


Visual Abstract

Abstract
When pregnancy is discovered during or after a diagnostic examination, the physician or the patient may request an estimate of the radiation dose received by the fetus as per guidelines and standard operating procedures. This study provided the imaging community with dose estimates to the fetus from PET/CT with protocols that are adapted to University of Michigan low-dose protocols for patients known to be pregnant. Methods: There were 9 patients analyzed with data for the first, second, and third trimesters, the availability of which is quite rare. These images were used to calculate the size-specific dose estimate (SSDE) from the CT scan portion and the SUV and 18F-FDG uptake dose from the PET scan portion using the MIRD formulation. The fetal dose estimates were tested for correlation with each of the following independent measures: gestational age, fetal volume, average water-equivalent diameter of the patient along the length of the fetus, SSDE, SUV, and percentage of dose from 18F-FDG. Stepwise multiple linear regression analysis was performed to assess the partial correlation of each variable. To our knowledge, this was the first study to determine fetal doses from CT and PET images. Results: Fetal self-doses from 18F for the first, second, and third trimesters were 2.18 mGy (single data point), 0.74–1.82 mGy, and 0.017–0.0017 mGy, respectively. The combined SSDE and fetal self-dose ranged from 1.2 to 8.2 mGy. These types of images from pregnant patients are rare. Conclusion: Our data indicate that the fetal radiation exposure from 18F-FDG PET and CT performed, when medically necessary, on pregnant women with cancer is low. All efforts should be made to minimize fetal radiation exposure by modifying the protocol.
Diagnostic imaging that uses ionizing radiation may sometimes be necessary for a pregnant patient despite the potential risk to the fetus. Typically, when such diagnostic information is needed, it is relating to the health of the mother. When radiologists or nuclear medicine physicians need to decide if the diagnostic benefits will outweigh the risks of radiation, it is important they have a reasonable estimate of radiation dose to the fetus. When pregnancy is discovered during or after a diagnostic examination, the physician or the patient may request an estimate of the radiation dose received by the fetus. The risks of fetal adverse outcomes, including childhood cancer induction, are small at a dose of 100 mGy and negligible at doses of less than 50 mGy (1,2). In the case of hybrid imaging in which both modalities involve radiation, the fetal dosimetry resulting from both modalities should be considered. One example is PET/CT, where the CT scan provides anatomic information and the PET scan provides information on radionuclide uptake at the tumor site. Fetal dose estimates from CT have been based primarily on Monte Carlo simulations of geometric patient models (3–5). PET studies of pregnant patients are extremely uncommon, and even 18F-FDG PET studies accidentally performed on pregnant patients are rare (6–11). Therefore, providing fetal dose estimates from the CT and 18F-FDG PET images themselves and from dose reports would be helpful to the medical imaging community. In this study, fetal dose estimates for PET/CT scans were based on a series of pregnant patients in their first, second, and third trimesters. These images were used to calculate the size-specific dose estimate (SSDE) (12) from the CT scan portion and to calculate the SUV and 18F-FDG uptake dose from the PET scan portion using the MIRD formulation. This study provided the imaging community with dose estimates to the fetus from PET/CT based on patient data, the availability of which is quite rare.
MATERIALS AND METHODS
Pregnant Patient Population
In total, 9 18F-FDG PET/CT scans performed on pregnant patients over an 11-y period at the University of Michigan were analyzed. The axial range of these scans covered the full uterus. The gestational ages of the fetuses of these patients ranged from 3 to 40 wk. The cohort included 2 patients in the first trimester of pregnancy, 2 in the second trimester, and 5 in the third trimester. Some patients were scanned multiple times during pregnancy and the postpartum period to ascertain diagnostic information pertaining to the patient. The postpartum scans were included in this study as a way of comparing what dose a fetus might get from a PET/CT scan using standard protocols for nonpregnant patients.
CT Fetal Dose Estimation
The CT portion of the scans was acquired with 120-kVp and 130-kVp acquisition protocols, with the slice thickness varying from 2 to 5 mm. The patients were originally scanned with one of the following scanners: Siemens Biograph Vision 6 PET/CT, Siemens Biograph 40 True Point PET/CT, and Siemens Emotion Duo CT/CPS 1062 PET. No oral contrast agent was used for the CT examinations. The PET/CT images of the pregnant mothers’ anatomy were at least from the top of the cranium to the upper thigh of the mother. The gestational age was estimated from the clinical data.
CT axial scans of the same 9 patients were collected on Siemens systems. These images were analyzed retrospectively, and the scan parameters were obtained from the Digital Imaging and Communications in Medicine (DICOM) header shown in Table 1. There are 2 patients who were scanned twice with the fetus at different gestational ages.
Patient Data
These CT scans were performed using techniques yielding low doses as shown in Table 1. For all 9 patients, there was no automatic tube current modulation; therefore, a constant tube current and kilovoltage were used. For patients 1–5, scanned before 2011, the CT dose index–volume (CTDIvol) was not reported since this quantity was not a Food and Drug Administration requirement at the time. The CTDIvol was calculated using the output values for a 32-cm phantom of 6.7 mGy/100 mAs in the center and 12.8 mGy/100 mAs at the periphery for the Emotion Duo (13) and Biograph 6 (14) scanners. The pitch factor could not be located in the DICOM header for scans from these scanners, so we assumed it to be 1.0.
The CT dose to the fetus was based on the SSDE method used to calculate organ dose (8,15–23). A recent study by Hardy et al. (24) showed a reasonable accuracy (±25%) with SSDE as a surrogate of fetal dose. The normalized dose coefficient (NDC) scales the CTDIvol to make it reflect the dose the patient actually receives. The NDC is calculated directly from the patient size surrogates, which include the effective diameter or water-equivalent diameter (DW). The preferred patient size surrogate is the DW since it directly incorporates attenuation properties from the patient scan. DW represents the diameter of a cylinder of water that contains the same total x-ray attenuation as that contained within the patient’s axial cross section and depends on both the cross-sectional area of the patient and the attenuation of the contained tissues. The method of calculating DW described in American Association of Physicists in Medicine report 220 (12) was implemented using the following equation: Eq. 1where CT represents the mean CT number within the reconstructed field of view and AROI is the product of the number of pixels in the region of interest (ROI) and the pixel area. Our ROI was inscribed inside the reconstructed DICOM images for each patient. Since the DICOM images are square matrices, we inscribed a circle inside each DICOM image with a diameter equal to the entire width of the image. DW was calculated from CT axial images as previously described. Corrections were applied to images that were not reconstructed at isocenter (25). In some cases, when the reconstructed image center was not at isocenter, this ROI could contain padding values of −3,024 Hounsfield units. Therefore, we applied a remapping of all the values inside the circle used to calculate the mean CT number, which mapped all signals equal to −3,024 to −1,000 Hounsfield units to simulate air. The use of padding values is common to most CT vendors, but the padding value may differ. Failure to correct for this would decrease the DW values. We did not perform any thresholding or connected-component analysis of the axial image data before calculating DW. The DW uses the mean Hounsfield units of the patient habitus, taking into consideration the attenuation properties of the patient. The DW was then used to calculate the NDC using equation A-1 from the American Association of Physicists in Medicine task group report 204, replicated in equation 2 here:
Eq. 1where CT represents the mean CT number within the reconstructed field of view and AROI is the product of the number of pixels in the region of interest (ROI) and the pixel area. Our ROI was inscribed inside the reconstructed DICOM images for each patient. Since the DICOM images are square matrices, we inscribed a circle inside each DICOM image with a diameter equal to the entire width of the image. DW was calculated from CT axial images as previously described. Corrections were applied to images that were not reconstructed at isocenter (25). In some cases, when the reconstructed image center was not at isocenter, this ROI could contain padding values of −3,024 Hounsfield units. Therefore, we applied a remapping of all the values inside the circle used to calculate the mean CT number, which mapped all signals equal to −3,024 to −1,000 Hounsfield units to simulate air. The use of padding values is common to most CT vendors, but the padding value may differ. Failure to correct for this would decrease the DW values. We did not perform any thresholding or connected-component analysis of the axial image data before calculating DW. The DW uses the mean Hounsfield units of the patient habitus, taking into consideration the attenuation properties of the patient. The DW was then used to calculate the NDC using equation A-1 from the American Association of Physicists in Medicine task group report 204, replicated in equation 2 here: Eq. 2
Eq. 2
where constant a = 3.70469 and constant b = 0.03671937. The SSDE is simply the product of the NDC and CTDIvol as shown in equation 3: Eq. 3where the CTDIvol for a 32-cm phantom was taken from the patients’ dose reports. The average SSDE was taken along the length of the fetus. The absorbed dose to the uterus was used as a surrogate for the absorbed dose to the embryo/fetus as is common practice in medical radiation dosimetry (22,23). The CT localizer radiograph (or topogram) technique (kVp and mA) is reported in Table 1. The dose range for the topograms was 0.08–0.13 mGy.
Eq. 3where the CTDIvol for a 32-cm phantom was taken from the patients’ dose reports. The average SSDE was taken along the length of the fetus. The absorbed dose to the uterus was used as a surrogate for the absorbed dose to the embryo/fetus as is common practice in medical radiation dosimetry (22,23). The CT localizer radiograph (or topogram) technique (kVp and mA) is reported in Table 1. The dose range for the topograms was 0.08–0.13 mGy.
18F-FDG Fetal Dose Estimation
The 18F-FDG dose administered for all 9 patients in this study was 130 MBq (3.5 mCi). At the time of the injection, the physicians knew that the patients were pregnant, which is the reason for such a low injection dose. All pharmacokinetic and dosimetric estimates for 18F-FDG, including placental crossover, are shown in Table 2 (26).
18F-FDG Uptake MIRD Calculation Using RADAR with Interpolation Between 12, 24, and 36 Weeks
For 18F-FDG dose calculations, the fetuses in the first, second, and third trimesters were rounded to gestational ages of 3, 6, and 9 mo. The 18F-FDG fetal self-dose and total dose from both maternal organs and the fetal self-dose were calculated using a table of specific absorption fractions (27) for the following organs: adrenals, brain, breasts, gallbladder wall, lower large intestine wall, small intestine, stomach, upper large intestine wall, heart wall, kidneys, liver, lungs, muscle, ovaries, pancreas, red marrow, bone surfaces, skin, spleen, thymus, thyroid, urinary bladder wall, uterus, fetus, and placenta.
The SUV is a simple metric for assessing the amount of activity present in the fetus. The SUV was determined using Hermes software by drawing a contour ROI about the fetus in all slices of the PET image where the fetus was present. The mean, maximum, and peak (95% percentile) values were determined over the entire volume of the fetus.
Statistical Analysis
The fetal dose estimates were tested for correlation with each of the following independent measures: gestational age, fetal volume, average DW of the patient along the length of the fetus, SSDE, SUV, and percentage of dose from 18F-FDG. Stepwise multiple linear regression analysis was performed to assess the partial correlation of each variable.
RESULTS
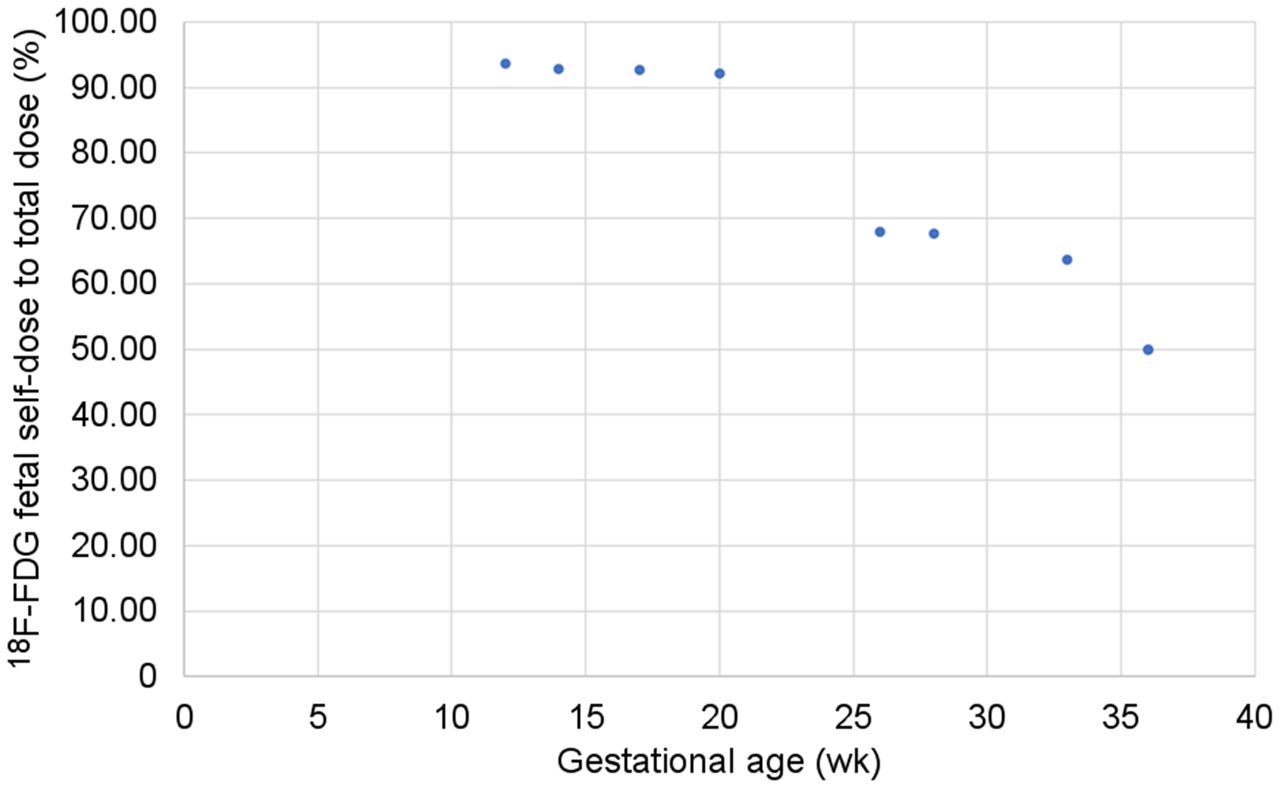
All data were collected under an institutional review board–approved protocol in a retrospective manner in which the need for patient consent was waived. Table 3 shows the following information gathered from the PET scan: SUVmean, SD, SUVmax, and 95th percentile SUV, all over the entire volume of the fetus. Table 2 shows the SSDE for 4 cases after 2011, the 18F fetal self-dose, 18F fetal total dose, total dose from SSDE and 18F to fetus, and percentage of fetal self-dose to total dose. Figure 1 shows the 18F-FDG fetal self-dose to fetal total dose from organs, including the fetus, of the patient.
SUVmean, SUVmax, and 95th Percentile SUV over Entire Fetal Volume
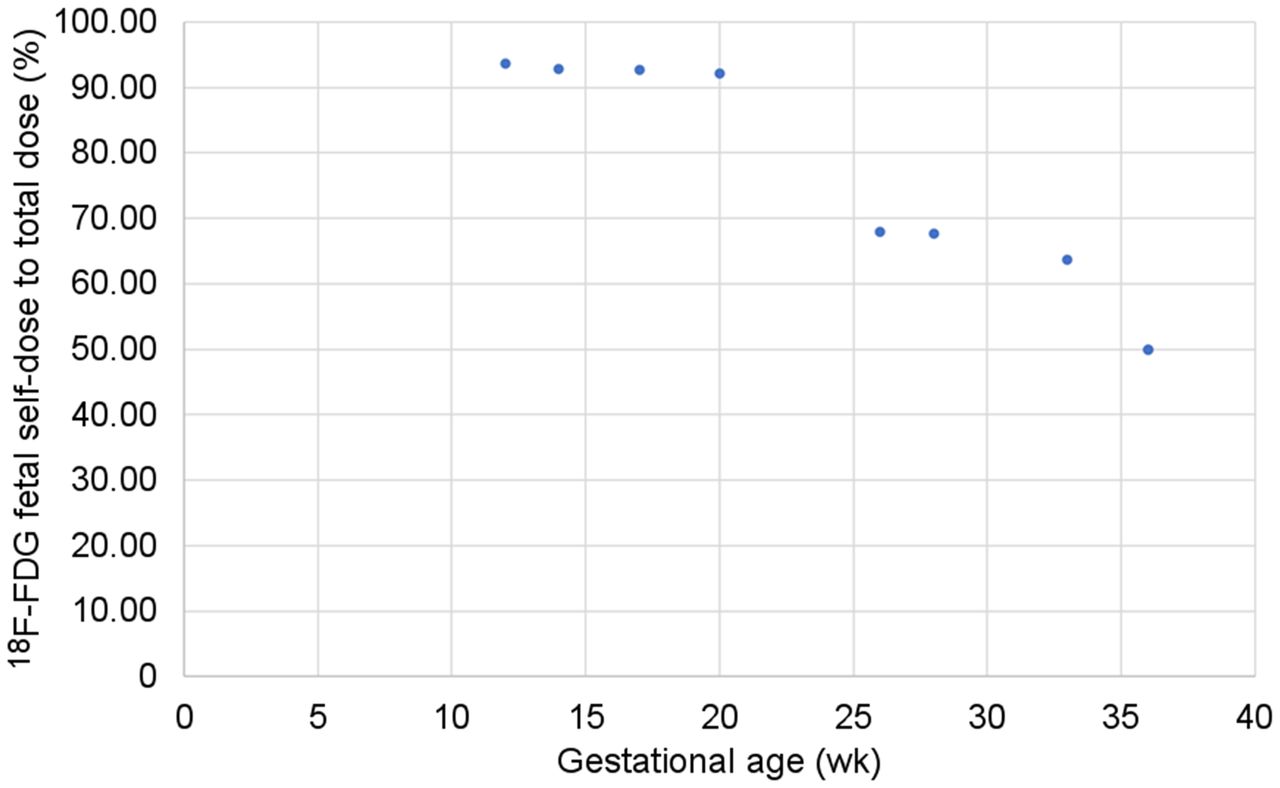
18F-FDG fetal self-dose to fetal total dose from organs of patient.
DISCUSSION
To our knowledge, this was the largest series of pregnant patients for whom fetal radiation dose from 18F-FDG and SSDE was calculated. Our data add considerably to the existing literature about fetal radiation exposure from 18F-FDG PET and CT dose studies of pregnant patients. These patients were not accidentally exposed to 18F-FDG during their pregnancy but rather underwent intentional studies that were performed after adequate consideration of the risks and benefits of 18F-FDG PET in these pregnant patients with malignancy. 18F-FDG is known to cross the placental membrane and accumulate in the fetus (8,22,28–30), and we were able to clearly identify 18F-FDG activity in the fetus inside the gravid uterus, confirming the ability of 18F-FDG to cross the placenta and accumulate in the fetus. There is no scientific literature documenting fetal toxicity associated with 18F-FDG in pregnant women or nonhuman primates. All our patients delivered healthy babies at term.
For visual inspection, Figure 2 shows examples of a single CT and corresponding PET image of the fetus for pregnant patients in the first, second, and third trimesters.

Examples of single PET (left), CT (middle), and PET/CT (right) images for 6 patients in cohort with high concentration of 18F-FDG in fetal heart at gestational ages (from top to bottom) of 12 wk, 20 wk (second and third from top), and 36 wk (bottom three) to demonstrate first trimester, second trimester, and third trimester pregnancies, respectively. 18F-FDG uptake in fetus is seen in PET images.
Our results show that fetal doses from a combined dose from 18F-FDG and SSDE range from 1.2 to 8.2 mGy and that the SSDE alone ranges from 1.0 to 2.0 mGy, as shown in Table 2. These doses are significantly below the threshold of 50–100 mGy considered for deterministic effects to the fetus, although fetal dose in this range does not conclusively result in an adverse impact on the fetus (31). Generally, most of the diagnostic studies performed during a mother’s pregnancy are below this threshold. However, there is no threshold for stochastic effects, but a discussion about the probability of various deterministic and stochastic effects occurring because of fetal exposure to radiation from CT or 18F-FDG PET in pregnancy is beyond the scope of this article.
It is not uncommon for a pregnant mother to be imaged using CT by itself. According to a large, multicenter study of advanced medical imaging in pregnancy. The CT imaging rates in the United States increased from 2.0 examinations per 1,000 pregnancies in 1996 to 11.4 per 1,000 pregnancies in 2007, remained stable through 2010, and decreased to 9.3 per 1,000 pregnancies by 2016 (32). Fetal dose estimates from CT have been based primarily on Monte Carlo simulations of geometric patient models. One method is the CTExpo software (version 1.5.1; Medizinische Hochschule) (32), in which organ dose estimates are based on simulations performed by Zankl et al. at the German National Research Center, with the Eva geometric phantom model representing a standard-sized female patient (3,4). Felmlee et al. demonstrated estimates of CT dose index using Monte Carlo simulations on an anthropomorphic phantom (5). Using Monte Carlo simulations, Ratnapalan et al. (33) and Lazarus et al. (34) reported that normalized fetal CT dose ranges from 7.3 to 14.3 mGy/100 mAs and that mean dose is 17.1 mGy (range, 8–44 mGy), respectively. Goldberg-Stein et al. looked at a series of 54 patients and estimated mean fetal dose to be 24.8 mGy (range, 6.7–56 mGy) (35). Doses to the fetus from a single-acquisition abdominal–pelvic CT examination have ranged between 10 and 50 mGy in phantom and clinical studies. Hurwitz et al. (36) estimated fetal dose as 1.52–3.22 cGy using physical measurements from internal dosimeters in an anthropomorphic phantom that was modified to represent a newly pregnant patient and a patient who was 3 mo pregnant. Since the patients in our study were known to be pregnant before the scan, the scanner technique may have been set to give the lowest possible CTDIvol, which was indicative of the automatic exposure control’s being turned off. Although CTDIvol is often provided, the uniform cylindric phantom does not represent the gross anatomy of a pregnant patient. SSDE, a quantity that describes the absorbed dose to the patient, scales the CTDIvol with a factor based on the patient’s size and attenuation (12,37). This metric will be required to be reported by vendors soon, though it will likely be an average SSDE over the entire patient range. Hardy et al. (24) calculated the CTDIvol–to–fetal-dose coefficients for tube current–modulated and fixed tube current CT examinations of pregnant patients of various gestational ages and reported the SSDE. To estimate SSDE to an organ, Moore et al. (23) provided a method that utilized the conversion factor for the uterus. Existing methods to estimate fetal dose for pregnant patients undergoing CT examinations assume early term pregnancy in a single-sized patient model with an average, nonvarying maternal anatomy. These dose estimates do not consider natural variations such as fetal presentation and gestational age. Differences in these attributes can cause overestimation or underestimation of up to 100% (38). Angel et al. (39) used Monte Carlo simulations to estimate fetal dose in CT for a range of gestational ages and patient sizes and found no significant correlation between gestational age and fetal dose. For various fetal ages and maternal body habitus, the fetal dose estimates were between 1.1 and 21.9 mGy for CT.
18F-FDG PET studies of pregnant patients are extremely uncommon, and even 18F-FDG PET studies accidentally performed on pregnant patients are rare (6–11). Because adequate and accurate data regarding 18F-FDG uptake by the fetus are not available other than the very few case reports of accidental exposure, it is difficult to get an estimate of fetal radiation exposure from 18F-FDG PET in pregnant patients. As a result, most estimates of fetal dose from 18F-FDG PET are based on models of exposure of the fetus to radiation from the mother and do not consider self-dose from the fetus itself. Those studies that have been published are based mostly on data from nonhuman primates and mathematic models (8–11). Recent case reports by Zanotti-Fregonara et al. (28,40) have raised the possibility that 18F-FDG dose to the fetus in early pregnancy may be higher than estimated by current dosimetric standards. Hence, there is a need to have more data to establish the accurate fetal dose exposure. A few studies have looked at fetal dose from mothers having a PET scan using 18F-FDG (41–44). The Society of Nuclear Medicine and Molecular Imaging has provided a nuclear medicine radiation dose tool for 18F-FDG examinations for different patient models, including pregnant women in the early stage of pregnancy and at 3, 6, and 9 mo into pregnancy. This model provides 2 dosimetry tables (45,46) to perform these calculations, and the user inputs the initial activity. The first is from International Commission on Radiological Protection (ICRP) publication 128 (2015), which bases its dosimetry model on anthropomorphic phantoms and bases its effective doses on organ-weighting factors from ICRP publication 60. The tables contain a mix of published estimates from ICRP (publications 53, 80, and 106) and dosimetry provided by Stabin et al. (26). The second is dose estimates from the Radiation Dose Assessment Resource (RADAR) (2017) generated using a set of anthropomorphic phantoms (26) based on the recommended body and organ masses given in ICRP publication 89 (2003). This study uses PET scans of pregnant patients to calculate the SUV, fetal self-dose, and total fetal dose from the organs of the patient, and from our findings, we determined that 18F-FDG dose is exceedingly low. The fetal heart contains the highest concentration of 18F-FDG uptake, as shown in Figures 3–7, which show examples of 18F-FDG in the fetal heart for patients in their second and third trimesters. Supplemental Figure 1 shows a patient who is well into her third trimester with 18F-FDG in the fetal heart, like that shown in Figure 7 (supplemental materials are available at http://jnm.snmjournals.org). Figure 2A shows a higher concentration of 18F-FDG uptake in the fetal heart.

Example of concentrated uptake of 18F-FDG in fetal heart (arrows) for patient in second trimester at 20 wkT.

Example of concentrated uptake of 18F-FDG in fetal heart (arrows) for patient in second trimester at 26 wk.

Example of concentrated uptake of 18F-FDG in fetal heart (arrows) for patient in second trimester at 28 wk (entering third trimester).

Example of concentrated uptake of 18F-FDG in fetal heart (arrows) for patients well into third trimester at 33 wk.

Example of concentrated uptake of 18F-FDG in fetal heart (arrows) for patients well into third trimester at 36 wk.
For PET/CT, the total estimated radiation dose to the fetus is the sum of CT exposure, maternal γ-irradiation, and fetal β- and γ-irradiation. One method for calculating fetal dose estimates for CT is the ImPACT CTDosimetry dose calculator (CTDosimetry.xls, version 0.99; ImPACT) (47), which is based on Monte Carlo simulations performed by the National Radiological Protection Board (48) with a geometric MIRD phantom model (49).
A limitation to our study is that, although we believe our sample of pregnant patients to be the largest ever reported, it is still relatively small. Another limitation is that we considered the fetus to be an oval shape in PET images for calculating SUV. It was difficult to contour the perimeter of the fetus, especially for the first trimester; however. this oval was confined as much as possible to the fetus for each PET slice. We also rounded the gestational age upward to 3, 6, and 9 mo for the MIRD calculations. Lastly, we did not attempt to estimate the dose uncertainties for this study.
CONCLUSION
To our knowledge, this was the first study to determine fetal doses from CT and PET images of pregnant patients. These types of images from pregnant patients are rare. Fetal self-dose from 18F for the first, second, and third trimesters was 2.18, 0.74–1.82, and 0.017–0.0017 mGy, respectively. The range of SSDE for the CT scan and fetal self-dose for the PET scan was 1.2–8.2 mGy. Our data indicate that fetal radiation exposure from 18F-FDG PET and CT performed, when medically necessary, on pregnant women with cancer is low. All efforts should be made to minimize fetal radiation exposure while maintaining diagnostic accuracy by modifying the protocol.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is there a risk to the fetus for pregnant patients undergoing a PET/CT scan?
PERTINENT FINDINGS: In a study involving 9 pregnant patients who underwent PET/CT, our data suggest that the fetal radiation exposure from 18F-FDG PET and CT performed, when medically necessary, on pregnant women with cancer is low. The fetal self-dose from 18F-FDG for the first, second, and third trimesters was 2.18, 0.74–1.82, and 0.017–0.0017 mGy, respectively, and the range of SSDE and fetal self-dose was 1.2–8.2 mGy.
IMPLICATIONS FOR PATIENT CARE: Although use of PET/CT on pregnant patients is not encouraged, the data suggest that if a scan is needed to assess the health of the patient, the dose to the fetus would not put the fetus at risk. All efforts should be made to minimize fetal radiation exposure by modifying the protocol.
Footnotes
Published online Sep. 8, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 2, 2022.
- Revision received August 23, 2022.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.