


Abstract
2461
Introduction: Epidemiologic studies have established an association between markers of obstructive sleep apnea (OSA) severity and cardiovascular disease (CVD). Coronary microvascular disease (CMD) is a marker of CVD prognosis and a precursor to several CVDs including heart failure with preserved ejection fraction (HFpEF). However, no studies have examined the association between clinical and polysomnographic features of OSA and CMD. In this study we examine the association between markers of OSA severity such as the frequency of upper airway obstruction, hypoxia severity and clinical symptoms of sleepiness, with CMD.
Methods: This is a cross-sectional analysis of N=346 patients who underwent diagnostic overnight polysomnography and cardiac positron emission tomography (PET) perfusion imaging with rubidium (82Rb) within a large health care system from 2015-2019. Obstructive features were categorized using the apnea-hypopnea index (AHI) into three major groups mild or no OSA (AHI <15), moderate OSA (AHI 15 – 29), severe OSA (AHI 30 or more). Hypoxia severity was determined using the T90% index (percentage of sleep spent with < 90% O2 saturation) while sleepiness was defined as Epworth sleepiness scale (ESS) ≤15. We defined abnormal myocardial blood flow (MBF) reserve (MFR) as the ratio of stress to rest MBF <1.5 after rate-pressure product correction. Multivariate logistic regression analyses were conducted to compute the odds ratios (OR) of abnormal MFR for each of the OSA severity categories. The model was adjusted for age, sex, body mass index (BMI), current cigarette smoking, diabetes, hypertension, hyperlipidemia, history of stroke or transient ischemic attack (TIA), history of a myocardial infarction or revascularization. The analysis for the AHI was further adjusted for ESS and T90%.
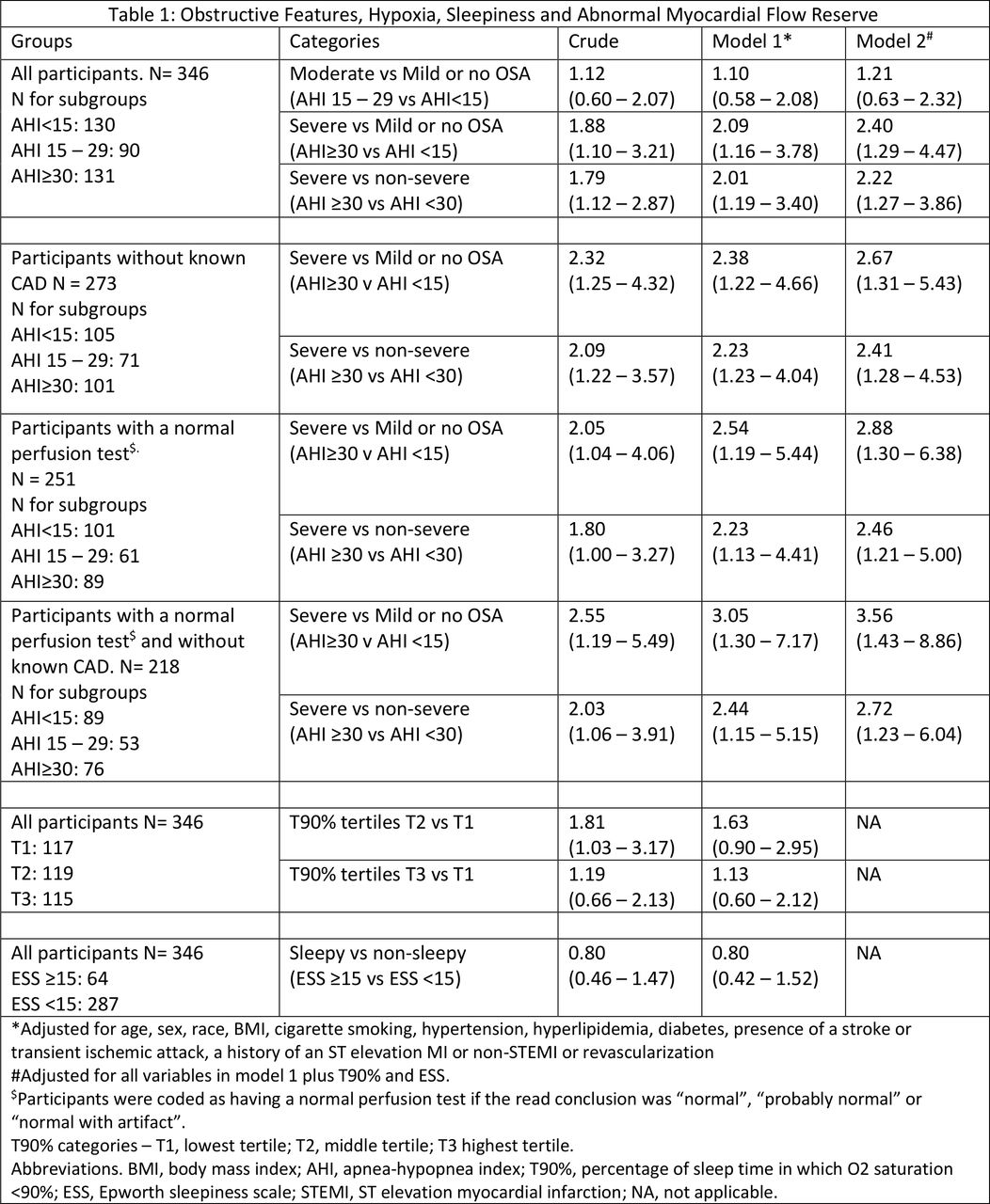
Results: Patients with abnormal MFR were older (62 vs 59 years). However, there was no association between gender, BMI, hypertension, hyperlipidemia, or race, and abnormal MFR. The frequency of abnormal MFR increased with worsening AHI (P trend 0.019). There was no statistically significant change in abnormal MFR frequency across T90% tertiles or between ESS groups. In both univariate and multivariate analyses, persons with severe OSA by AHI were more than twice as likely to have abnormal MFR compared to those with mild or no OSA (OR for fully adjusted model 2.40 [95% CI: 1.29 – 4.47]) or those with non-severe OSA (OR for fully adjusted model 2.22 [95%CI: 1.27 – 3.86]). The association between OSA severity by AHI and abnormal MFR was preserved when analysis was restricted to participants who did not have a prior CAD history and had a normal perfusion test (see table 1 for details). There was no interaction by age (≥60 years vs < 60 years), gender or race (Black, White, Hispanic) and AHI on the association with abnormal MFR. There was no association between T90% or sleepiness and abnormal MFR.
Conclusions: Severe airway obstruction in OSA was associated with abnormal MFR. This significant relationship persisted among those with normal perfusion tests and no prior CAD history indicating an association with CMD. The findings also suggest that the frequency of obstruction likely plays a major role in the pathogenesis of CMD in OSA and may be a better measure of CMD likelihood than hypoxia or sleepiness symptoms alone. Future studies should focus on the role of MFR in risk stratification and prognosis of patients with OSA and the impact of OSA-specific therapy on MFR.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.