


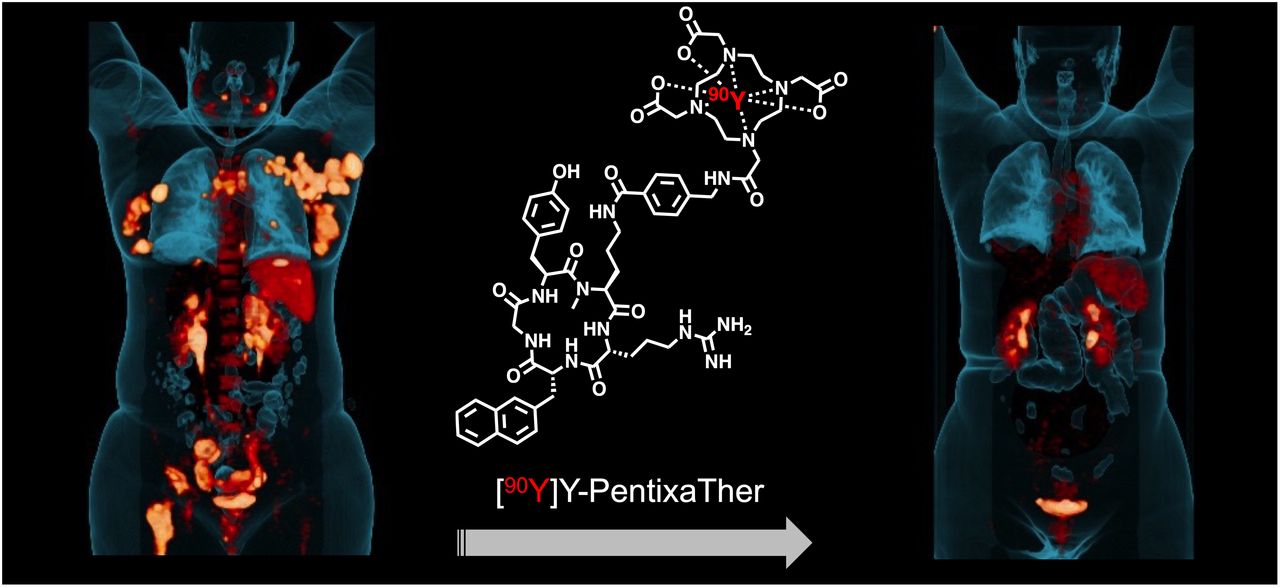
Visual Abstract

Abstract
C-X-C motif chemokine receptor 4 (CXCR4)–targeted radioligand therapy (RLT) has already been applied to advanced blood cancers, such as multiple myeloma or diffuse large B-cell lymphoma. We present a series of patients with advanced T-cell lymphoma (TCL) who were scheduled for CXCR4-directed therapy as a conditioning regimen, followed by hematopoietic stem cell transplantation (HSCT). Methods: Four patients with advanced, heavily pretreated, and relapsed TCL (2 men, 2 women; median age, 50 y) without suitable alternative therapeutic options underwent CXCR4-directed PET and pretherapeutic dosimetry. We then conducted CXCR4-targeted RLT in combination with allogeneic (3/4, 75%) or autologous (1/4, 25%) HSCT. One patient also underwent radioimmunotherapy targeting CD66 to enhance therapeutic efficacy. We investigated safety, best response, progression-free survival, and overall survival. Results: Pretherapeutic dosimetry indicated lymphoma-absorbed doses of up to 33.2 Gy from CXCR4-targeted RLT. Except for 1 patient who developed tumor lysis syndrome along with transient grade 3 kidney failure, no acute toxicity, allergic reactions, or other adverse events were recorded during therapy. One patient developed septicemia and subsequently died 16 d after RLT, whereas engraftment was achieved in the remaining 3 patients (75%). During follow-up, a partial response was recorded in 1 of 3 patients (33.3%) and a complete metabolic response in the other two (66.7%, with 1 patient also receiving additional radioimmunotherapy). Median progression-free survival was 7 mo (range, 4–25 mo). After a median follow-up of 54 mo (range, 4–56 mo), 3 patients were still alive at the date of censoring. Conclusion: For advanced, heavily pretreated TCL, CXCR4-directed RLT may serve as an effective conditioning therapy before HSCT and can cause substantial antilymphoma activity, leading to a remarkable response in selected cases.
- C-X-C motif chemokine receptor 4
- CXCR4
- chemokine receptor
- theranostics
- radioligand therapy
- T-cell lymphoma
As an orphan disease, peripheral T-cell lymphoma (TCL) accounts for up to 10% of all cases of non-Hodgkin lymphoma (1). The current World Health Organization classification of lymphoid neoplasms lists 29 different subtypes (2), and the 5-y survival rate is estimated to be 25.4%–80.2% (3,4). First-line treatment consists of cyclophosphamide, doxorubicin, vincristine, etoposide, and prednisolone (5–7), whereas more effective regimens such as brentuximab vedotin, cyclophosphamide, doxorubicin, and prednisone can be administered primarily to patients exhibiting CD30-positive peripheral TCLs (8). In advanced, relapsed, or refractory stages, however, therapeutic options are limited and include myeloablative conditioning high-dose chemotherapeutic regimens, followed by hematopoietic stem cell transplantation (HSCT) (4).
Recent ex vivo analyses reported a substantial overexpression of the C-X-C motif chemokine receptor 4 (CXCR4) on specimens from lymphoma patients (9), including peripheral TCL (10). Thus, the CXCR4-targeting PET agent 68Ga-pentixafor has been administered to patients with various subtypes of lymphomas (11,12). Such initial reports showed an intense radiotracer accumulation in disease manifestations, in particular for TCL (11,12), thereby allowing identification of patients who can be treated with the therapeutic CXCR4-targeting radiotracer 90Y/177Lu-pentixather. The feasibility of treatment with these β-emitting agents has already been demonstrated, such as in patients with multiple myeloma, acute leukemia, or diffuse large B-cell lymphoma (13–16). In the present report, we describe our initial experience with CXCR4-directed radioligand therapy (RLT) as a conditioning therapy for patients with advanced TCL before HSCT in a theranostic setting. We also report on the antilymphoma activity of radiolabeled CXCR4-targeted treatment.
MATERIALS AND METHODS
We offered experimental CXCR4-targeted RLT as a conditioning regimen and to achieve antilymphoma activity based on the German Pharmaceutical Act (§13.2b). Patients gave written informed consent to all diagnostic and therapeutic procedures. The local ethical committee of the University Würzburg waived the need for approval because this was a retrospective investigation (waiver no. 20220103 01). The patients were partly investigated in a previous study (17), without assessment of the clinical course or the achieved doses to tumor or normal organs. Table 1 provides an overview of the investigated patients.
Patient Characteristics
CXCR4-Directed 68Ga-Pentixafor PET
To assess the retention capacities in vivo, we conducted pretherapeutic CXCR4-directed PET/CT using 68Ga-pentixafor, which was prepared in-house as described previously (12). CXCR4 expression was visualized 60 min after intravenous administration of 68Ga-pentixafor (median injected activity, 136.5 MBq; range, 85–157 MBq) using a Biograph mCT 64 or 128 PET/CT system. Expert readers confirmed CXCR4 expression in sites of disease (12).
CXCR4-Directed Dosimetry and RLT
Before RLT, all patients underwent dosimetry using 177Lu-pentixather (18), thereby allowing us to provide the exact amount of administrable activity to minimize off-target effects and to calculate the tumor dose at sites of disease. For therapy, we administered 4.8 GBq of 90Y-pentixather (range, 4.2–5.1 GBq; Table 2). Radiotracer synthesis was described previously (14). Relative to 177Lu (half-life, 160.8 h), the physical half-life of 90Y is only 64 h and thus allows substantial shortening of the time until HSCT (16). The administrable activity of 90Y-pentixather was based on the individual kinetics derived from pretherapeutic dosimetry (with the assumption of a maximum tolerable dose to the kidneys of 23 Gy) (16). We then performed RLT a median of 8 d after pretherapeutic dosimetry (range, 3–14 d). As described previously (16), we also administered a nephroprotective solution consisting of 25 g/L solutions of arginine and lysine (overall, 2 L), following a current practical guidance on receptor-targeted radionuclide therapies (19). As per our routine protocol, we also assessed vital signs and laboratory values (routine hematology and blood chemistry).
Administered Activities and Doses to Organs and Lymphoma
We also treated 1 patient (patient 3) with a CD66-targeting radioimmunotherapy, thereby increasing antilymphoma effects. 188Re was attached to the murine anti-CD66 monoclonal antibody BW 250/183 (antigranulocyte; Scintec Diagnostics) (16). Anti-CD66 radioimmunotherapy using 13.5 GBq was then performed 2 d after CXCR4 RLT using 90Y-pentixather.
Conditioning Chemotherapy/High-Dose Therapy and HSCT
Three (75%) patients received allogeneic HSCT, using an additional conditioning regimen, whereas 1 patient was treated with high-dose therapy followed by autologous HSCT (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
Assessment of Adverse Events and Outcome
We applied the Common Terminology Criteria for Adverse Events, version 5.0 (20). To assess short-term response to CXCR4-targeted RLT, we measured lactate dehydrogenase (in U/L) in all patients. A low-dose CT scan on patient 4, which had been conducted directly before conditioning therapy to rule out pulmonary infections, was also assessed for a short-term antilymphoma effect by CXCR4-directed RLT. The image-based best response was determined using the current Lugano criteria (21). Progression-free survival was defined as the time between initiation of RLT and progressive disease on imaging or the onset of novel therapy (16). Overall survival was determined as the time from initiation of RLT until the date of death or censoring.
RESULTS
Patient Characteristics
Between November 2015 and December 2021, we included 4 patients with relapsed, refractory TCL (2 women, 2 men); their median age was 50 y (range, 43–53 y). The investigated patients had a median of 3 previous treatment lines (range, 2–3; Supplemental Table 1). At the time of CXCR4 RLT, multiple manifestations in lymph nodes (n = 4 patients) and bone (n = 2), as well as in kidneys, pleura, spleen, skin, ovary, and abdominal bulk (n = 1 each), were recorded.
Pretherapeutic Dosimetry
Respective 177Lu-pentixather activities for pretherapeutic dosimetry are shown in Table 2, along with the specific absorbed dose to the kidneys, liver, spleen, bone marrow, and tumor (with the kidneys as the dose-limiting organs). We expected absorbed doses of up to 33.2 Gy to lymphoma from RLT.
CXCR4-Targeted RLT and Adverse Events
We administered a median of 4.8 GBq of 90Y-pentixather. Table 2 shows the estimated absorbed doses to the kidneys (assuming a 40% reduction by coinfusion of amino acids). During RLT, vital signs were normal and did not show any alterations in any patients. No acute toxicity, allergic reactions, or adverse events were recorded in 3 (75%) patients. In patient 4, however, an extensive CXCR4-positive tumor burden caused tumor lysis syndrome with transient grade 3 acute kidney failure 2 d after RLT (Fig. 1). In all patients, CXCR4-directed RLT (and additional radioimmunotherapy in 1 patient) caused the expected myeloablation, including neutropenia (<500/μL) a median of 11 d after therapy (range, 11–14 d). HSCT was then performed after a median of 14.5 d in all patients (range, 14–16 d). We observed successful engraftment with an absolute neutrophil recovery in 3 patients, whereas 1 patient (patient 1) died before reaching neutrophil reconstitution. Patients 3 and 4 reached engraftment after 12 d. In Patient 2, however, neutrophil reconstitution was not immediately successful after autologous HSCT but was reached after another conditioning therapy and allogeneic HSCT (2 mo after CXCR4 RLT, Supplemental Table 1).

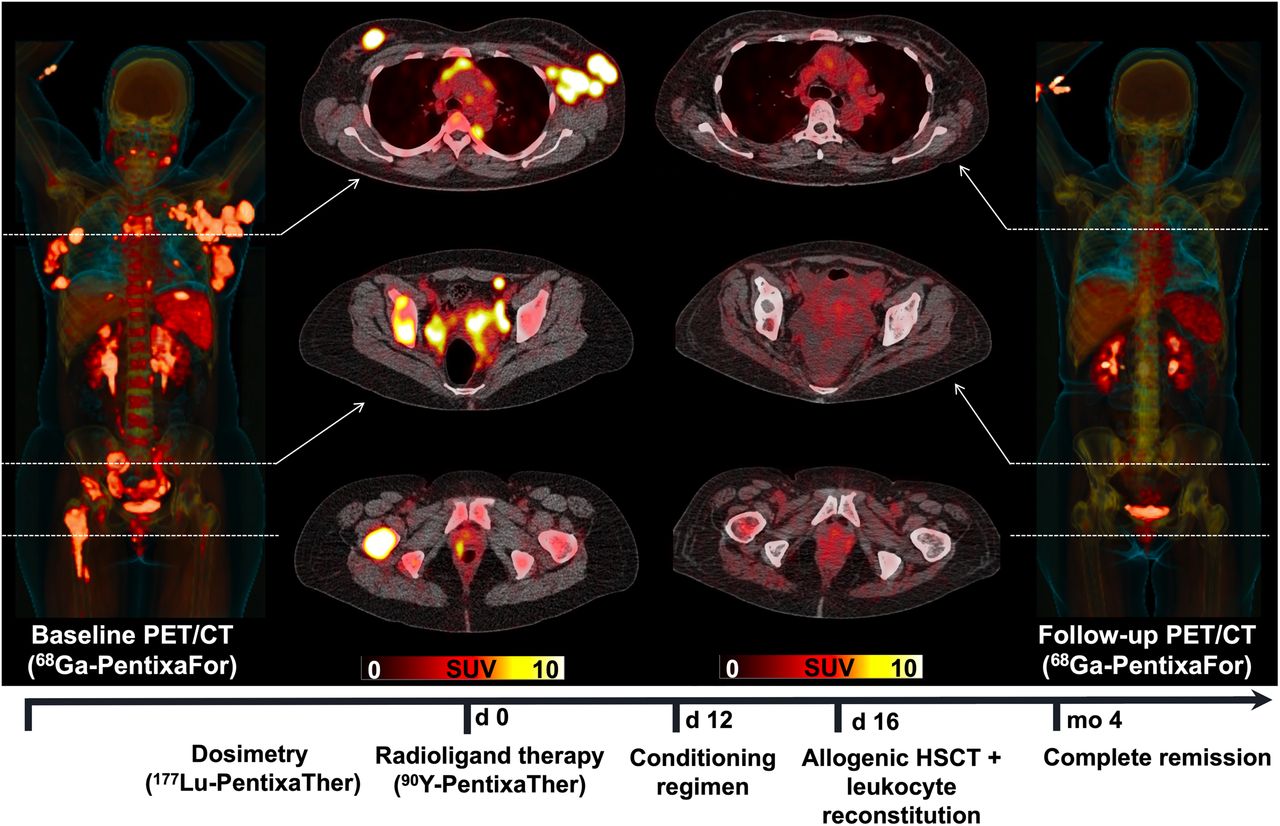
Complete metabolic response after CXCR4-directed RLT as conditioning regimen before allogeneic HSCT (patient 4). Maximum-intensity projections and transaxial CXCR4-directed 68Ga-pentixafor PET/CT before (left) and 4 mo after (right) CXCR4-directed RLT using 90Y-pentixather. Before therapy, patient demonstrated multiple CXCR4-positive sites of disease, including nodal, peritoneal, and osseous manifestations, whereas posttherapy imaging revealed complete response. Timeline of treatment is also displayed.
Response Assessment
Assessing short-term response, we observed a continuous decrease in lactate dehydrogenase right after CXCR4-targeted RLT in patient 1 (Fig. 2A). For patients 2 (Fig. 2B) and 4 (Fig. 2D), a substantial increase in lactate dehydrogenase right after CXCR4-targeted RLT was noted, which substantially declined before the next therapeutic steps. Further supporting the notion of a substantial antilymphoma effect exclusively due to CXCR4-directed RLT, low-dose CT in patient 4 (directly before conditioning therapy) also demonstrated a decrease in lymph node manifestations (Supplemental Fig. 1). Patient 1 died from sepsis caused by diffuse peritonitis 16 d after RLT (without any further available image-based follow-up). Of the 3 patients available for assessing the best response, we observed a partial response in 1 patient (patient 2; 33.3%) and a complete metabolic response in 2 patients (66.7%; patients 3 and 4).
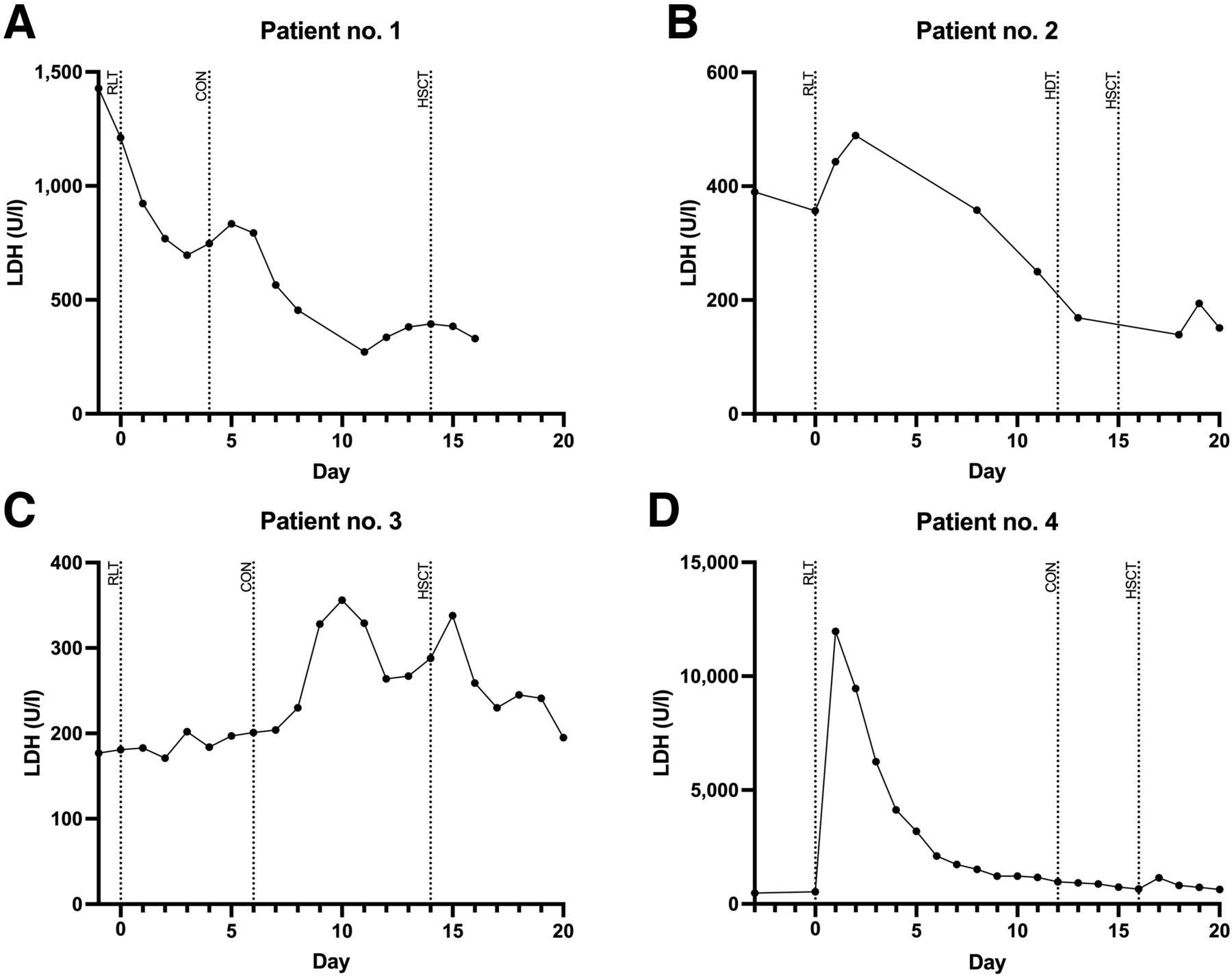
Time course of lactate dehydrogenase (LDH) (in U/L) as indicator of early response to CXCR4-directed RLT. Dotted lines indicate RLT, start of conditioning therapy (CON), start of high-dose therapy (HDT), or start of HSCT. Patient 1 (A) showed rapid and continuous decline in LDH after CXCR4-RLT. Before next therapeutic steps, patient 2 (B) and patient 4 (D) exhibited remarkable increase in LDH, followed by massive decline, supporting notion of immediate response to CXCR4-directed RLT in those 3 patients. Patient 3 (C), however, demonstrated modest LDH fluctuations between RLT and CON.
Further Long-Term Follow-up
Of those 3 patients available for further long-term follow-up, median progression-free survival was 7 mo (range, 4–25 mo), whereas for the entire cohort the median was 5.5 mo. Patient 2 exhibited progressive disease after 7 mo and received further regimens of chemotherapy and radiation therapy of inguinal lymph nodes. Patient 3 had progression after 25 mo; thus, a donor leukocyte infusion as adoptive immunotherapy was administered. Neither patient showed any signs of progression during further long-term follow-up. For patient 4, no further follow-up was available after complete response was recorded after 4 mo (as the date of censoring had been reached). All 3 patients (patients 2–4) were still alive at the time of censoring (respective median survival, 54 mo; range, 4–56 mo; entire cohort, median overall survival, 29 mo).
DISCUSSION
In the present case series, we demonstrated the feasibility of CXCR4-directed RLT in patients with heavily pretreated and relapsed or refractory TCL without suitable treatment options. Except for 1 patient experiencing tumor lysis syndrome (not life-threatening) along with transient grade 3 kidney failure, therapy was well tolerated, without any acute allergic reactions or toxicity. Although 1 patient died from neutropenia 16 d after RLT, engraftment was achieved in the remaining 3 patients (with 1 patient receiving additional radioimmunotherapy). Those patients demonstrated either a partial or a complete metabolic response (Fig. 1) and were alive at the date of censoring (median survival, 54 mo). Thus, our CXCR4-targeting theranostic approach may serve as an effective part of conditioning therapy before HSCT and can cause substantial antilymphoma activity, leading to remarkable responses in selected cases. Prospective phase I and II studies are now urgently needed to further corroborate our initial findings.
Similar to previous reports, we observed no acute adverse events during therapy, except for 1 case of tumor lysis syndrome causing a transient and non–life-threatening grade 3 kidney failure (17). However, given the increased CXCR4 expression in hematopoietic stem and progenitor cells within the bone marrow compartment (22), CXCR4 therapy led to the desired cytopenia, whereas patients were also at increased risk for infectious disease during follow-up. In our cohort, 1 patient succumbed to sepsis (caused by Enterococcus faecium and Escherichia coli) 16 d after RLT (patient 1). Such lethal infections, however, are not uncommon in the early posttransplantation phase (23). In the remaining 3 patients, successful engraftment could be achieved, along with remarkable outcome benefits. In those patients demonstrating a complete metabolic response (patients 3 and 4), no delay in treatment plan occurred and all needed therapeutic steps were performed as scheduled (including CXCR4-directed RLT, complete myeloablation, allogeneic HSCT, and successful engraftment). Patient 2, however, did not reach immediate successful neutrophil reconstitution after CXCR4 therapy and autologous HSCT and had to undergo another conditioning therapy with consecutive allogeneic HSCT. However, an additional CD66-directed 188Re radioimmunotherapy may have been used, as previously reported for diffuse large B-cell lymphoma (16). As such, in patients with an inadequate response to 90Y-pentixather alone, such CD66-targeting radioimmunotherapies or treatment with α-emitters (225Ac) could also be envisioned (24).
In lymphoma patients treated with total-body irradiation, increasing doses are tightly linked to improved response rates and survival (25,26). Such a trend was also observed in the present investigation, such as in patient 4, showing a lymphoma dose of up to 33.2 Gy and a complete response. This is in line with a previous investigation applying CXCR4-directed RLT for diffuse large B-cell lymphoma, also reporting doses of 40 Gy in selected cases (16). Although the critical renal dose of 23 Gy was not reached in any of our patients, patient 4 developed tumor lysis syndrome along with transient grade 3 kidney failure. Baseline 68Ga-pentixafor PET had already revealed an extensive CXCR4-positive tumor load with an SUVmax of up to 38.1 in selected target lesions (Fig. 1, PET quantification not shown). Thus, despite all precautions due to pretherapeutic dosimetry, those high-risk individuals with an extremely high tumor burden and intense 68Ga-pentixafor signal should be closely monitored. In this regard, future studies should also elucidate whether PET-based quantification, such as of the SUVs or CXCR4-avid tumor volumes, may hold potential to identify patients prone to an increased risk of developing relevant off-target effects, including tumor lysis syndrome. Such a quantification of pretherapeutic PET may also allow estimation of tumor doses without the need for time-consuming dosimetry or may even allow detection of patients who are most likely to benefit from treatment, as recently shown in the context of prostate-specific membrane antigen–targeted RLT for prostate cancer (27). On the other hand, a recent study did not observe a relevant tumor sink effect in oncologic patients scheduled for CXCR4-directed 68Ga-pentixafor PET (28). As such, in patients with advanced disease exhibiting a high tumor load, no decreased uptake in normal organs was noted, supporting the notion that tumor or normal-organ doses may be better calculated from pretherapeutic dosimetry as performed in the present study (28).
Our findings have to be interpreted with caution. In our cohort, substantial overall survival was noted during long-term follow-up, but CXCR4-directed treatment is part of a therapeutic algorithm also including HSCT; thus, the effects of pentixather are difficult to decipher from those of other concomitant therapies. Nonetheless, we observed either a continuous lactate dehydrogenase decline or an increase followed by a rapid decrease in this blood marker right after CXCR4-directed RLT, indicating a short-term response to pentixather. Further ruling out the effects of concomitant therapies is that patient 4 also demonstrated a reduction in lymph node manifestations on CT before conditioning therapy (Supplemental Fig. 1). The retrospective character and small number of patients should trigger future prospective studies. For instance, the COLPRIT phase I and II trial aims to provide further evidence on the impact of the theranostic concept using 68Ga-pentixafor and 177Lu/90Y-pentixather in advanced blood cancers.
CONCLUSION
For relapsed, refractory TCL, CXCR4-directed RLT may serve as an effective part of the conditioning regimen before HSCT and can cause substantial antilymphoma activity, leading to a remarkable response in selected cases. This feasibility study demonstrated that further prospective phase I and II studies are needed, which will define the role of implementing CXCR4-directed RLT in the treatment algorithm of TCL patients.
DISCLOSURE
This project is partially supported by the Okayama University “RECTOR” Program, the JSPS (KAKENHI 22H03027, Takahiro Higuchi), and the German Research Foundation (453989101, Rudolf Werner and Takahiro Higuchi). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can CXCR4-directed RLT exhibit substantial antilymphoma activity and serve as a conditioning regimen before HSCT in patients with refractory, relapsed TCL?
PERTINENT FINDINGS: Although 1 patient died from sepsis 16 d after RLT, engraftment was achieved in the remaining 3 patients. Those patients demonstrated either a partial or a complete metabolic response and were alive at the date of censoring, with a median survival of 54 mo.
IMPLICATIONS FOR PATIENT CARE: Our CXCR4-targeting theranostic approach may serve as an effective conditioning regimen before HSCT and can exhibit substantial antilymphoma activity, leading to a remarkable response in selected cases.
Footnotes
Published online Jun. 23, 2022.
- © 2023 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 29, 2022.
- Revision received June 13, 2022.





{kind=link}
{kind=link}
{kind=link}