


After years of development and many published studies, prostate-specific membrane antigen–targeted radioligand therapy recently reached a critical milestone on March 23, 2022, with approval of 177Lu-PSMA-617 by the U.S. Food and Drug Administration (1). This landmark success heralds a new era of large-scale theranostics for nuclear medicine. This editorial provides the first-hand perspective on the origins of the phase III VISION trial and, specifically, the creation of the imaging criteria for selection of patients for PSMA-targeted therapy.
ENDOCYTE: A PHOENIX RISEN FROM THE ASHES
Endocyte was founded in 1996 to develop small-molecule drug conjugates and imaging agents targeting the folate receptor (2). In 2012, Endocyte entered into a license agreement with Merck & Co. for codevelopment of a folate-targeted theragnostic for women with platinum-resistant ovarian cancer. Two years later, Endocyte received a positive opinion for conditional marketing authorization from the Committee for Human Medicinal Products for the combination of the folate-targeted small-molecule drug conjugate and a companion SPECT diagnostic for patient selection. Shortly after, Endocyte withdrew the conditional marketing authorization application because the phase III trial failed the predefined futility analysis. During that same time, Endocyte expanded its portfolio to include prostate-specific membrane antigen (PSMA)–targeted theranostics and initiated a phase I trial investigating a PSMA-targeted small-molecule drug conjugate and 99mTc-based PSMA-targeted SPECT tracer for prostate cancer (3).
While analyzing the failure of the folate-targeted theragnostic trial (4), Endocyte restructured the organization and explored in-licensing opportunities. Leveraging of the company’s history with theranostics and patient selection experience, along with the growing recognition of the potential of PSMA-targeted radioligand therapy, Endocyte announced the worldwide licensing agreement for 177Lu-PSMA-617 with ABX GmbH in October 2017. The team then quickly worked to initiate the phase III trial “177Lu-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer” (VISION). Endocyte decided to use 68Ga-PSMA-11 PET/CT for patient selection and entered into a supply agreement with Telix to use its PSMA-11 kit for sites that did not have an active 68Ga-PSMA-11 investigational-new-drug authorization. Less than a year after acquisition of PSMA-617, the first patient was enrolled in the VISION study. Along with overall survival, imaging-based progression-free survival was negotiated by Endocyte with the Food and Drug Administration as an alternate primary endpoint. In October 2018, Novartis announced its intent to acquire Endocyte—an event that completed the story of Endocyte’s rising from the ashes. On March 23, 2021, Novartis announced the successful results of the VISION trial, approximately 3.5 y after Endocyte’s acquisition of the exclusive license for PSMA-617 (5).
FORMULATING THE PSMA PET SELECTION CRITERIA
The first decision was whether to even use imaging for patient selection. For example, if imaging excluded only less than 10% of patients, would it be worth the added effort, expense, and complexity to the trial? On the other hand, if selection were too restrictive, patients could be excluded who might otherwise benefit from 177Lu-PSMA-617. After consulting with a variety of opinion leaders, a 10%–20% exclusion rate by imaging was targeted as an optimal compromise between too restrictive and not restrictive enough, which was achieved in the trial. At the time (and arguably still), there were not enough robust data in the public domain to inform a definitive exclusion rate and set expectations based on efficacy outcomes in this patient population using PSMA PET. In addition to the complex task of maximizing the likelihood of successfully reaching efficacy endpoints, one must balance the feasibility and thus reproducibility of the reading criteria. Relating novel criteria to existing, familiar, criteria may improve the likelihood of successful implementation.
The next decision was whether to use PSMA PET alone or to combine PSMA and 18F-FDG PET. At that time, the combination of PSMA and 18F-FDG PET had been advantageously used to evaluate for low PSMA uptake by PSMA PET, as well as for discordant lesions by combining PSMA and 18F-FDG PET (6). After careful consideration, it was decided to use PSMA PET/CT in combination with the diagnostic CT, because adding 18F-FDG PET presented potential operational complexity and cost in the execution of a large, global clinical trial. However, when considering patients in a standard-of-care clinical setting, addition of 18F-FDG PET/CT to improve patient selection could save money (7). In a large, global clinical trial setting, 2 scans versus 1 scan could increase variability in readings. Future issues with reimbursement of PET could occur with both 18F-FDG and PSMA PET, but PSMA PET was considered more essential given the patent necessity for assessing the PSMA expression of tumors for this targeted therapy.
A definition for “PSMA-positive” and “PSMA-negative” was created specifically for this trial. In this context, the definition of PSMA positivity was designed not to localize prostate cancer but to identify tumors with sufficient target expression that would likely respond to therapy. The use of an SUV cutoff was not chosen for this global trial given the variability of SUV across clinical sites and the known challenges of standardization and certification. Visual assessment against an appropriate internal reference was chosen. Blood pool was too low as a reference, and using multiples of the blood pool would require measuring SUVs. Spleen was considered, which often has high uptake and thus the possible advantage of a more stringent threshold. Preliminary evaluation of splenic uptake in PSMA PET scans revealed there was too much variability (unpublished data, Phillip H. Kuo, February 2018). Finally, some patients might not have a spleen, which would preclude that as a universal reference organ. The commonly used Deauville criteria for 18F-FDG PET for lymphoma uses the liver as a reproducible visual internal reference standard (8). The team defined PSMA positivity as “greater than liver” rather than “equal to or greater than liver” to provide a more stringent selection. Given the prior Endocyte experience with grading levels of activity on folate-receptor imaging, a binary assessment (PSMA positivity or negativity) was chosen.
CT can be used to identify aggressive tumors, which would then be assessed on the PET/CT scan for level of PSMA uptake. To aid with reproducibility, we used the familiar RECIST 1.1 as a foundation. Assessment of anatomic imaging was divided into 3 systems: lymph nodes, solid organs, and skeleton. The need to identify and accurately measure lesions for determination of PSMA status requires high-quality anatomic imaging and careful reads by imagers.
First, the lymph node category was addressed. The ALSYMPCA trial with 223Ra-chloride included patients with lymphadenopathy up to 3 cm in short-axis diameter and showed that benefit in overall survival could be achieved in patients with bone metastases without treating nodes up to 3 cm (9). If a patient had extensive, nonnodal disease with intense uptake on PSMA PET but PSMA-negative nodes, we surmised that patients would still likely benefit. Instead of a 3-cm threshold, 2.5 cm in short-axis diameter was ultimately used for greater stringency.
Next, the solid-organ and parenchymal metastases were considered. Like the size criteria for target lesions in RECIST 1.1, only disease at least 1.0 cm in short-axis diameter would be assessed for PSMA status. The need to identify metastases down to 1.0 cm in short-axis diameter emphasizes the need for careful evaluation of the anatomic imaging, since a PSMA-negative metastasis could be more difficult to identify on PET imaging. Unfortunately, at 1.0 cm in short-axis diameter, activity could be underestimated because of the partial-volume effect, but it would be critical to include metastases down to this size given the impact of parenchymal metastases on survival.
Finally, the skeletal system was particularly challenging. Because the patient population in the VISION trial would be previously treated with multiple therapies, it would have been difficult to distinguish between healed, sclerotic metastases and active sclerotic disease on CT. Thus, a focus on aggressive or destructive bone disease with a soft-tissue component was pursued. Like the size criteria for target lesions in RECIST 1.1, the reader would assess only those bone metastases with a soft-tissue component at least 1.0 cm in short-axis diameter, and only the soft-tissue component would be assessed for level of activity.
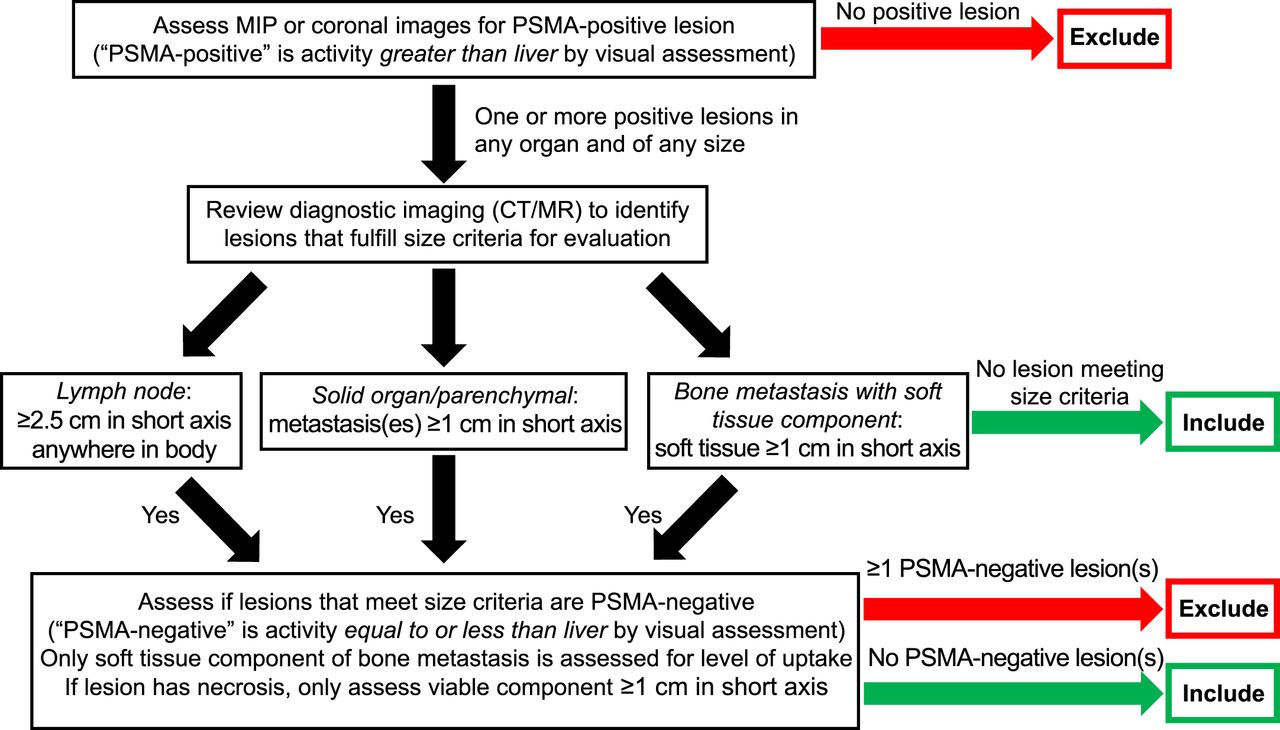
The first step in the reading criteria is assessing the PSMA PET images for at least 1 PSMA-positive lesion (of any size) to ensure the presence of targetable disease (Fig. 1). The reader then evaluated the anatomic imaging for lesions that met the size criteria for assessment of PSMA status (Fig. 1). One or more PSMA-negative lesions resulted in exclusion (Figs. 1 and 2). The rationale was that 1 PSMA-negative lesion of adequate size for assessment could represent only a portion of the PSMA-negative disease reservoir that would not respond to PSMA-targeted therapy. This was also important for the imaging-based progression-free-survival endpoint. Theoretically, PSMA-positive disease would respond promptly after the initial cycles of 177Lu-PSMA-617 but even 1 PSMA-negative lesion would continue to grow and, therefore, the sum of the diameters of the target lesions would increase to progression of disease soon after nadir. A major concern was potentially excluding good responders who have high uptake in many lesions except one. Use of cutoffs such as greater than 70%, 80%, or 90% of lesions positive was considered. Prior unpublished Endocyte experience with folate imaging demonstrated that this methodology adds significant variability and complexity to the reading (unpublished data, Phillip H. Kuo et al., October 2013). Ultimately, the original exclusion criterion of one or more PSMA-negative lesions was maintained.
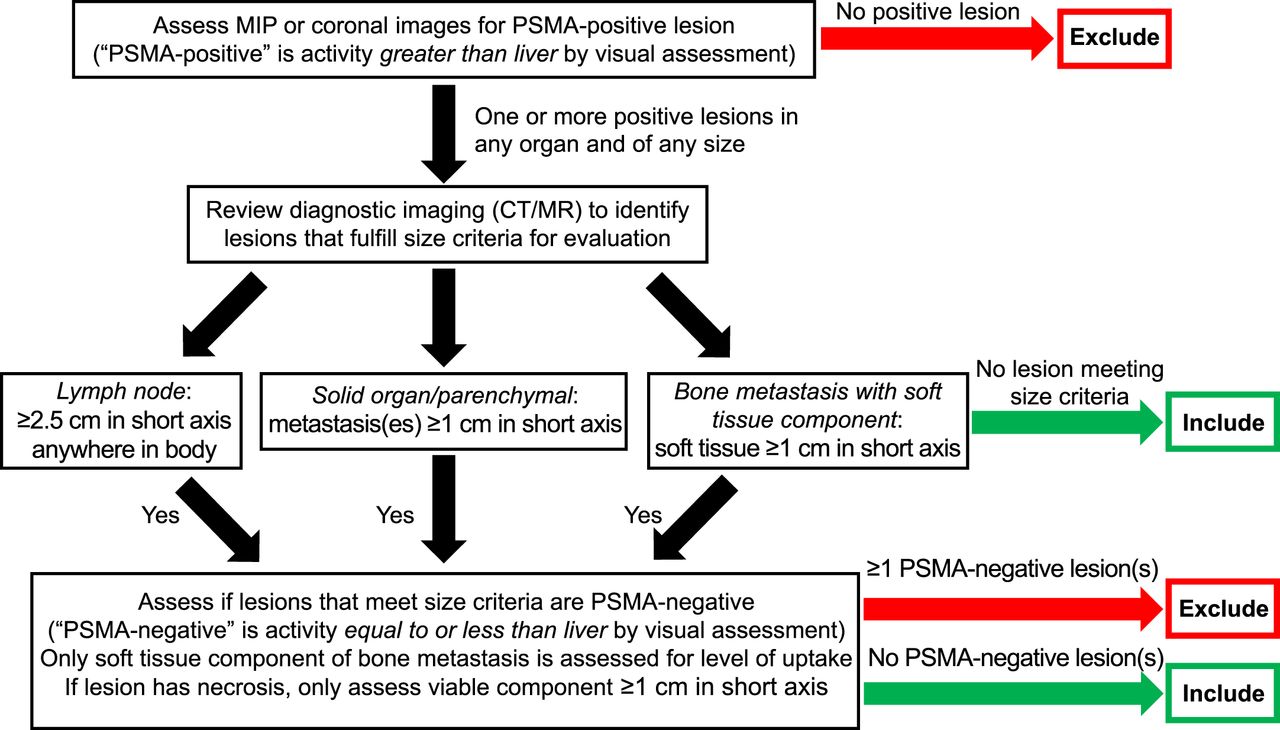
Reading methodology of VISION trial for patient selection. MIP = maximum-intensity projection.
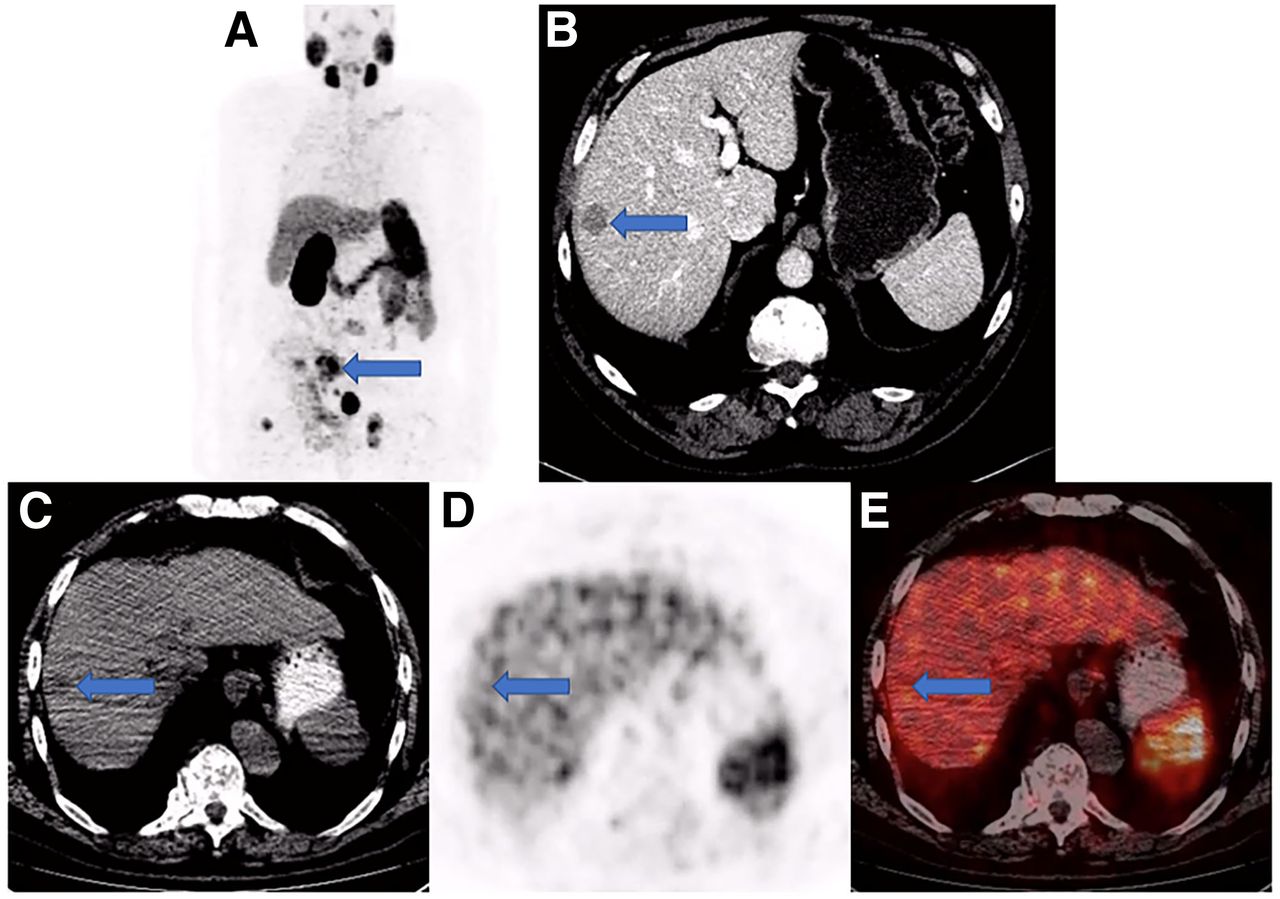
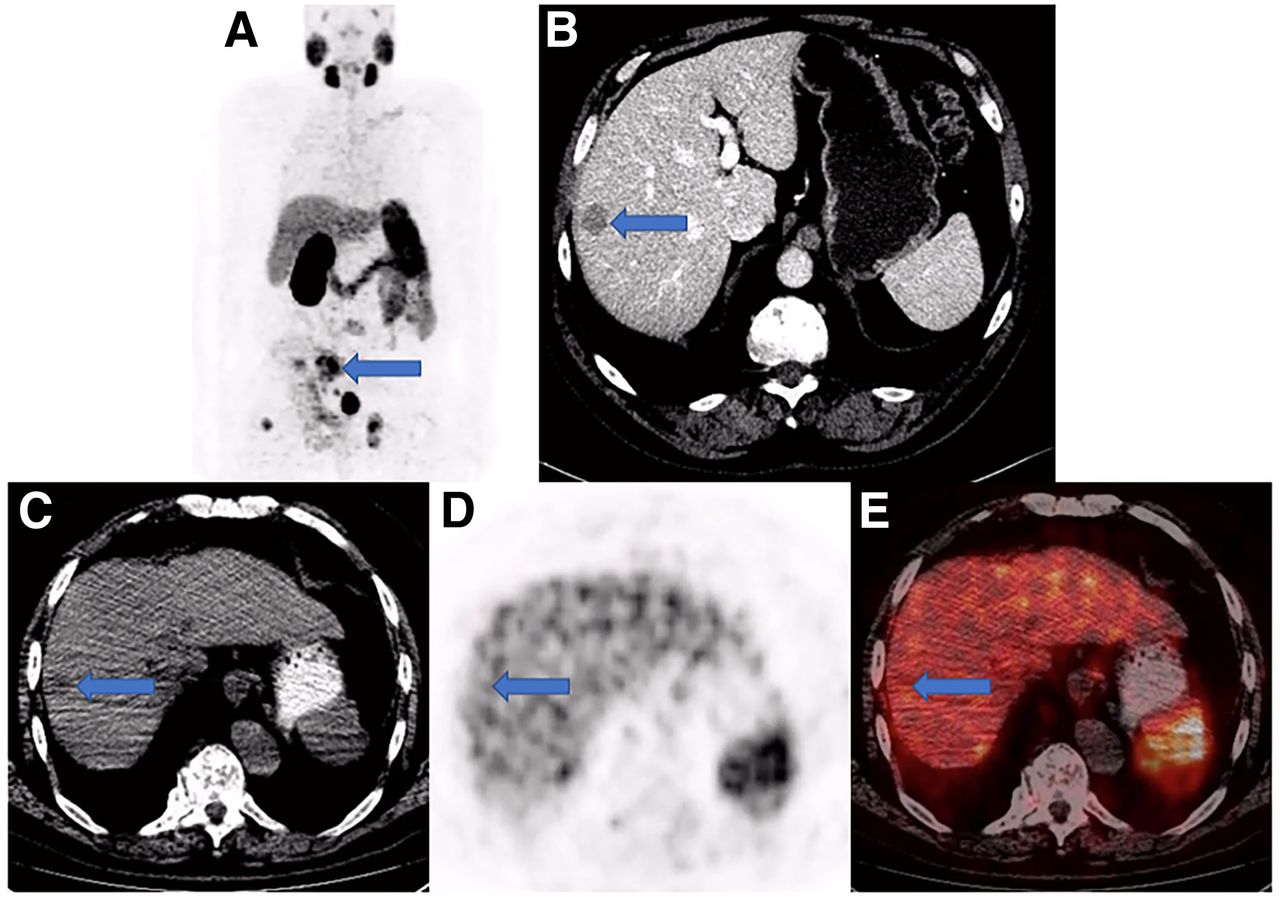
Example of patient who would have been excluded by imaging selection criteria used in VISION trial. (A) Anterior maximum-intensity projection from 68Ga-PSMA-11 PET/CT has readily evident PSMA-positive disease, such as in sacrum (arrow); thus, next step is to evaluate diagnostic CT for lesions that fulfill size criteria for possible exclusion. (B) On contrast-enhanced diagnostic CT, 1.8-cm metastasis is identified in right hepatic lobe (arrow). Transaxial low-dose CT (C), PET (D), and PET/CT (E) images show that metastasis (arrows) has activity similar to normal liver, is therefore PSMA-negative, and would result in exclusion. Level of uptake in hepatic metastasis was importantly confirmed in sagittal and coronal planes (not shown) in case of misregistration.
By synthesizing the knowledge of radiotherapeutic trials with prior experience in developing reading criteria for theranostics, novel imaging selection criteria saw their first use in the successful VISION trial. Future correlation with outcomes and advanced PSMA PET analyses are needed to further refine these selection criteria to optimize patient care and management decision algorithms (10,11).
DISCLOSURE
Phillip Kuo is an employee of Invicro. He is a consultant or speaker for Amgen, Eisai, Endocyte, GE Healthcare, Novartis, Invicro, Bayer, Chimerix, Fusion Pharma, and UroToday. He is a recipient of research grants from Blue Earth Diagnostics and GE Healthcare. Richard Messmann is an employee of Novartis and previously of Endocyte. Taylor Benson is an employee of Novartis and previously of Endocyte. Michael Groaning is an employee of Amgen and previously of Endocyte and Novartis. No other potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENT
We thank the entire Endocyte and Novartis teams for their contributions to the VISION trial.
Footnotes
Published online Jan. 27, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 7, 2021.
- Revision received January 20, 2022.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Real-World Experience with 177Lu-PSMA-617 Radioligand Therapy After Food and Drug Administration Approval
- Survey of Clinical Protocols for the Use of 177Lu-PSMA-617 in the United States
- SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-PSMA-617 Radionuclide Therapy
- A VISION Substudy of Reader Agreement on 68Ga-PSMA-11 PET/CT Scan Interpretation to Determine Patient Eligibility for 177Lu-PSMA-617 Radioligand Therapy
- A VISION Substudy of Reader Agreement on 68Ga-PSMA-11 PET/CT Scan Interpretation to Determine Patient Eligibility for 177Lu-PSMA-617 Radioligand Therapy
- SNMMI Consensus Statement on Patient Selection and Appropriate Use of 177Lu-PSMA-617 Radionuclide Therapy
- A VISION Substudy of Reader Agreement on 68Ga-PSMA-11 PET/CT Scan Interpretation to Determine Patient Eligibility for 177Lu-PSMA-617 Radioligand Therapy
- Is 18F-FDG PET Needed to Assess 177Lu-PSMA Therapy Eligibility? A VISION-like, Single-Center Analysis
- Clinical Trials of Prostate-Specific Membrane Antigen Radiopharmaceutical Therapy
- Eligibility for 177Lu-PSMA Therapy Depends on the Choice of Companion Diagnostic Tracer: A Comparison of 68Ga-PSMA-11 and 99mTc-MIP-1404 in Metastatic Castration-Resistant Prostate Cancer
- Reply: What Does an Imaging "Selection" Claim Actually Mean?
- What Does an Imaging "Selection" Claim Actually Mean?