


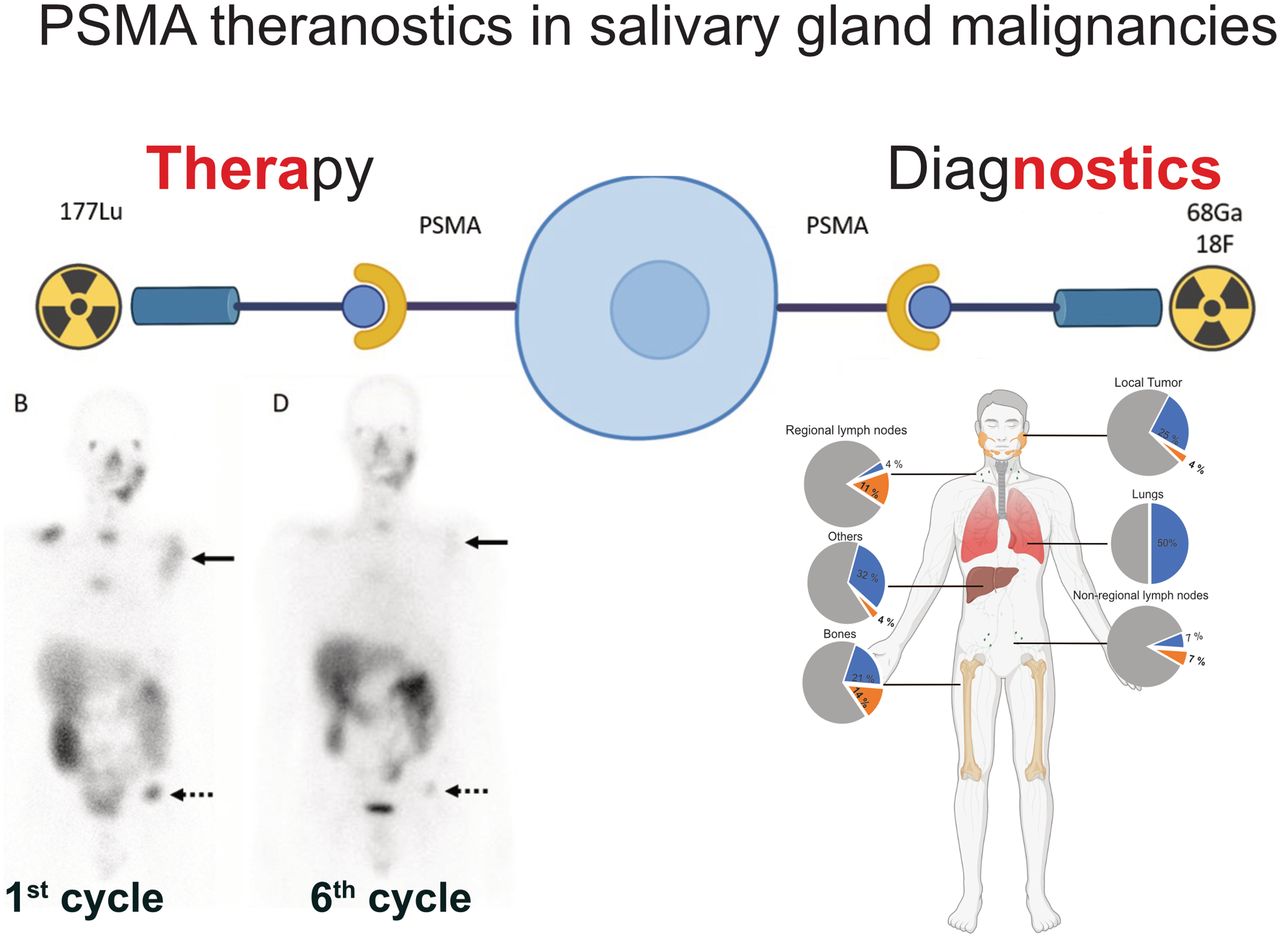
Visual Abstract

Abstract
We analyzed the diagnostic performance of prostate-specific membrane antigen (PSMA) PET/CT and the dosimetry, efficacy, and safety of 177Lu-PSMA-617 radioligand therapy (RLT) in salivary gland malignancies (SGMs). Methods: We identified 28 SGM patients with PSMA PET/CT from our database. CT and PSMA PET/CT images were evaluated separately by 3 masked readers in joint reading sessions. Pathologic findings were grouped into 6 TNM regions, and lesion-based disease extent was classified as no disease (n = 1, 4%), unifocal (n = 2, 7%), oligometastatic (n = 9, 32%), multifocal (n = 3, 11%), or disseminated (n = 13, 47%). For each region, the SUVmax of the lesion with the highest uptake was measured and the visual PSMA expression score was evaluated on a per-patient basis using PROMISE criteria. The association between PSMA expression and clinical and histopathologic markers was tested using the Student t test. Five patients underwent PSMA RLT with intratherapeutic dosimetry. Response was assessed using RECIST 1.1, and adverse events were graded according to version 5.0 of the Common Terminology Criteria for Adverse Events. Results: Compared with CT, PSMA PET/CT demonstrated additional metastatic lesions in 11 of 28 (39%) patients, leading to upstaging of TNM and lesion-based disease extent in 3 (11%) and 6 (21%) patients, respectively. PSMA PET/CT detected CT-occult local tumor, regional lymph nodes, nonregional lymph nodes, and bone metastases in 1 (4%), 4 (14%), 2 (7%), and 4 (14%) patients, respectively; no additional lesions were detected in the other predefined regions. PSMA expression level was higher than liver in 6 patients (25%). A significantly higher SUVmax was observed in male than female patients (15.8 vs. 8.5, P = 0.007) and in bone than lung lesions (14.2 vs. 6.4, P = 0.006). PSMA RLT was discontinued after 1 cycle in 3 of 5 patients because of insufficient tumor doses. No adverse events of grade 4 or higher occurred. Conclusion: In SGMs, PSMA PET/CT demonstrated a superior detection rate and led to upstaging in about one third of patients when compared with CT. The male sex and the presence of bone metastases were associated with significantly higher PSMA expression. PSMA RLT was well tolerated, but most patients did not have more than 1 cycle because of insufficient tumor doses.
Salivary gland malignancies (SGMs) are rare head and neck tumors that encompass 24 different histologic subtypes, with mucoepidermoid carcinoma and adenoid cystic carcinoma (ACC) being the most frequent (1–3). SGMs most commonly originate from the parotid, submandibular, and sublingual glands and are characterized by slow growth and an indolent course but tend to show multiple recurrences and distant metastases (4). Although survival outcomes have improved with surgery and postoperative radiotherapy in early and locally advanced stages of the disease, there is no consensus on systemic treatments in recurrent or metastatic disease (5). No further standard treatment has yet been established for recurrent or metastatic disease. SGMs show a high intrinsic resistance to classic cytotoxic drugs. Recently, small phase II trials demonstrated the tyrosine kinase inhibitors lenvatinib or axitinib to have activity in ACC (6,7). Further, for a subset of patients with such specific genetic alteration as NTRK fusions, BRAF mutations, or Her2/neu amplifications, molecule-targeted therapies are available (8,9). However, for most patients, no molecule-targeted therapies are available, and those patients are treated mostly with the cytotoxic drugs cisplatin, taxanes, anthracyclines, cyclophosphamide, or 5-fluororuacil, with only a moderate response rate. Taken together, there is a huge unmet medical need to improve the palliative treatment of patients with recurrent or metastatic SGMs.
Routine imaging is performed using MRI and CT (10). Additional 18F-FDG PET can increase sensitivity, especially with regard to N or M stage, impacting therapy management in 12.5% of cases (11). Furthermore, recent immunohistochemical and PET imaging studies have shown increased prostate-specific membrane antigen (PSMA) expression in ACC, implying that PSMA-targeted imaging may improve staging accuracy and that 177Lu-PSMA-617 radioligand therapy (RLT) can be feasible in a theranostic setup (12–15).
The aim of this study was to investigate the diagnostic role of PSMA PET/CT and the safety, feasibility, and efficacy of PSMA RLT in patients with SGM.
MATERIALS AND METHODS
Eligibility Criteria
Our institutional database was screened for SGM patients undergoing PSMA PET/CT from May 2015 to October 2021. All patients gave written informed consent to undergo clinical PSMA imaging or therapy. The retrospective analysis of available data was approved by the local institutional review board, and the requirement to obtain informed consent was waived (University of Duisburg–Essen, medical faculty, protocol 21-10370-BO).
PSMA PET/CT Image Acquisition
Values are presented as median and interquartile range. Images were acquired in accordance with the joint procedure guidelines of the European Association of Nuclear Medicine and the Society of Nuclear Medicine and Molecular Imaging: 63 min (26 min) or 98 min (21 min) after the administration of 116 MBq (44.5 MBq) of 68Ga-PSMA-11 (n = 21, 75%) or 281 MBq (97 MBq) of 18F-PSMA-1007 (n = 7, 25%), respectively (16). Images were acquired on a Biograph mCT (11/28, 39%) or Biograph Vision 600 (17/28, 61%) PET/CT system (Siemens Healthineers).
Image Interpretation
CT and PSMA PET/CT scans were analyzed separately 2 wk apart by 2 masked nuclear medicine physicians in joint consensus sessions and an additional board-certified radiologist for the CT reading session. The CT scans were read first, and for TNM-based analysis, pathologic findings were grouped into the following categories: local tumor, regional lymph nodes, nonregional lymph nodes, lung, bone, and other regions.
To assess the lesion-based disease extent, CT and PSMA PET/CT analysis results were each grouped into the following disease categories: no evidence of disease, unifocal disease (1 lesion), oligometastatic disease (2–5 lesions), multifocal disease (6–10 lesions), and disseminated disease (>10 lesions). For PSMA PET/CT analysis, the SUVmax of the lesion of each region with the highest uptake was measured. The PSMA expression score was assessed visually in accordance with PROMISE criteria on a per-patient level (17).
177Lu-PSMA-617 RLT
PSMA RLT was performed as therapy after exhaustion of established treatment options following the decision of a multidisciplinary tumor board. An overview of patient selection is provided in Figure 1. Key eligibility criteria were adequate bone marrow and kidney function in accordance with the procedure guidelines of the European Association of Nuclear Medicine and Society of Nuclear Medicine and Molecular Imaging for PSMA RLT (18) and a PSMA expression level of at least 2 (17). Each cycle, 6.8 ± 1.4 GBq of 177Lu-PSMA-617 were administered intravenously, with a 6-wk interval between cycles. Progression-free survival was defined as the interval from treatment start until death or progressive disease according to RECIST, version 1.1, as analyzed by 2 readers in joint consensus sessions (19).

CONSORT (Consolidated Standards of Reporting Trials) diagram describing SGM patient selection for PSMA-directed imaging and PSMA RLT.
Blood count, creatinine, transaminases, and symptoms were monitored before and during PSMA RLT, and toxicity was graded according to the Common Terminology Criteria for Adverse Events, version 5.0 (20).
Dosimetry
Posttherapeutic dosimetry of tumor lesions and kidneys was performed for all patients undergoing PSMA RLT and calculated according to OLINDA/MIRD recommendations (21). SPECT/CT imaging was performed on a Siemens Intevo SPECT/CT system using the xQuant reconstruction algorithm, allowing for quantitative 177Lu imaging as previously described (22). The chosen imaging schedule was set to include 4 time points (4, 24, 48, and 120–144 h) after injection, with at least 2 time points considered necessary to determine lesion or kidney doses. For logistic reasons, 2 or 3 time points were acquired for each cycle, respectively.
Statistical Analysis
The statistical analyses were performed using SPSS (version 27.0; IBM). The Student t test was used to assess differences in SUVmax dependent on sex, location of the primary, and disease site (bone vs. lung).
RESULTS
Patient Characteristics
The study included 28 patients (11 men, 39%; 17 women, 61%). Histopathologic subtypes were ACC (24/28, 86%), adenocarcinoma (2/28, 7%), acinic cell carcinoma (1/28, 4%), and sebaceous carcinoma (1/28, 4%). The median age was 59 y (range, 30–75 y). The clinical indication for PSMA PET/CT was initial staging for 2 patients (7%), restaging for 12 (43%), and evaluation for PSMA RLT for 14 (50%). Five patients (18%) underwent PSMA RLT. Detailed patient characteristics are provided in Table 1.
Patient Characteristics
Five of these patients (3 female, 2 male) received a total of 11 cycles of PSMA RLT (range, 1–6 cycles). The median age of PSMA RLT patients was 50 y (range, 40–65 y). Demographic and clinical information on the treatment cohort is provided in Table 2.
Characteristics of PSMA RLT Cohort
CT Versus PSMA PET/CT Detection Accuracy
CT detected any disease in 25 of 28 (89%) patients, local tumor in 7 (25%), regional lymph nodes in 1 (4%), and distant metastases in 22 (79%). PSMA PET was positive in 27 (96%) patients and visualized local tumor in 8 (29%), regional lymph nodes in 5 (18%), and distant metastases in 25 (89%) (Fig. 2). PSMA PET/CT demonstrated additional metastatic lesions in 11 (39%) patients; in 8 (29%) patients, CT-negative regions were rated positive on PSMA PET/CT. PSMA PET/CT detected additional bone metastases in 2 patients (7%) and nonregional lymph node metastases in 1 patient (4%), with no disease shown on CT (TNM upstaging). PSMA PET/CT led to an up-shift of lesion-based disease extent in 6 (21%) patients (Table 3). Figure 3 shows an example SGM patient, in whom additional bone lesions were detected by PSMA PET/CT.

Pie charts demonstrating additional detection of diseased regions by PSMA PET/CT (orange) when compared with standalone CT (blue). Charts demonstrate percentage positive patients among 28 patients, separately for each region.
Analysis of Lesion-Based Disease Extent

68Ga-PSMA PET/CT of 69-y-old man with adenoid-cystic carcinoma of right submandibular gland after primary resection. Maximum-intensity projection (A) and axial slices (B–E) of 68Ga-PSMA PET/CT reveal bone metastases in sixth left rib (white arrow) and sacral bone (black arrow) without CT correlate (F and G), confirmed by follow-up imaging 6 mo later.
In 6 (21%) patients 18F-FDG and PSMA PET/CT were performed within a 3-mo interval without interim progression on morphologic imaging. Of the 6 patients, 2 had higher detection efficacy for PSMA PET/CT, 2 had higher detection efficacy for 18F-FDG PET/CT, and 2 had equal detection efficacy for both modalities.
PSMA Ligand Uptake
PSMA expression score was 0 (n = 2, 7%), 1 (n = 4, 15%), 2 (n = 15, 56%), and 3 (n = 6, 22%), respectively (Fig. 4). The male sex (15.8 vs. 8.5, P = 0.007) was significantly associated with a higher SUVmax (Table 4). The mean SUVmax in tumor sites of patients with a primary tumor in the minor salivary glands was 12.8, versus 9.0 in those with a primary in the major salivary glands, without statistical significance (P = 0.31). SUVmax was significantly higher in bone than lung metastases (14.2 vs. 6.4, P = 0.006).

PSMA expression score by PROMISE criteria for 27 patients. One patient without any detected lesion was excluded.
Comparison of SUVmax for Sex, Primary Location at Initial Diagnosis, Bone Metastasis vs. Lung Metastasis, and Subtype
PSMA RLT Absorbed Dose and Efficacy
In total, 5 patients received PSMA RLT. Dosimetry was performed for the kidneys and a total of 13 tumor lesions over 7 therapy cycles. The highest lesion-absorbed dose was 0.68 Gy/GBq (mean, 0.41 Gy/GBq; range, 0.06–0.68 Gy/GBq). The highest lesion uptake ratio after 24 h was 0.44 (mean, 0.16; range, 0.004–0.44). The mean effective half-life of the lesions was 7.7 min (range, 0.32–30.98 min). The mean kidney-absorbed dose was 0.37 Gy/GBq (range, 0.32–0.41 Gy/GBq). Dosimetry results for each cycle are shown in Table 5.
Results of Individual Patient Dosimetry
PSMA RLT was discontinued in 3 patients after 1 cycle because visual lesion uptake was below liver uptake on the 24-h posttreatment 177Lu-PSMA scintigraphy. In these 3 patients, systemic treatment was initiated before progression occurred. Progression-free survival was 3 mo (n = 1) or not reached (n = 1, last follow-up: 12 mo) after initiation of PSMA RLT in the 2 patients remaining with more than 1 treatment cycle. The long-term response was observed in the only patient with acinic cell carcinoma, with the remainder having ACC. Supplemental Figure 1 shows a patient example (supplemental materials are available at http://jnm.snmjournals.org).
PSMA RLT Adverse Events and Follow-up
Changes in blood parameters did not meet the adverse-event criteria of the Common Terminology Criteria for Adverse Events, version 5.0. Xerostomia that was less than serious was reported by both patients undergoing more than 1 cycle of PSMA RLT, without worsening under treatment.
DISCUSSION
The results of our study indicate a superior detection rate for PSMA PET/CT in SGMs, with additional localization of lesions in 11 of 28 patients (39%) and TNM upstaging in 3 (11%) patients through the detection of CT-occult oligometastatic bone metastases. Therefore, in salivary gland tumors PSMA PET/CT may be a possible alternative to other hybrid imaging modalities such as 18F-FDG PET/CT or PET/MRI (11,23). In addition, PSMA PET/CT identifies candidates for PSMA RLT, which was well tolerated and induced a tumor response.
PSMA PET/CT revealed oligometastatic disease in 9 of 28 (32%) patients (Table 3). Accurate localization of disease supports planning of metastasis-directed therapy. Metastasis-directed therapy of oligometastatic head and neck cancer, including SGMs, has been shown to result in high disease-control rates (24), which underline the importance of sensitive imaging to further optimize this treatment option. PSMA PET/CT revealed multifocal or disseminated disease in 3 of 9 (33%) patients with CT oligometastatic disease. Detection of multifocal or disseminated disease may thereby more accurately identify patient candidates for systemic therapy not likely to benefit from local treatment alone.
Seventy-five percent of patients had at least 1 lesion with PSMA uptake equal to or higher than liver uptake, with significantly higher PSMA expression occurring in male patients and bone lesions (Table 4). Boxtel et al. likewise demonstrated high tumor uptake (13). Higher PSMA expression in male patients is not supported by current knowledge of PSMA regulation pathways, since high androgen levels suppress the PSMA encoding gene folate hydrolase 1, potentially reducing PSMA expression levels (25). This finding has been demonstrated in prostate cancer patients, in whom prolonged androgen-deprivation therapy was linked to increases in PSMA expression (26). Likewise, the androgen axis can be active in patients with SGMs, and the efficacy and safety of androgen receptor–targeted treatment is currently being investigated in a prospective single-arm clinical trial (NCT04325828). In line with this possibility, an immunohistochemistry study by Boxtel et al. showed higher PSMA expression in tumor cells of SGMs in women than in men, attributed to lower levels of circulating androgens (27). In contrast to immunohistochemistry findings, PSMA PET/CT allows for the in vivo noninvasive assessment of target PSMA expression in entire lesions and at multiple tumor sites. PSMA PET/CT indicates that male patients may be more suitable candidates for PSMA RLT. However, because the small sample size is conducive to the occurrence of type 1 errors, further analyses of larger cohorts are warranted.
In our case series, PSMA RLT was well tolerated. Events grade 3 or higher in the Common Terminology Criteria for Adverse Events were not noted. There was no treatment-limiting xerostomia. In line with this finding, side effects of PSMA RLT were grade 1–2 in a study by Klein Nulent et al., and only 1 patient experienced grade 3 thrombocytopenia (28). However, tumor-absorbed doses in our patients were unsatisfactory. Although high PSMA expression was noted on both PSMA PET/CT and early posttreatment SPECT/CT, retention times of PSMA uptake were short, resulting in lower absorbed doses than in prostate cancer. A potential explanation is the low detection threshold of PSMA PET/CT, resulting in a high target-to-background signal that may lead to an overestimation of PSMA expression (29).
To our knowledge, this was the largest study so far to evaluate the dosimetry of PSMA RLT in SGMs. Uijen et al. reviewed a total of 15 cycles of PSMA RLT in 10 non–prostate cancer patients, also including 2 patients with SGMs (30). Klein Nulent et al. demonstrated the first case of ACC treated with PSMA RLT, but treatment response or dosimetry data were not reported (14). Has Simsek et al. reported 1 ACC patient treated with PSMA RLT, revealing intense metastatic PSMA uptake on posttreatment imaging performed after 24 h (15). Klein Nulent et al. reported the first cohort study to evaluate the efficacy and safety of PSMA RLT in SGMs (28). Six patients with SGMs were treated with PSMA RLT, which resulted radiologically stable disease in 2 patients after 4 cycles and a clinical response such as pain relief, less dyspnea, and less fatigue in 4 patients after 2 or 4 cycles of PSMA RLT (28).
In our study, tumor stabilization over more than 1 y was observed for only 1 of 5 PSMA RLT patients, indicating that further improvement is needed. In the future, RLT may be improved by more stringent patient selection, application of higher-activity regimens, or introduction of α-based RLT. Further research focusing on histopathologic subtypes, specifically on PSMA RLT in acinic cell carcinoma, may be of interest.
Limitations of this study include its retrospective, single-center design and small sample size.
CONCLUSION
PSMA PET/CT demonstrated superior tumor detection and led to upstaging in about one third of SGM patients when compared with CT. The male sex and the presence of bone metastases were associated with significantly higher PSMA expression. PSMA RLT was tolerated well and stabilized disease in 1 patient. However, frequent discontinuation after 1 PSMA RLT cycle and low tumor-absorbed doses indicate that PSMA RLT for SGM needs further improvement.
DISCLOSURE
Wolfgang Fendler received financial support from the German Research Foundation (Deutsche Forschungsgemeinschaft grant FE1573/3-1/659216) and Wiedenfeld-Stiftung/Stiftung Krebsforschung Duisburg. Manuel Weber reports fees from Boston Scientific, Terumo, Eli Lilly, and Advanced Accelerator Applications, outside the submitted work. Christoph Berliner reports personal fees from Janssen (speakers’ bureau), ABX (image review), and Roche (image review) outside the submitted work. Ken Herrmann reports personal fees from Bayer, Sofie Biosciences, SIRTEX, Adacap, Curium, Endocyte, BTG, IPSEN, Siemens Healthineers, GE Healthcare, Amgen, Novartis, ymabs, Aktis Oncology, Theragnostics, and Pharma15; other fees from Sofie Biosciences; nonfinancial support from ABX; and grants from BTG, outside the submitted work. David Kersting is supported by the Universitätsmedizin Essen Clinician Scientist Academy/German Research Foundation and reports research funding from Pfizer outside the submitted work. Benedikt Schaarschmidt is supported by a research grant from PharmaCept, outside the submitted work. Wolfgang Fendler reports fees from Sofie Biosciences (research funding), Janssen (consultant, speakers’ bureau), Calyx (consultant), Bayer (consultant, speakers’ bureau), and Parexel (image review) outside the submitted work. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is PSMA a potential target for theranostic applications in SGMs?
PERTINENT FINDINGS: In SGMs, PSMA PET/CT has a higher detection rate than conventional imaging and led to upstaging in about one third of patients. 177Lu-PSMA-617 treatment was tolerable and resulted in disease stabilization in 1 patient with acinic cell carcinoma.
IMPLICATIONS FOR PATIENT CARE: Preliminary findings demonstrate a superior detection rate for PSMA PET/CT compared with CT in SGMs and a potential role for PSMA RLT in a subset of patients. Prospective studies on larger collectives are warranted.
Footnotes
Published online Sep. 22, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 27, 2022.
- Revision received September 16, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.