Three hundred twenty-four patients were included; their characteristics are outlined in Table 1. The median age was 59 y (interquartile range, 16 y). The most common tumor entity was sarcoma (131/324, 40%), followed by primary tumors of the pancreas (67/324, 21%), brain (22/324, 7%), and lung (14/324, 4%) and pleural mesothelioma (12/324, 4%). Most patients (235/324, 73%) underwent 68Ga-FAPI PET imaging for restaging purposes. A breakdown of histopathologic diagnoses, as well as the presence of primary and metastatic lesions for each category, is provided in Supplemental Table 1.
Patient Characteristics (n = 324)
Tumor Diagnostics and 68Ga-FAPI PET
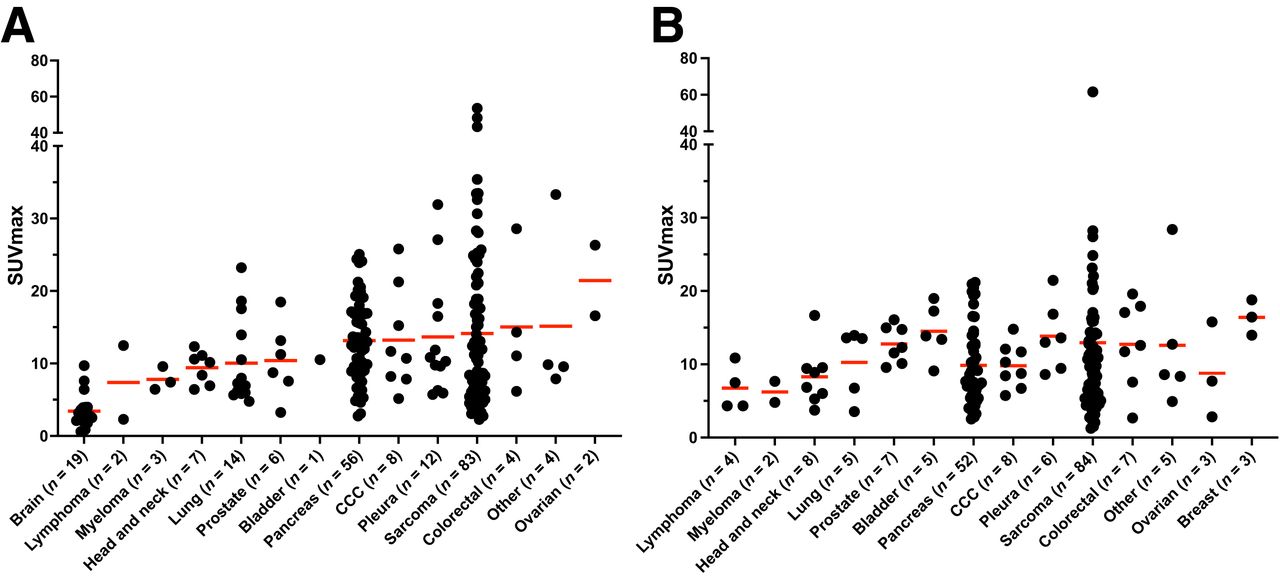
The mean SUVmax for primary lesions and metastatic lesions on 68Ga-FAPI PET is shown in Figures 1A and 1B, respectively. Mean values of primary tumor SUVmax ranged from 3.41 for brain tumors to 21.44 for ovarian tumors. The mean primary tumor SUVmax was higher than 10 for 9 of 17 (53%) tumor entities with primary lesions, including prostate (10.4), bladder (10.5), pancreas (13.2), and sarcoma (14.1), among others. The mean SUVmax for primary lesions and metastatic lesions using broader subgroups is provided in Supplemental Figure 1.

Mean SUVmax on 68Ga-FAPI PET for primary lesions (n = 221) (A) and hottest metastatic lesions per patient (n = 199) (B). Data points represent hottest lesions for individual patients. Data in A and B were sorted by mean SUVmax in A. Numbers of patients included for every tumor entity are given on x-axis. Red lines represent mean values. y-axis is split to account for extreme values. Primary and metastatic lesions for every tumor entity are provided in Supplemental Table 1.
Staging by 68Ga-FAPI PET is presented in Supplemental Figure 2 for the 7 most common tumor entities in our registry (with at least 10 patients, excluding brain tumors). In our prospective cohort, distant metastatic disease was detected in most patients with head and neck cancer (8/9, 89%), pancreatic cancer (44/67, 66%), sarcoma (79/122, 65%), colon or rectal cancer (7/11, 64%), prostate cancer (7/11, 64%), bladder cancer (5/8, 63%), and cholangiocellular carcinoma (CCC, 6/11, 55%). Locoregional-only disease was detected most often in lung carcinoma (11/14, 79%) and in pleural mesothelioma (9/12, 75%).
68Ga-FAPI PET Versus 18F-FDG PET Imaging
In our cohort, 237 of 324 patients (73%) had undergone additional 18F-FDG PET, and a head-to-head analysis of both imaging modalities was performed. Mean SUVmax was significantly higher for 68Ga-FAPI than for 18F-FDG PET among primary tumors of the pancreas (13.2 vs. 6.1, P < 0.001) and sarcoma (14.3 vs. 9.4, P < 0.001), as shown in Figure 2A. Similarly, the mean SUVmax in metastatic lesions was significantly higher for 68Ga-FAPI than for 18F-FDG in pancreatic cancer (9.4 vs. 5.5, P < 0.001; Fig. 2B).

Comparison of mean SUVmax for primary lesions (A) and metastatic lesions (B) between 68Ga-FAPI and 18F-FDG PET across tumor entities. Entities are arranged as presented in Figure 1. Mean and SD are presented for every bar. Two-tailed paired t test was performed. *P < 0.05. **P < 0.01. ***P < 0.001.
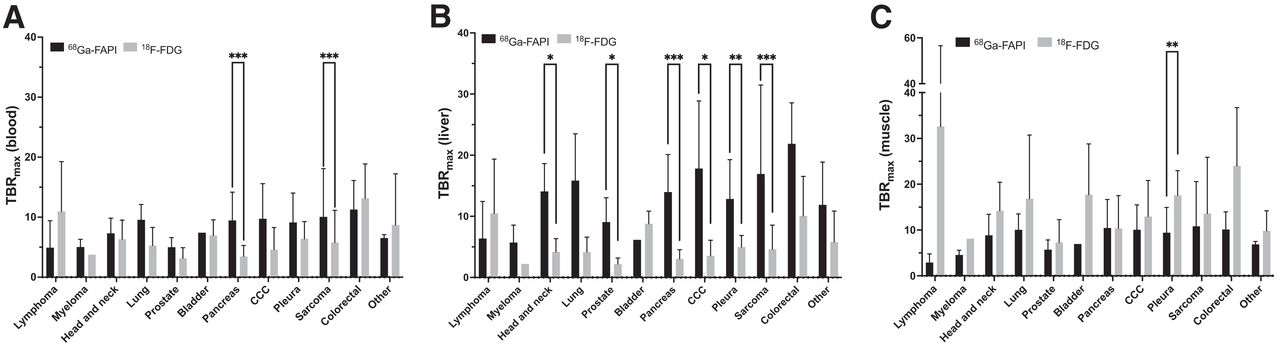
For primary tumors, mean tumor-to-background ratio (TBRmax) (with blood pool background) was significantly higher for 68Ga-FAPI than for 18F-FDG in pancreatic cancer (9.9 vs. 3.5, P < 0.001) and sarcoma (10.4 vs. 5.8, P < 0.001), as shown in Figure 3A. Mean TBRmax (with liver background) was also significantly higher for 68Ga-FAPI than for 18F-FDG in pancreatic cancer (14.7 vs. 3.0, P < 0.001) and sarcoma (17.3 vs. 4.7, P < 0.001), in addition to prostate cancer (7.8 vs. 2.7, P = 0.017), pleural mesothelioma (12.9 vs. 5.0, P = 0.003), head and neck cancer (14.5 vs. 4.2, P = 0.013), and CCC (19.5 vs. 3.6, P = 0.016), as shown in Figure 3B. Conversely, mean TBRmax (with muscle background) was significantly lower for 68Ga-FAPI than for 18F-FDG in pleural mesothelioma (9.4 vs. 17.6, P = 0.004; Fig. 3C).
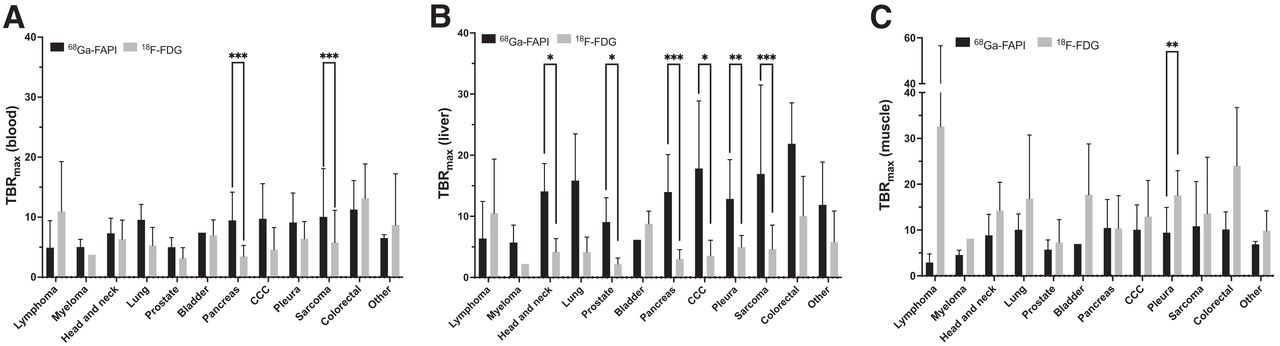
Comparison of mean TBRmax for primary lesions between 68Ga-FAPI and 18F-FDG PET across tumor entities, with different reference backgrounds (blood [A], liver [B], and muscle [C]). Entities are arranged as presented in Figure 1. Mean and SD are presented for every bar. Two-tailed paired t test was performed. *P < 0.05. **P < 0.01. ***P < 0.001.
For metastatic lesions, the mean TBRmax (with blood pool background) was significantly higher for 68Ga-FAPI than for 18F-FDG in pancreatic cancer (7.0 vs. 3.4, P < 0.001) and sarcoma (9.8 vs. 5.8, P = 0.028), as shown in Figure 4A. Mean TBRmax (with liver background) was also significantly higher for 68Ga-FAPI than for 18F-FDG in pancreatic cancer (10.6 vs. 2.8, P < 0.001) and sarcoma (18.9 vs. 4.7, P = 0.003), in addition to prostate cancer (15.1 vs. 4.9, P < 0.001), pleural mesothelioma (13.5 vs. 4.8, P = 0.017), and CCC (14.5 vs. 3.9, P = 0.012), as shown in Figure 4B. Conversely, mean TBRmax (with muscle background) was significantly lower for 68Ga-FAPI than for 18F-FDG in pleural mesothelioma (9.4 vs. 17.8, P = 0.027), prostate cancer (8.0 vs. 15.6, P = 0.009), and CCC (10.0 vs. 15.4, P = 0.024), as shown in Figure 4C.
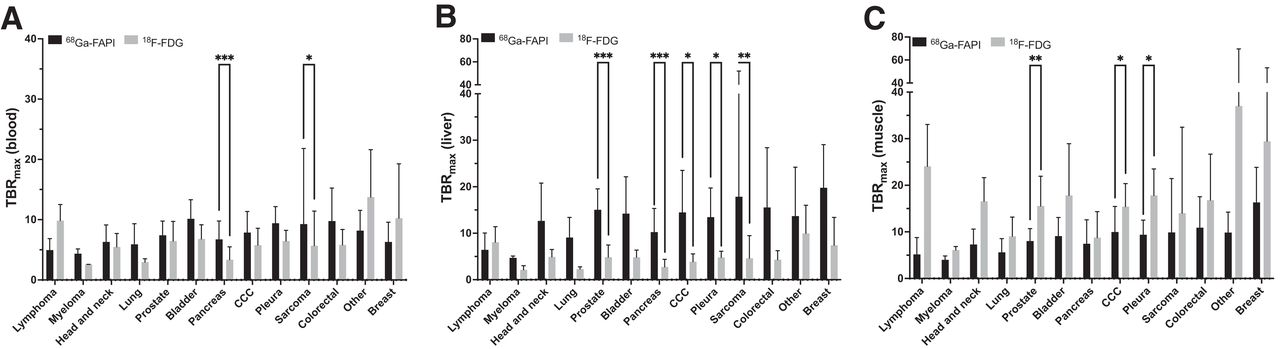
Comparison of mean TBRmax for metastatic lesions between 68Ga-FAPI and 18F-FDG PET across tumor entities, with different reference backgrounds (blood [A], liver [B], and muscle [C]). Entities are arranged as presented in Figure 1. Mean and SD are presented for every bar. Two-tailed paired t test was performed. *P < 0.05. **P < 0.01. ***P < 0.001.
There were no significant differences between metabolic tumor volumes measured for primary lesions and metastatic lesions in 68Ga-FAPI and 18F-FDG PET scans across tumor entities, as shown in Supplemental Figure 3.
Examples of 68Ga-FAPI and 18F-FDG PET scans showing tumor uptake and FAPα staining in tumor samples are presented in Supplemental Figures 4–8.
A comparison of primary SUVmax and involved regions between 68Ga-FAPI and 18F-FDG PET among metastatic and nonmetastatic disease and across tumor entities is provided in Supplemental Table 2. When compared with 18F-FDG, 68Ga-FAPI showed superior detection for locoregional disease in sarcoma (52 vs. 48 total regions detected) and for distant metastatic disease in sarcoma (137 vs. 131), pancreatic cancer (65 vs. 57), head and neck cancer (15 vs. 13), CCC (12 vs. 11), lung cancer (9 vs. 8), and bladder cancer (8 vs. 7). However, 68Ga-FAPI showed inferior detection of lymphoma compared with 18F-FDG (7 vs. 10).
Immunohistochemistry and FAP Scoring
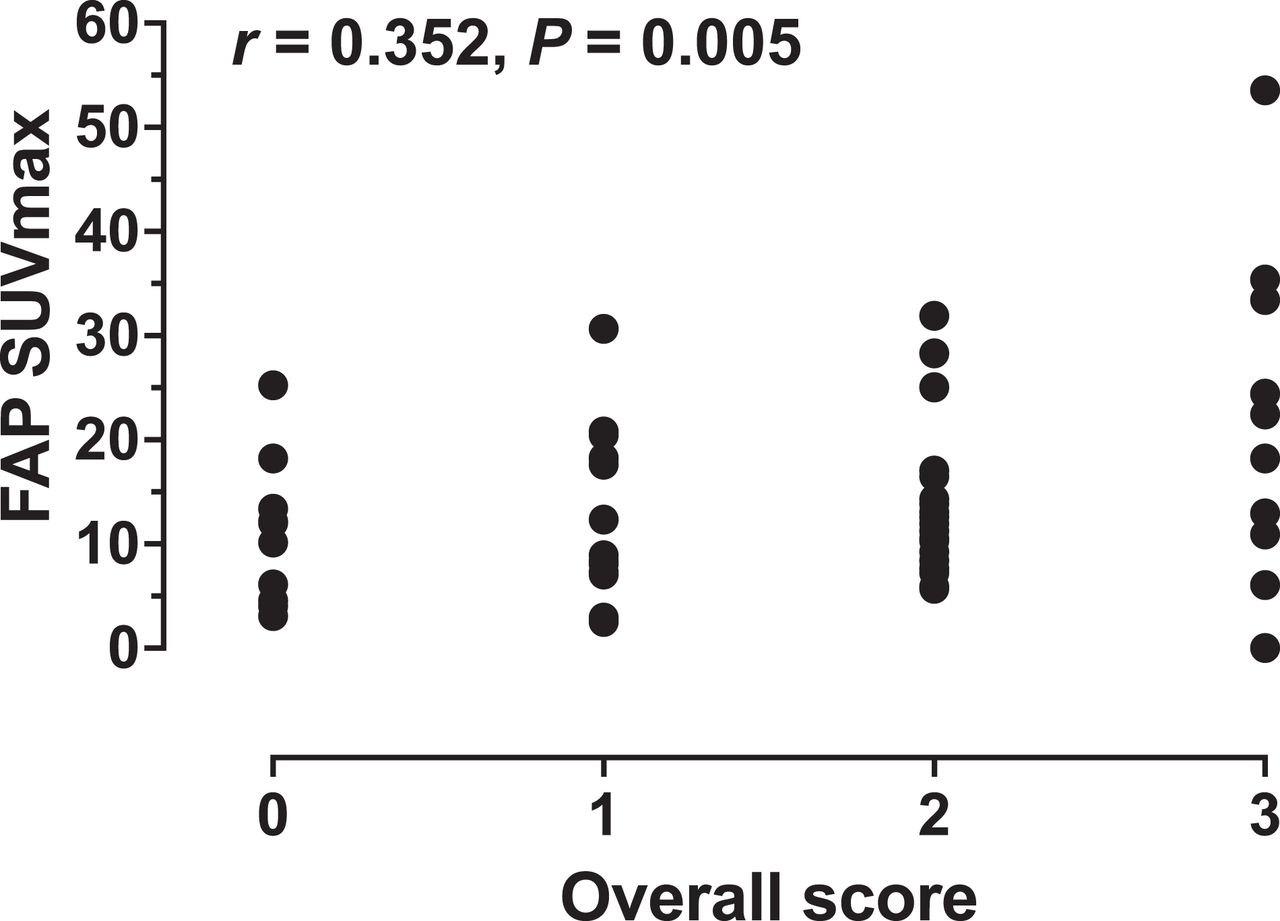
Sixty-one tissue samples dated within 3 mo from the date of 68Ga-FAPI PET (median, 20.5 d; interquartile range, 23 d) were analyzed and scored (sarcoma, n = 33; pancreas, n = 11; pleura, n = 5; urothelium, n = 4; colon or rectum, n = 3; head and neck, n = 3; prostate, n = 1; and lung, n = 1). The corresponding SUVmax on 68Ga-FAPI PET measured for the specific lesions biopsied before or after 68Ga-FAPI PET, or surgically removed after 68Ga-FAPI PET, were included in the correlation analysis. Across the 61 samples, there was a significant positive correlation between the overall score for FAPα immunohistochemistry and 68Ga-FAPI SUVmax (r = 0.352, P = 0.005, Fig. 5).
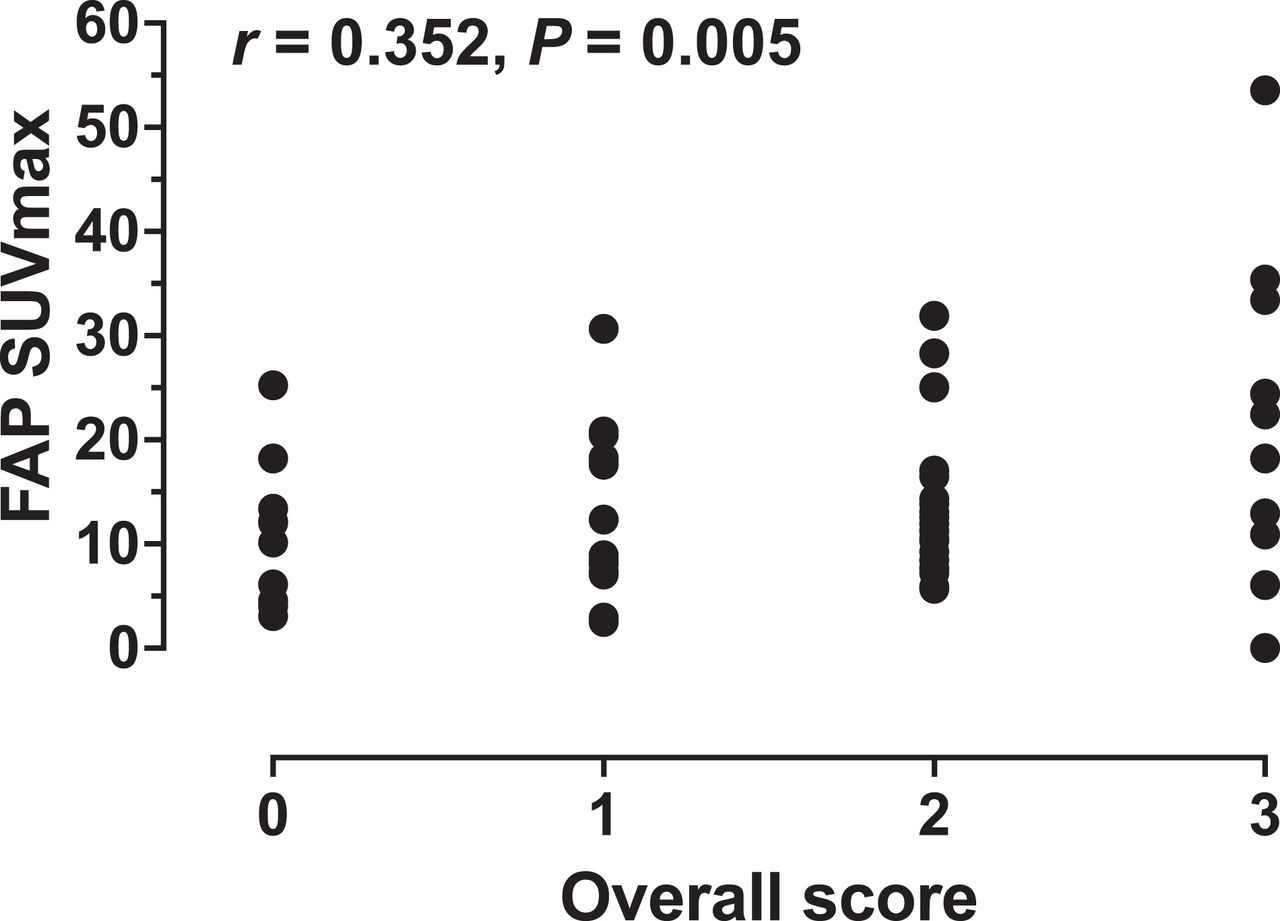
Correlation of 68Ga-FAPI SUVmax with overall score for FAP-immunohistochemistry samples within 3 mo from 68Ga-FAPI PET (n = 61). Overall FAP score refers to highest score assigned for tumor or stroma. r is Pearson correlation coefficient. Strength of correlation: negligible (0.00 < r ≤ ±0.29), low (±0.30 ≤ r ≤ ±0.49), moderate (±0.50 ≤ r ≤ ±0.69), or high (r ≥ ±0.70).
DISCUSSION
We report findings for 324 patients with 21 tumor entities diagnosed and staged by 68Ga-FAPI PET as part of our registry study over a 3-y period, with a head-to-head analysis of 68Ga-FAPI versus 18F-FDG PET uptake in tumor and metastatic lesions, as well as correlation between 68Ga-FAPI uptake and FAPα expression in tissue samples. This represents the largest cohort, to our knowledge, of patients examined with this novel imaging modality. Our results demonstrate higher tumor-to-liver uptake ratios for 68Ga-FAPI than for 18F-FDG in 6 of 14 (43%) of the evaluated tumor entities (most prominently sarcoma and pancreatic cancer, in addition to head and neck cancer, prostate cancer, CCC, and pleural mesothelioma) and comparable results in 8 of 14 (57%). Furthermore, we observed a positive correlation between radiotracer uptake and FAPα immunohistochemistry staining.
Relatively low 68Ga-FAPI uptake in normal parenchyma improves tumor delineation, especially in regions with high physiologic glucose uptake. Thus, 68Ga-FAPI demonstrates improved per-region tumor detection for pancreatic cancer, sarcoma, CCC, prostate cancer, pleural mesothelioma, and head and neck cancer when compared with 18F-FDG. As such, 68Ga-FAPI PET is a promising imaging modality for these entities, and it has the potential for more precise staging and management of patients, as well as theranostic screening.
68Ga-FAPI PET images the protein FAPα, which is located primarily on cancer-associated fibroblasts in the stroma, but this protein can also be found on tumor cells. High tumor uptake and low organ uptake support the potential use of FAPI ligands in a therapeutic context, particularly for sarcoma and pancreatic cancer. Use of FAP-directed radioligand therapy has been reported to be feasible for breast cancer (11), ovarian cancer (27), and sarcoma and pancreatic cancer (15,28), as well as multiple advanced and refractory tumors (14,29,30). All applications of FAP-directed radioligand therapy relied on baseline patient selection by high uptake on 68Ga-FAPI PET. In addition, FAP-targeting drugs have been showing clinical promise across various tumor entities; 1 prominent example is talabostat, which has shown tumor control in 21% of patients with colorectal cancer (31). As such, future drug developments and their potential clinical applications may be enhanced through 68Ga-FAPI imaging, which aids in selecting patients whose tumors exhibit high 68Ga-FAPI uptake and low glycolytic phenotypes and who would potentially benefit from FAP-directed radioligand therapy.
Another ongoing clinical trial at our department (NCT05160051) aims to explore the diagnostic accuracy of 68Ga-FAPI-46 PET and its impact on management and interreader reproducibility for different FAP-expressing tumor entities. Here, tumor samples will be collected within 8 wk from the time of the 68Ga-FAPI PET scan to better elucidate the correlation between 68Ga-FAPI-46 uptake intensity and histopathologic FAP expression.
Our analysis has several limitations. SUV for 68Ga-FAPI is reproducible at different time points (18) and is routinely measured but not yet a well-established metric. In addition, for some patient subgroups, there were low sample sizes and a referral bias. We report SUVs from different PET devices; despite cross calibration based on European Association of Nuclear Medicine Research Ltd. standards, SUV deviations may have occurred but were not statistically significantly (e.g., random samples with equal numbers of patients, P = 0.949). Moreover, the fact that quantitative immunohistochemistry assessment across all planes of whole-mount pathology specimens was not feasible may have led to deviations between 68Ga-FAPI SUVmax and immunohistochemistry scores.
CONCLUSION
When compared with 18F-FDG, 68Ga-FAPI demonstrates higher absolute uptake in pancreatic cancer and sarcoma, as well as higher tumor-to-background uptake along with improved tumor detection for pancreatic cancer, sarcoma, CCC, prostate cancer, pleural mesothelioma, and head and neck cancer. A prospective clinical trial at our department (NCT05160051) is currently under way.
DISCLOSURE
Rainer Hamacher is supported by the Clinician Scientist Program of the University Medicine Essen Clinician Scientist Academy (UMEA) sponsored by the faculty of medicine and Deutsche Forschungsgemeinschaft (DFG) and has received travel grants from Lilly, Novartis, and Pharma Mar, as well as fees from Lilly and Pharma Mar. Lukas Kessler is a consultant for AAA and BTG and received fees from Sanofi. Kim Pabst has received a Junior Clinician Scientist Stipend of UMEA sponsored by the Faculty of Medicine at the University of Duisburg–Essen and DFG, and he has received research funding from Bayer outside the submitted work. Katharina Lueckerath is a consultant for Sofie Biosciences and receives research funding from Curie Therapeutics. Stefan Kasper reports personal fees and grants from AstraZeneca, Merck Serone, Merck Sharpe & Dohme, Amgen, Bristol Myers Squibb, Roche, Lilly, Servier, Incyte, and SanofiAventis outside the submitted work. Claudia Kesch has received consultant fees from Apogepha, research funding from AAA/Novartis and Curie Therapeutics, and compensation for travel from Janssen R&D. Bastian von Tresckow is an advisor or consultant for Allogene, BMS/Celgene, Cerus, Incyte, Miltenyi, Novartis, Pentixafarm, Roche, Amgen, Pfizer, Takeda, Merck Sharp & Dohme, and Gilead Kite; has received honoraria from AstraZeneca, Novartis, Roche Pharma AG, Takeda, and Merck Sharp & Dohme; reports research funding from Novartis, Merck Sharp & Dohme, and Takeda; and reports travel support from AbbVie, AstraZeneca, Kite-Gilead, Merck Sharp & Dohme, Takeda, and Novartis. Christine Hanoun received honoraria from BMS, Takeda, and AstraZeneca; travel grants from AbbVie; and research funding from Novartis. Hubertus Hautzel reports research funding and travel support from PARI GmbH outside the submitted work. Ken Herrmann reports personal fees from Bayer, SIRTEX, Adacap, Curium, Endocyte, IPSEN, Siemens Healthineers, GE Healthcare, Amgen, Novartis, ymabs, Aktis, Oncology, and Pharma15, as well as personal and other fees from Sofie Biosciences, nonfinancial support from ABX, and grants and personal fees from BTG, all of which are outside the submitted work. Boris Hadaschik has had advisory roles for ABX, AAA/Novartis, Astellas, AstraZeneca, Bayer, Bristol Myers Squibb, Janssen R&D, Lightpoint Medical, Inc., and Pfizer; has received research funding from Astellas, Bristol Myers Squibb, AAA/Novartis, the German Research Foundation, Janssen R&D, and Pfizer; and has received compensation for travel from Astellas, AstraZeneca, Bayer, and Janssen R&D. Philipp Harter reports grants, personal fees, and nonfinancial support from Astra Zeneca and GSK; grants and personal fees from Roche, MSD, Clovis, and Immunogen; personal fees from Mersana, Sotio, Stryker, and Zai Lab; and grants from Boehringer Ingelheim, Medac, Genmab, Deutsche Krebshilfe, Deutsche Forschungsgemeinschaft, and the European Union, all of which are outside the submitted work. Jens T. Siveke received honoraria as a consultant or for continuing medical education presentations from AstraZeneca, Bayer, Bristol-Myers Squibb, Eisbach Bio, Immunocore, Novartis, Roche/Genentech, and Servier; his institution receives research funding from Bristol-Myers Squibb, Celgene, Eisbach Bio, and Roche/Genentech, and he holds ownership and serves on the Board of Directors of Pharma15, all outside the submitted work. Wolfgang Fendler reports fees from SOFIE Bioscience (research funding), Janssen (consultant, speakers’ bureau), Calyx (consultant), Bayer (consultant, speakers’ bureau, research funding), and Parexel (image review), as well as financial support from Mercator Research Center Ruhr (MERCUR, An-2019-0001), IFORES (D/107=81260, D/107=30240), and Wiedenfeld-Stiftung/Stiftung Krebsforschung Duisburg, all outside the submitted work. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the 68Ga-FAPI PET uptake for different tumor entities?
PERTINENT FINDINGS: Mean SUVmax was significantly higher for 68Ga-FAPI than for 18F-FDG in primary and metastatic pancreatic cancer lesions and in sarcoma. Mean TBRmax in primary lesions was better for 68Ga-FAPI than for 18F-FDG in sarcoma, CCC, and cancers of the head and neck, prostate, pancreas, and pleura and was comparable for the remaining entities. Radiotracer uptake correlated positively with FAP expression levels in tissue samples. 68Ga-FAPI was superior to 18F-FDG in detecting locoregional disease in sarcoma and distant metastatic disease in sarcoma, CCC, and cancers of the pancreas, head and neck, lung, and bladder.
IMPLICATIONS FOR PATIENT CARE: 68Ga-FAPI PET offers theranostic screening and has the potential for more precise staging and management of patients with these entities.
Footnotes
Published online Dec. 29, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 18, 2022.
- Revision received November 8, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diagnostic Accuracy of 68Ga-FAPI Versus 18F-FDG PET in Patients with Various Malignancies
- Design, Preclinical Evaluation, and Clinical Translation of 68Ga-FAPI-LM3, a Heterobivalent Molecule for PET Imaging of Nasopharyngeal Carcinoma
- Fibroblast Activation Protein {alpha}-Directed Imaging and Therapy of Solitary Fibrous Tumor
- Molecular Imaging Biomarkers in Cardiooncology: A View on Established Technologies and Future Perspectives
- Comparison of Baseline 68Ga-FAPI and 18F-FDG PET/CT for Prediction of Response and Clinical Outcome in Patients with Unresectable Hepatocellular Carcinoma Treated with PD-1 Inhibitor and Lenvatinib
- Tumor Characterization by [68Ga]FAPI-46 PET/CT Can Improve Treatment Selection for Pancreatic Cancer Patients: An Interim Analysis of a Prospective Clinical Trial