


Visual Abstract

Abstract
In head and neck cancer, a major limitation of current intraoperative margin analysis is the ability to detect areas most likely to be positive based on specimen palpation, especially for larger specimens where sampling error limits detection of positive margins. This study aims to prospectively examine the clinical value of fluorescent molecular imaging to accurately identify “the sentinel margin,” the point on a specimen at which the tumor lies closest to the resected edge in real-time during frozen section analysis. Methods: Eighteen patients with oral squamous cell carcinoma were enrolled into a prospective clinical trial and infused intravenously with 50 mg of panitumumab-IRDye800CW 1–5 d before surgery. Resected specimens were imaged in a closed-field near-infrared optical imaging system in near real-time, and custom-designed software was used to identify locations of highest fluorescence on deep and peripheral margins. The surgeon identified the sentinel margin masked to optical specimen mapping, and then the regions of highest fluorescence were identified and marked for frozen analysis. Final pathology based on specimen reconstruction was used as reference standard. Results: Resected specimens were imaged in the operating room, and fluorescence had a higher interobserver agreement with pathology (Cohen κ value 0.96) than the surgeon (Cohen κ value of 0.82) for the location of the closest margin. Plotting margin distance at the predicted sentinel margin location of each observer versus the actual closest margin distance at pathology demonstrated best correlation between fluorescence and pathology (R2 = 0.98) with surgeon (R2 = 0.75). Conclusion: Fluorescence imaging can improve identification of the sentinel margin in head and neck cancer resections, holding promise for rapid identification of positive margins and improved oncologic outcomes.
- head and neck cancer
- oral squamous cell carcinoma
- tumor margins
- fluorescent image-guided surgery
- surgical oncology
In head and neck squamous cell carcinoma (HNSCC), surgery requires balancing complete tumor clearance with conservation of uninvolved tissue to preserve airway, voice, and swallowing. Achieving adequate margins can be challenging (1) and it is established that positive margins are associated with local recurrence and decreased overall survival. Even with advances in operative techniques and technology, positive margin rates have remained unchanged over the past 30 y (2,3).
Assessment of tumor specimens to identify positive margins after removal allows surgeons to resect further tissue from the wound bed is required to achieve adequate tumor clearance. This involves visual inspection and palpation of the specimen, with sampling of areas of concern from the specimen or wound bed for intraoperative frozen section analysis (FSA) (4). This process is inconsistent, surgeon-dependent, and complicated by sampling error in larger specimens.
Our group has previously demonstrated that ex vivo fluorescent imaging can identify the point on a specimen surface at which the tumor comes closest to the resection edge—the sentinel margin (5,6). The aim of the present study was to evaluate the accuracy and clinical value of fluorescent sentinel margin identification when compared prospectively to current clinical practice. We hypothesized that an objective, focused assessment of a specimen using optical imaging might reduce false-negatives during intraoperative margin assessment, maintain orientation of sampled areas on the specimen to the wound bed, and streamline the margin assessment process.
MATERIALS AND METHODS
Clinical Trial Design
Between June 2018 and December 2019, patients with biopsy-proven primary or recurrent oral squamous cell carcinoma scheduled for curative surgery were enrolled into a prospective single-center, nonrandomized, clinical trial evaluating a fluorescence molecular imaging agent called panitumumab-IRDye800CW. The institutional review board of Stanford University approved this study, and all subjects signed a written informed consent form. The trial was approved by the Food and Drug Administration (FDA) and registered with ClinicalTrials.gov (NCT03733210; NCT02415881; NCT03405142). This study was performed in accordance with the Helsinki Declaration of 1975 and its amendments, FDA’s International Conference on Harmonistaion-Good Clinical Practice (ICH-GCP) guidelines and the laws and regulations of the United States.
Study Workflow
Enrolled patients were infused intravenously with 50 mg of panitumumab-IRDye800CW 1–5 d before surgery (7). Dosing, timing, and safety information on panitumumab-IRDye800CW is provided in the supplemental materials (supplemental materials are available at http://jnm.snmjournals.org) (8–17).
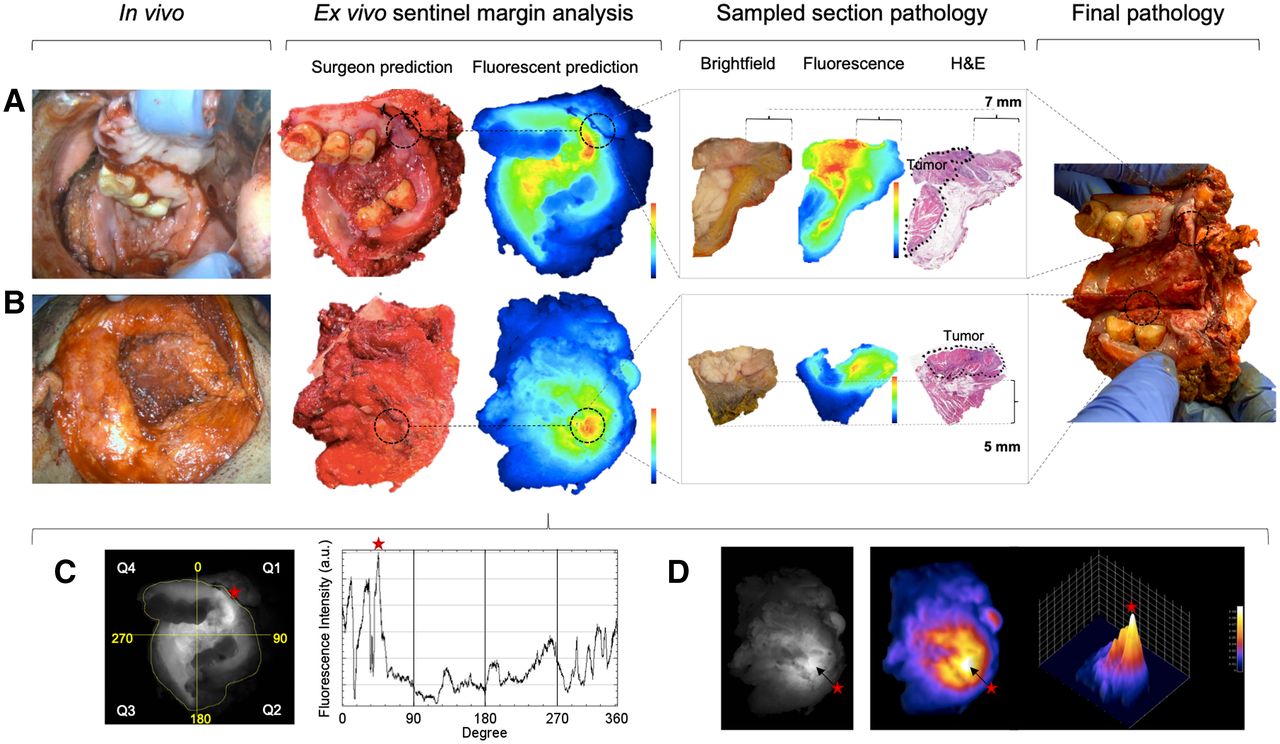
The study workflow is outlined in Figure 1. In the operating room, primary tumor specimens, as well as sampled margins for FSA, were imaged ex vivo on the back table immediately after removal from the patient in a closed-field near-infrared optical imaging system (IGP-ELVIS, LICOR Biosciences, Inc.) (18). All tumor resections were 3-dimensional and were therefore repositioned within the IGP-ELVIS to capture each surface in a 2-dimensional plane. Imaged surfaces were denoted mucosal if they primarily captured the mucosal aspect of the resection (Fig. 1A). All other surfaces were denoted deep (Fig. 1B). Only imaged surfaces that required pathologic evaluation by the surgical team were included in the study analysis.
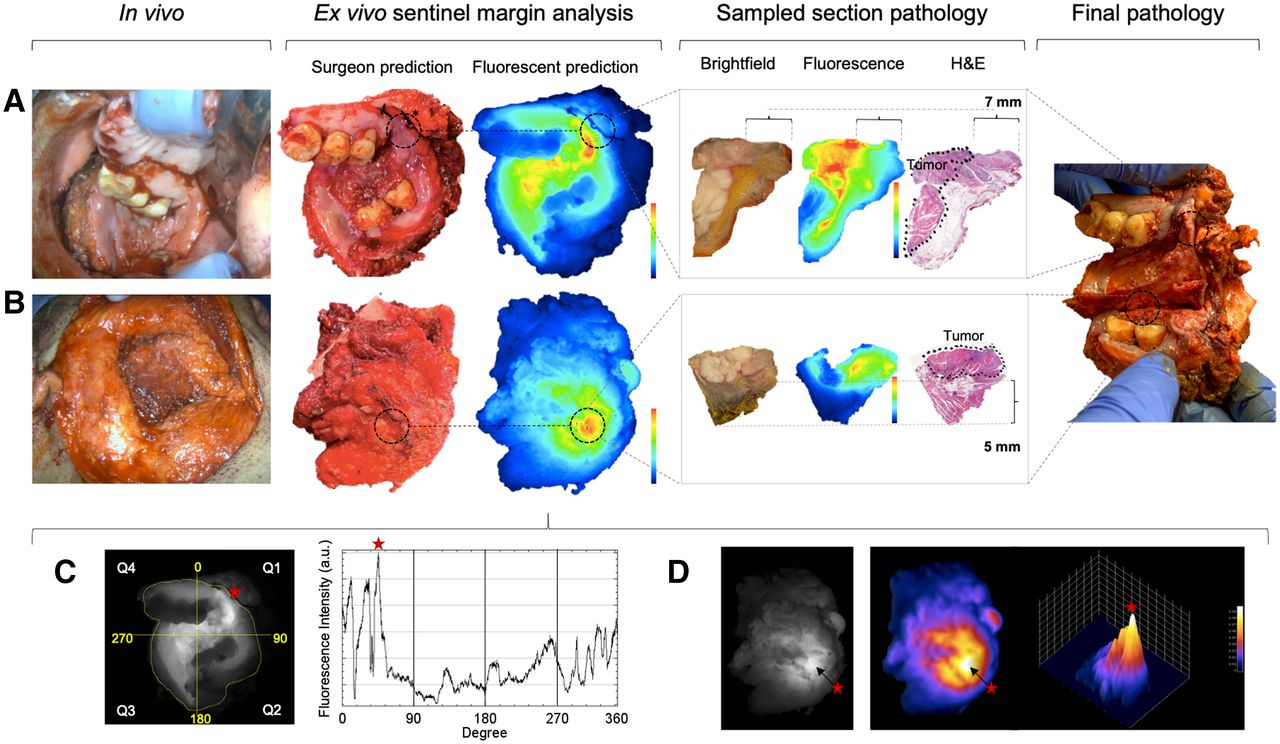
Study workflow is demonstrated in representative patient 18 with right-sided retromolar trigone squamous cell carcinoma. Patient was infused intravenously with 50 mg of panitumumab-IRDye800CW 3 d before surgery. From left to right, workflow shows lesion in vivo and then ex vivo, examining mucosal (A) and deep surfaces of resection (B). On both surfaces, surgeon and fluorescence were in agreement as to location of sentinel margin. Sampled tissue from these locations underwent closed-field fluorescent imaging and then hematoxylin and eosin (H&E) staining to evaluate margin distance. (C) Mucosal surface fluorescent sentinel margin analysis in this patient as demonstrated by a mask manually fitted around periphery of specimen within 1 mm of resection edge followed by graph showing the raw fluorescence data of each point along mask in 8-bit gray scale format enabling isolation of area of highest fluorescence on periphery (represented by red star). (D) Deep surface fluorescent sentinel margin analysis as demonstrated using 3-dimensional signal-mapping tool to scale and isolate area of highest fluorescence intensity (represented by red star and arrow).
Acquired images were exported as TIFF files from the optical imaging system to a laptop for near-real-time fluorescent analysis of the sentinel margin using ImageJ software (version 1.50i; National Institutes of Health) as previously described (5,6).
To compare our fluorescent analysis against current clinical practice, the board-certified surgeon, masked to fluorescence, was asked to identify the point at which the tumor came closest to the specimen edge ex vivo. This was often done at pathology in collaboration with the pathologist. Their specimen orientation and sentinel margin demarcation was photo- and video-documented. This photo was then used to compare the point of highest fluorescent signal on that surface by registering the 2 images against each other. A margin of error equivalent to 1 bread loaf at pathology was used when comparing each prediction against final pathology as gold standard. Individual bread loafs are approximately 5 mm thick (19); therefore, if the surgeon or fluorescence is within 5 mm of the true sentinel margin, this would fall within the realm of “close enough” to ink, activating the pathologist select radial margins in the area of concern. Where there was clinical concern that the specimen had close or positive margins, FSA was performed on the presumptive sentinel margins demarcated by the surgeon. These frozen sections were processed and analyzed as standard of care, and the results were reported to the operating team for intraoperative action as appropriate. Margins were defined in this study as clear if ≥5 mm from invasive tumor, close if <5 mm from invasive tumor, and positive if invasive carcinoma or carcinoma in situ was present at the specimen edge (20,21).
Primary tumor specimens underwent routine pathologic processing and assessment, and all tissue cassettes were reimaged in the IGP-ELVIS before paraffin-embedding. A standard synoptic report was generated by a board-certified pathologist, including identification of the final closest margin location and distance on mucosal and deep surfaces as seen on hematoxylin and eosin slides, serving as gold standard to compare the sentinel margin predictions of the surgeon and fluorescence. Epithelial growth factor receptor (EGFR) immunohistochemistry and expression quantification of selected slides were performed as previously described (22).
To map all predicted sentinel margin locations against final pathology, locations were recorded categorically according to which pathology cassette they belonged to. Where 2 sentinel margin predictions were located on separate areas of a same cassette, they were differentiated with reference to their orientation on the cassette. A ruler was used to measure distance in millimeters from tumor edge (marked by the pathologist) to the specimen edge at each predicted sentinel margin on hematoxylin and eosin slides. Mean fluorescence intensity, defined as total counts per pixel area, divided by pixel area, was calculated for each acquired image of tissue taken intraoperatively for FSA using ImageStudio software (LI-COR Biosciences). Mean fluorescence intensity data were correlated to final tumor status (positive or negative).
Statistical Analysis
SciPy (version 1.4.1; open source), Scikit-learn (version 0.22.2; open source), and GraphPad Prism (version 8.0c; GraphPad Software) were used for statistical analysis. A Cohen κ statistic was used to assess the strength of agreement of sentinel margin location of the 2 observers (surgeon and fluorescence) independently against the gold standard (final pathology). The accuracy and error rate of sentinel margin location of each observer were calculated using standard statistics. The 95% CI of each observer’s accuracy was calculated using a t distribution. Accuracy P values were calculated based on the number of cassettes for each specimen, with respect to random choices. Pearson and Spearman correlation coefficients were calculated for margin distances at predicted sentinel margin locations of each observer against the actual closest margin distance at final pathology. A 2-sided P value of 0.05 or less was considered statistically significant.
RESULTS
Observer Agreement and Accuracy in Sentinel Margin Prediction
Primary tumor specimens from 18 patients were included in this study, with 28 specimen surfaces imaged and analyzed. The predicted sentinel margin location and corresponding measured margin distances at these locations per observer compared with final pathology are summarized in Table 1. Overall, areas of highest fluorescence strongly correlated final pathology (Cohen κ, 0.96). The surgeon had a relatively lower correlation with final pathology (Cohen κ, 0.81).
Summary of Interobserver Prediction of Sentinel Margin Location and Corresponding Margin Distance Versus Actual Closest Margin Location and Distance at Pathology
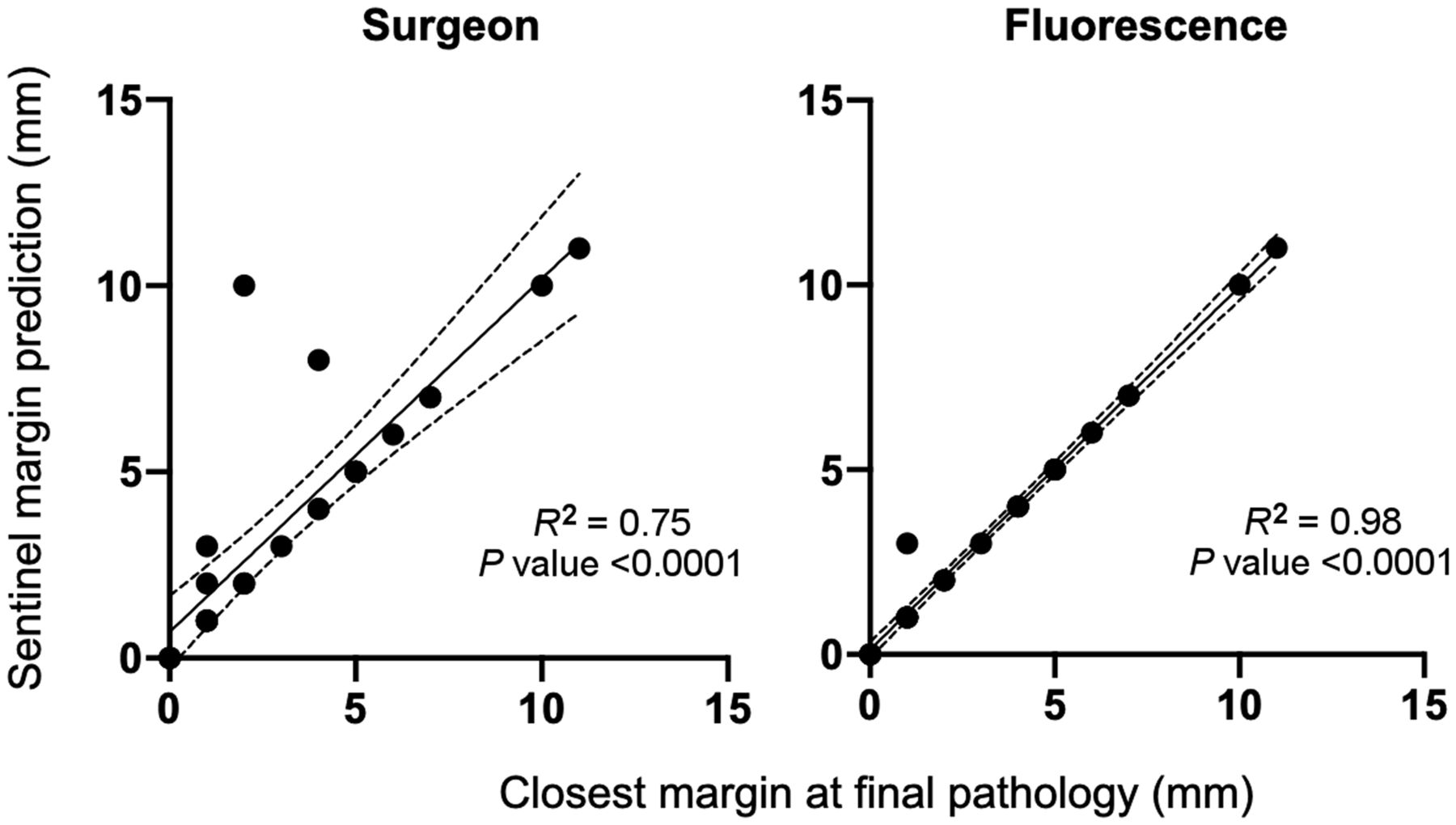
The accuracy of fluorescence intensity to identify the true sentinel margin was 96.4% (95% CI, 89.1–100; P < 0.001) compared with the surgeon at 82.1% (95% CI, 67.0–97.3; P < 0.001) as summarized in Table 2. Plotting margin distance at the predicted sentinel margin of each observer versus the actual closest margin distance at final pathology demonstrates better correlation between fluorescence and final pathology (R2 = 0.98; 95% CI, 0.93–1.00; P < 0.001) compared with the surgeon and final pathology (R2 = 0.75; 95% CI, 0.73–1.17; P < 0.001) (Fig. 2).
Accuracy of Observer at Identifying Final Closest Margin Location

Correlation between distance at predicted sentinel margin by observer with distance of closest margin on final pathology.
Clinical Value of Fluorescence in Sentinel Margin Analysis
The surgeon’s prediction of the sentinel margin disagreed with final pathology in 4 of 28 cases compared with 1 of 28 cases with fluorescence. In the 1 instance in which fluorescence disagreed with final pathology, the fluorescent-predicted sentinel margin location was in concordance with the surgeon’s prediction. This agreement equates to a clinically significant improvement in intraoperative frozen section sampling in 3 of 28 (10.7%) surfaces analyzed with fluorescence over current standard of care.
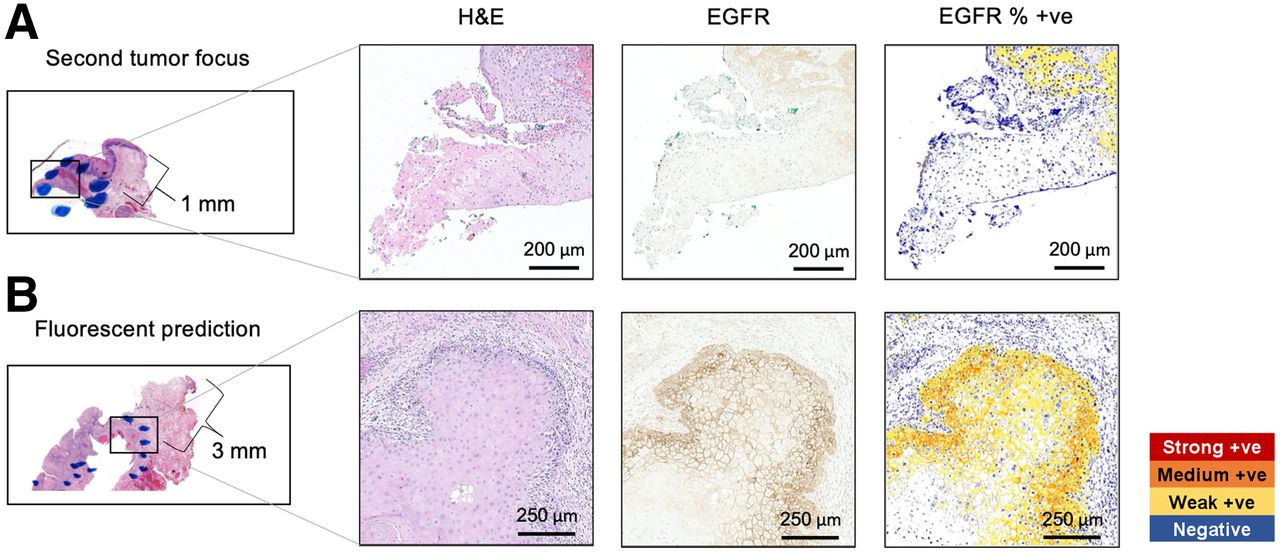
Closer examination of the 1 case in which there was tumor close to the mucosal surface that was not identified by fluorescence as being the area of highest signal revealed that this tumor was in fact a small secondary focus (Fig. 3). Immunohistochemistry staining and EGFR quantification of regions in which each focus of tumor came closest to the peripheral margin demonstrated EGFR expression at both points, but with higher EGFR expression (81.2%) where there was macroscopically visible disease on the main tumor focus versus (43.2%) on the smaller secondary focus (Fig. 4).

(A) Specimen evaluation workflow demonstrating partial glossectomy resection in situ, ex vivo specimen imaged in brightfield and closed-field fluorescence, followed by a depiction of specimen bread-loafed at final pathology. (B) Main centrally located tumor came closest to specimen edge superiorly, at a point accurately identified by both fluorescence and surgeon to be closest margin for this tumor (3 mm). Smaller separate focus of tumor was not macroscopically visible and registered as third highest region of fluorescent signal on peripheral margin. Blue dots outline tumor boundaries on mucosal surface. BF = brightfield; FLU = fluorescence; H&E = hematoxylin and eosin.
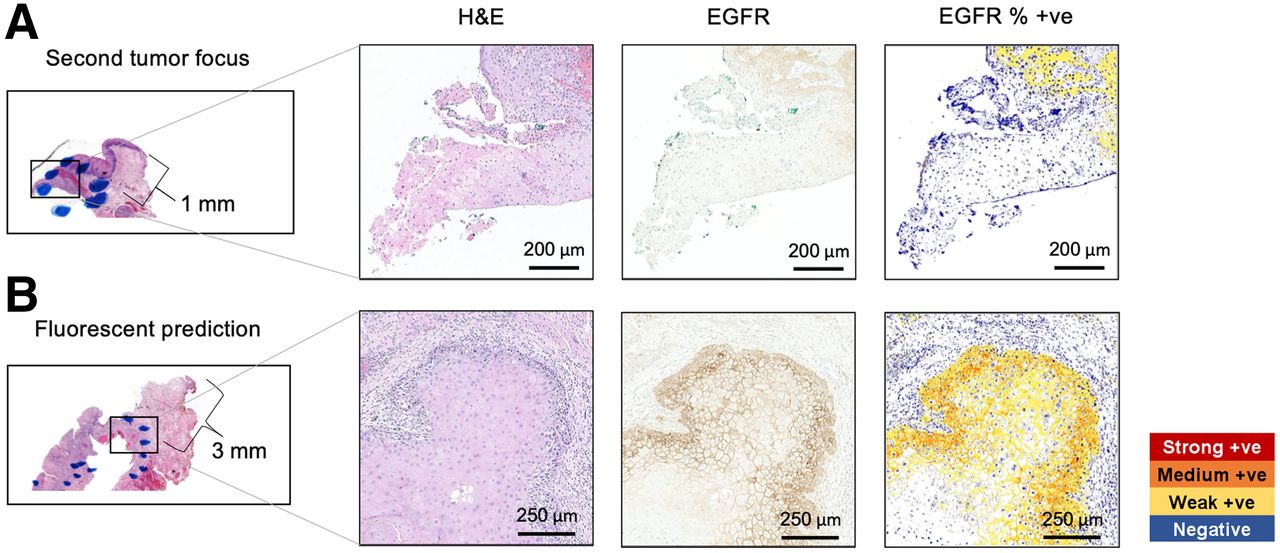
(A) Magnified view of 2 bread loafs demonstrating margin distance of 3 mm, where surgeon and fluorescence predicted sentinel margin on main tumor, compared with margin distance of 1 mm where a sperate secondary focus of tumor came close to anterior specimen edge. (B) Slides confirming presence of squamous cell carcinoma and EGFR expression at point on each tumor focus closest to margin edge. In main tumor, EGFR expression was quantified at 81.2% compared with 43.2% at secondary focus. +ve = positive; H&E = hematoxylin and eosin.
In 3 cases in which the fluorescent sentinel margin prediction outperformed conventional palpation by the surgeon, the final margin was close (<5 mm) in all cases, as summarized in Figure 5.

Cases in which fluorescence sentinel margin identification demonstrated improved identification of true closest margin when compared with conventional analysis technique by surgeon. (A) Patient 1 with a pT3 right lateral tongue squamous cell carcinoma infused 2 d before surgery. (B) Patient 2 with pT4a right lateral tongue squamous cell carcinoma infused 1 d before surgery. (C) Patient 13 with a pT4a right retromolar squamous cell carcinoma infused 2 d before surgery. BF = brightfield; Flu = fluorescence; H&E = hematoxylin and eosin.
DISCUSSION
This prospective study compares fluorescence with current intraoperative margin assessment, evaluated against final pathology as the gold standard. It builds on previous retrospective studies in which we developed the concept of sentinel margin detection using relative fluorescence intensities and showed that margin distance inversely correlates with areas of highest fluorescent intensity on the deep and mucosal surfaces (5,6). These studies laid the foundation for the current prospective trial but were limited by their retrospective nature, which meant that only specimens for which measurable bread loafs coincided with the intensity peaks on the deep surface, or areas of highest fluorescence intensity on the peripheral surface, could be included for analysis. Tissue is relatively homogeneous, thereby disrupting optical properties and enabling this technique to work consistently across specimens. Furthermore, although EGFR is heterogeneous across the different patient cancer specimens, it is high enough to allow fluorescence to penetrate through the tissue margin. This study, unlike previous research in this technique, is a prospective comparison to the surgeon.
This study demonstrates that ex vivo fluorescent molecular imaging of head and neck resections can improve objective detection of tumor that comes closest to the specimen edge when compared with standard of care, which was exemplified in 11% of cases in which fluorescence-based sentinel margin assessment outperformed standard-of-care pathologic assessment by the surgeon, suggesting this approach has potential to improve positive margin rate outcomes. Accurate isolation of the sentinel margin in the operating room within minutes has several benefits. Of highest clinical priority, it holds promise to minimize false-negative intraoperative margin assessment (23). From a resource-use standpoint, reduced tissue sampling and reduced FSA streamline operative workflow and decrease pathology demand (24,25). By identifying the sentinel margin in the operating room immediately after resection, there is promise for improved in vivo and ex vivo orientation of the specimen to the wound bed, which could increase precision during wound bed reresection, although this was not assessed here and requires focused evaluation in future studies (26,27). Anecdotally in this study, fluorescence imaging followed by sentinel margin analysis took approximately 5–10 min to complete (depending on the complexity of the specimen and how many surfaces were being imaged) whereas frozen sectioning typically takes 20–30 min per FSA. Hence, additional benefit can be found in providing directional information to the pathologist for areas to be assessed by FSA.
All 18 HNSCC specimens in this study originated from the oral cavity, but resection units varied, including glossectomies, maxillectomies, mandibulectomies, and composite resections. Our findings demonstrate that fluorescence molecular imaging of complex 3-dimensional resections involving soft tissue and bone is feasible and this is a significant strength of this study, as current ex vivo margin analysis in these complex specimens is particularly difficult (28). It is in these resections that there is a short window of opportunity for surgeon orientation of specimen to wound bed and where communication of margin locations between surgeon and pathologist are prone to error (29).
Before undertaking this study, we hypothesized that specimen positioning and intratumoral heterogeneity of EGFR could impact accuracy of fluorescent sentinel margin identification. In this study, we identified a case in which a smaller tumor satellite with both an associated lower EGFR expression and a lower fluorescence intensity resulted in a false-negative outcome because it lay closer to the resection edge than the main tumor focus. On the basis of this finding, and in line with the results of our previous studies, we would advise that at least 2–3 regions of highest fluorescent signal on a specimen surface be sampled (6). Sampling the 3 areas of highest fluorescence on the peripheral margin would have picked up this separate focus of microscopic disease that was not visually detectable or palpable, consistent with our previous studies (7).
In 1 of the 3 cases in which fluorescence was superior to surgeon sentinel margin prediction, the standard approach still identified a close margin of 2 mm. This highlights an important clinically relevant point, that there may be more than 1 location on a specimen surface, and multiple surfaces on 1 specimen, in which the tumor comes close to the resection edge. It is precisely in these cases where fluorescence can be of significant added value, as reresection from the wound bed at multiple locations may be necessary and without fluorescence guidance may be missed. The specimen imaging techniques are agnostic to the fluorescent agent used and may thus also apply beyond paniatumumab-IRDye800CW (30–32). It is worth mentioning that nonfluorescent optical dyes have been investigated for margin analysis with promising results (33–35).
There are study limitations worth highlighting. First, for a specimen surface whereby the surgeon or pathologist was not concerned about having close margins, fluorescence analysis and FSA were not performed in order to reduce time and allow focus on clinically relevant margin assessment, consistent with the philosophy that the margin assessment strategy should be used for clinical guidance only. Moreover, we did not examine margin distances at high fluorescent areas on specimen surfaces in which there was no clinical suspicion for close margins. As such, we cannot comment on the accuracy of fluorescent imaging at identifying the sentinel margin on all surfaces of all specimens resected in this study. Future trials could circumnavigate the issue of intraoperative delay, by prospectively collecting tissue samples at pathology of the identified sentinel margin location on all surfaces of all specimens (based on both fluorescent analysis and surgeon prediction) and then retrospectively analyze the margin distances on these tissue samples later. Second, fluorescence margin analysis in this study was performed by 1 person. Although this kept variability in fluorescent margin analysis and interpretation constant, a learning curve for performing the analysis and discrepancies in analysis between users was not examined. With increasing adoption of artificial intelligence technology in surgery, it is foreseeable that future use of this strategy may move toward computer-automated techniques.
CONCLUSION
Image-guided analysis of specimens can improve identification of the true closest margin in 3-dimensional resections with the potential to reduce positive margin rates. Results of the current study determined a clinically significant value of fluorescence-based margin assessment in 11% of patients. A study examining the value of this technique in improving communication of margin location between surgeon and pathologist as well as evaluating the efficacy of surgery-guided reresection should follow.
DISCLOSURE
This work was supported in part by the Stanford Comprehensive Cancer Center, the Stanford University School of Medicine Medical Scholars Program, the Garnett Passe and Rodney William’s Memorial Foundation, the Fulbright Association, The Netherlands Organization for Scientific Research (Rubicon; 019.171LW.022), the National Institutes of Health and the National Cancer Institute (R01CA190306), the Stanford Molecular Imaging Scholars (SMIS) program (T32CA118681), and an institutional equipment loan from LI-COR Biosciences, Inc. Eben L. Rosenthal served as a consultant for and has institutional equipment loans from LICOR Biosciences and Stryker. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How does ex vivo fluorescent molecular imaging of head and neck cancer resections compare with current standard of care in identifying the true closest margin?
PERTINENT FINDINGS: In this prospective observational clinical trial including 18 consecutive patients who underwent head and neck cancer surgical resections, fluorescence-based sentinel margin assessment outperformed the surgeon at identifying the true closest margin at final pathology in 11% of cases. Fluorescence had a higher interobserver agreement with final pathology (Cohen κ, 0.96) than the surgeon (Cohen κ, 0.82), and plotting the margin distance at the predicted sentinel margin location of each observer versus the actual closest margin distance at final pathology demonstrated best correlation between fluorescence and final pathology (R2 = 0.98).
IMPLICATIONS FOR PATIENT CARE: Broad translation of an ex vivo fluorescent molecular image–based approach to sentinel margin identification could improve accuracy of intraoperative margin sampling, with overall potential to reduce positive margin rates in surgery.
Footnotes
Published online Jan. 13, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
Immediate Open Access: Creative Commons Attribution 4.0 International License (CC BY) allows users to share and adapt with attribution, excluding materials credited to previous publications. License: https://creativecommons.org/licenses/by/4.0/. Details: http://jnm.snmjournals.org/site/misc/permission.xhtml.
REFERENCES
- Received for publication March 3, 2021.
- Accepted for publication November 16, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.