


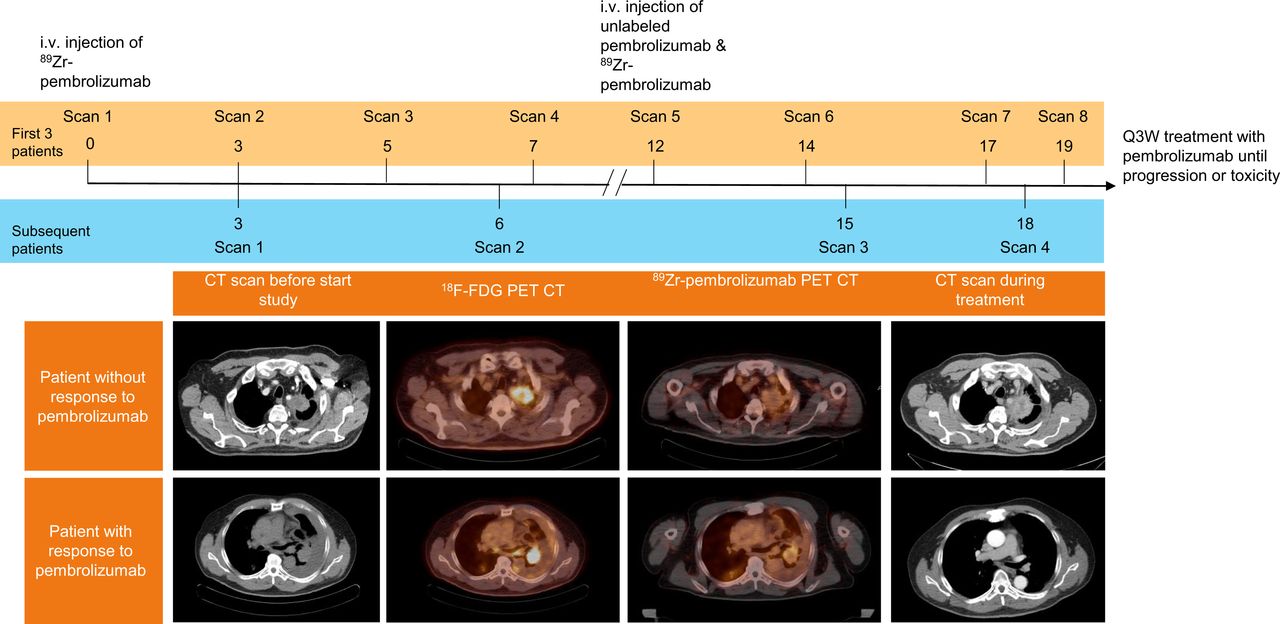
Visual Abstract
Abstract
The tumor programmed death ligand 1 (PD-L1) proportion score is the current method for selecting non–small cell lung cancer (NSCLC) patients for single-agent treatment with pembrolizumab, a programmed cell death 1 (PD-1) monoclonal antibody. However, not all patients respond to therapy. Better understanding of in vivo drug behavior may help in the selection of patients who will benefit the most. Methods: NSCLC patients eligible for pembrolizumab monotherapy as first- or later-line therapy were enrolled. Patients received 2 injections of 89Zr-pembrolizumab, 1 without a preceding dose of pembrolizumab and 1 with a preceding dose of 200 mg of pembrolizumab, directly before tracer injection. Up to 4 PET/CT scans were obtained after tracer injection. After imaging acquisition, patients were treated with 200 mg of pembrolizumab every 3 wk. Tumor uptake and tracer biodistribution were visually assessed and quantified as the SUV. Tumor tracer uptake was correlated with PD-1 and PD-L1 expression and response to pembrolizumab treatment. Results: Twelve NSCLC patients were included. One patient experienced grade 3 myalgia after tracer injection. 89Zr-pembrolizumab was observed in the blood pool, liver, and spleen. Tracer uptake was visualized in 47.2% of 72 tumor lesions measuring ΒΧΡ20 mm in the long-axis diameter, and substantial uptake heterogeneity was observed within and between patients. Uptake was higher in patients with a response to pembrolizumab treatment (n = 3) than in patients without a response (n = 9), although this finding was not statistically significant (median SUVpeak, 11.4 vs. 5.7; P = 0.066). No significant correlations were found with PD-L1 or PD-1 immunohistochemistry. Conclusion: 89Zr-pembrolizumab injection was safe, with only 1 grade 3 adverse event—possibly immune-related—in 12 patients. 89Zr-pembrolizumab tumor uptake was higher in patients with a response to pembrolizumab treatment but did not correlate with PD-L1 or PD-1 immunohistochemistry.
Immune checkpoint inhibitors have changed the treatment paradigm of advanced non–small cell lung cancer (NSCLC). However, identifying individual patients who will benefit from immune checkpoint inhibitors remains challenging. Better selection of patients will likely lead to higher response rates, fewer unnecessary toxicities, and reduced costs. The current method of selecting patients for single-agent treatment with pembrolizumab, a programmed cell death 1 (PD-1) monoclonal antibody, consists of scoring tumor programmed death ligand 1 (PD-L1) expression using immunohistochemistry. Although pembrolizumab monotherapy has been approved for the first- and second-line treatment of NSCLC patients with a PD-L1 tumor proportion score (TPS) of 1% or higher, only 28% of patients show a response to treatment, according to RECIST 1.1; the highest response rates were 40%–45% for patients with a TPS of greater than or equal to 50% (1–4). At the same time, approximately 10% of patients without tumor PD-L1 expression respond to treatment (1,5).
PET with radiolabeled antibodies visualizes and quantifies pharmacokinetics in vivo, which may help in the understanding of antibody behavior in blood and tissues (6). Previous research on NSCLC patients with radiolabeled immune checkpoint inhibitors revealed intra- and interpatient heterogeneity of tumor uptake for 89Zr-nivolumab (PD-1) and 89Zr-atezolizumab (PD-L1) (7,8). 89Zr-atezolizumab uptake strongly correlated with a response, whereas 89Zr-nivolumab uptake correlated with a lesional response but not an overall response. To our knowledge, studies of people with 89Zr-labeled pembrolizumab have not been performed yet. Preclinical studies with 64Cu- and 89Zr-labeled pembrolizumab in mice and rats showed uptake in the spleen and liver and specific targeting of PD-1 (9,10). Although nivolumab and pembrolizumab are PD-1--blocking antibodies with structural similarities, they bind to different areas on the PD-1 receptor (11–13). In this feasibility study, we aimed to investigate whether the administration of 89Zr-pembrolizumab is safe, to assess the biodistribution of 89Zr-pembrolizumab, and to correlate the tracer uptake with PD-1 and PD-L1 immunohistochemistry and the response to pembrolizumab treatment.
MATERIALS AND METHODS
Patients
This study was conducted according to the Declaration of Helsinki. The institutional review board (Medical Ethics Committee of the Amsterdam University Medical Centers [VU University Medical Center], Amsterdam, The Netherlands) approved this study, and all subjects signed a written informed consent form. The trial was registered at www.clinicaltrials.gov (Clinical Trials Identifier: NCT03065764). Twelve patients with advanced NSCLC eligible for pembrolizumab treatment were included in this multicenter trial.
Tumor Biopsies
Histologic tumor biopsies were obtained before the first 89Zr-pembrolizumab injection and after the last line of systemic therapy, in case patients received prior therapy. Tumor tissue sections were stained with hematoxylin and eosin (H&E), PD-L1 (Dako PD-L1 IHC 22C3 pharmDx), and PD-1 (Cell Marque Corp. Clone NAT105 antibody). An experienced thoracic pathologist who was unaware of clinical information evaluated the slides. PD-L1 and PD-1 expression was measured as total (both tumor and immune cells) PD-L1 and PD-1 expression. In addition, tumor PD-L1 expression was scored as the percentage of tumor cells showing positive staining in the sample. PD-L1 was scored according to 22C3 scoring guidelines (14). PD-L1 and PD-1 were also scored according to the SP142 scoring system (IC0, IC1, IC2, IC3) (15), but still with the 22C3 antibody.
89Zr-Pembrolizumab
89Zr-pembrolizumab was produced in compliance with current good manufacturing practices at Amsterdam University Medical Centers [VU University Medical Center], Amsterdam, The Netherlands) according to validated procedures (16–18). Pembrolizumab was labeled with 89Zr in an inert way to ensure that 89Zr-pembrolizumab kinetics fully resembled the kinetics of unlabeled pembrolizumab (19,20). 89Zr-pembrolizumab was produced as previously described with slight modifications (19). The production process is described in detail in the supplemental materials (supplemental materials are available at http://jnm.snmjournals.org).
Study Design
The study protocol consisted of 2 imaging series per patient, 1 without and 1 with a predose of unlabeled pembrolizumab (Supplemental Fig. 1). 89Zr-pembrolizumab (37 MBq ± 10%; 2 mg of pembrolizumab) was intravenously injected on day 0. Static PET/CT scans from the skull vertex to the midthighs were performed 1 h and 3, 5, and 7 d after injection for the first 3 patients, whereas all other patients were scanned on days 3 and 6 after injection. On day 12, patients received an infusion of 200 mg of unlabeled pembrolizumab, followed within 2 h by a 89Zr-pembrolizumab injection, to maximize the chance of representing therapeutic tumor targeting. A diagnostic CT scan of the thorax and upper abdomen and brain MRI were performed before the start of treatment. Pembrolizumab (200-mg flat dose) was administered every 3 wk until disease progression, unacceptable toxicity, or withdrawal of consent. Response assessment was performed with a diagnostic contrast-enhanced CT scan of the thorax and upper abdomen, with or without brain MRI (the latter only in case of pretreatment brain metastases), every 9 wk during treatment or more frequently if clinically indicated. RECIST 1.1 was used for assessment (21). Durable clinical benefit (DCB) was defined as a partial response or stable disease for greater than or equal to 6 mo.
PET Acquisitions
PET acquisitions were performed using a European Association of Nuclear Medicine Research Ltd.–calibrated Philips Ingenuity TF, Philips Big Bore, or Philips TF TOF PET/CT scanner (Philips Healthcare) at 10 min/bed position over the area containing the primary tumor and 5 min over the remaining bed positions. After this PET scan, a low-dose CT scan (50 mAs, 120 kV) was acquired for anatomic correlation and attenuation correction. Whole-body data were corrected for dead time, decay, scatter, and randoms and reconstructed with a matrix size of 144 × 144, 4-mm3 voxels, and a time-of-flight iterative reconstruction method. The transaxial spatial resolution was approximately 5 mm full width at half maximum in the center of the field of view.
PET/CT Analyses
Reconstructed images were transferred to offline workstations for further analysis. Tumor accumulation was assessed by an experienced nuclear physician and described as focal or diffuse uptake exceeding the local background and incompatible with physiologic uptake. Volumes of interest (VOIs) were manually delineated on each scan using the Accurate tool (22). Liver, spleen, brain, lungs, and kidneys were manually delineated on each scan using the low-dose CT scan as an anatomic reference (23). Fixed VOIs were placed in the descending aorta to measure blood-pool activity and in the lumbar vertebrae to estimate the bone marrow activity concentration. Tracer uptake in all delineated VOIs was quantified semiquantitatively as the SUV. From each VOI, we derived the mean and peak activity concentrations (Bq/cm3), normalized for body weight. SUVmean is used to report organ tracer uptake, and SUVpeak is used for tumor lesions (24). To compare tracer uptake between imaging series 1 and 2, the percentage injected dose per gram (%ID/g) of tissue was calculated. To avoid partial-volume effects, only results for tumor lesions exceeding 20 mm in the long-axis diameter are reported.
Blood Samples
Blood samples for assessing 89Zr-pembrolizumab concentrations were obtained at 5, 30, 60, and 120 min after injection for the first 3 patients. For the other patients, blood samples were drawn at 5 and 30 min after injection. Plasma and whole-blood concentrations were assessed by radioactivity measurements in a cross-calibrated γ-counter (Wallac Wizard 1480; PerkinElmer Inc.). The plasma activity concentration was calculated as the %ID/g.
Adverse Events
Adverse events were recorded from the initial signing of the informed consent form to the second full dose of pembrolizumab. The National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0 were used (25).
Statistical Analysis
Statistical analysis was performed using SPSS statistics for Windows version 26.0 (IBM SPSS). The median SUVpeak of all delineated lesions (long-axis diameter of ≥20 mm) per patient were calculated and used to compare the median values of patients with a DCB and patients without a DCB. Because of the small patient numbers, PD-1 immunohistochemistry was dichotomized as “PD-1 low” (IC0 and IC1) and “PD-1 high” (IC2 and IC3). A Mann–Whitney–Wilcoxon rank sum test was performed to evaluate differences in SUV for a response and immunohistochemistry. Progression-free survival (PFS) was summarized using Kaplan–Meier plots. PFS was defined from the date the patient received the first pembrolizumab cycle to the date of radiologic progression or death (whichever occurred first). The median SUVpeak of the full cohort was used to stratify high uptake versus low uptake, and the log-rank test was used to compare the groups. Correlations between SUVpeak of tumor lesions on different scan days were calculated using the Spearman rank correlation coefficient. The Wilcoxon signed rank test and the Friedman test were performed for paired data (multiple groups). P values of less than 0.05 were considered statistically significant.
RESULTS
Patients
Twelve patients, 5 chemotherapy naive and 7 with progression after first- or second-line treatment, were enrolled (Supplemental Table 1). All patients had histopathologically confirmed lung adenocarcinoma. Patients who were chemotherapy naive had higher PD-1 and PD-L1 expression rates than patients who received prior chemotherapy. Eight patients completed the full imaging series. For patients 2 and 3, scans were not performed at days 12 and 14, respectively, because of logistical problems. Patient 6 did not receive the second injection or treatment because of a large brain metastasis that required immediate treatment, and patient 7 refused to undergo the last PET/CT scan because of dyspnea. For patient 12, only a scan of the thorax could be obtained at days 6, 15, and 18 because of severe myalgia (grade III).
Safety
The most frequently reported adverse events were fatigue, anorexia, and dyspnea (Supplemental Table 2), most of which were disease related. In 1 patient, grade III anemia was observed, but the onset was before tracer injection. One patient experienced grade III myalgia after the first 89Zr-pembrolizumab injection. This patient discontinued treatment after the first pembrolizumab cycle because of the myalgia and had progressive disease within 6 mo after the start of treatment.
Pharmacokinetics
To explore whether microdosing of the tracer (2 mg) could be used to image tumor uptake, we compared the %ID/g in plasma, in organs, and in tumor lesions between the first imaging acquisition (part 1) and the second imaging acquisition (part 2). Plasma clearance was slower for part 2 than for part 1 (Supplemental Fig. 2). Because of limited data, no statistical tests were performed. The concentration of pembrolizumab in the spleen was lower in part 2, suggesting that the spleen served as a “sink” (Supplemental Fig. 3).
For the other organs, no differences were observed in %ID/g between part 1 and part 2 for the first 3 patients (Supplemental Fig. 2). Remarkably, not all tumor lesions that were identified in part 1 could be assessed in part 2 (Supplemental Table 3). Nineteen tumor lesions could be identified in 10 patients at multiple time points in part 1, and 10 lesions were visible at multiple time points in part 2 (Supplemental Fig. 3). In 2 patients, %ID/g in the primary tumor was higher in part 2 than in part 1 (Supplemental Fig. 3). In the following paragraphs, only data for part 1 are shown.
Biodistribution of 89Zr-Pembrolizumab
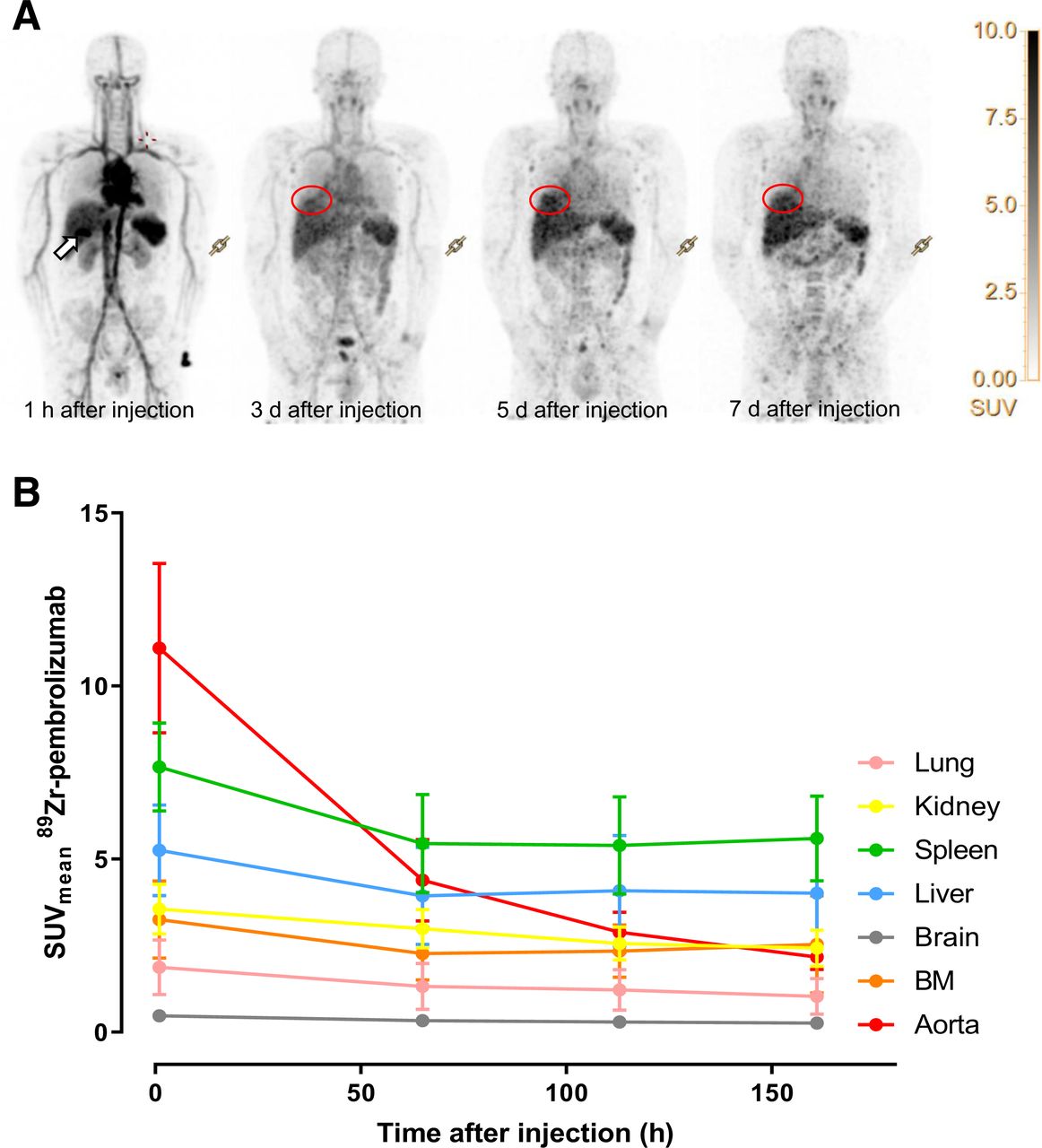
On the first PET/CT scan (performed 1 h after injection), 89Zr-pembrolizumab uptake was observed in the blood pool, liver, spleen, and kidneys (Fig. 1A). In 2 of 3 patients (66.6%), the gallbladder was also visualized (Fig. 1A). Circulating 89Zr-pembrolizumab in the blood pool was highest (SUVmean, 11.5 ± 1.4) at 1 h after injection and decreased over time (SUVmean, 4.6 ± 1.2, 3.0 ± 0.5, and 2.3 ± 0.6 on days 3, 5, and 7 after injection, respectively) (Figs. 1A and 1B). Uptake was high in the liver and spleen (SUVmean, 3.9 ± 1.4 and 5.5 ± 1.4, respectively, on day 3 after injection) (Figs. 1A and 1B) and remained stable over time (liver: SUVmean, 4.1 ± 1.6 on day 5 after injection and 4.0 ± 1.6 on day 7 after injection; spleen: SUVmean, 5.4 ± 1.4 on day 5 after injection and 5.6 ± 1.2 on day 7 after injection). Intestinal uptake was variable (Fig. 1A), and low uptake was seen in the kidneys, bone marrow, non–tumor-bearing lung tissue, and brain (SUVmean, 3.0 ± 0.6, 2.4 ± 0.5, 1.3 ± 0.7, and 0.4 ± 0.1, respectively, on day 3). In 8 of 12 patients, nonmalignant lymph nodes or adrenal glands showed low tracer uptake (examples are shown in Supplemental Fig. 4). In patient 1, an axillary lymph node (not suggestive of malignancy on an 18F-FDG PET/CT scan) that showed low tracer uptake was biopsied. Histopathologic examination showed a high density of PD-1–positive lymphocytes in the secondary lymphoid follicles and no malignant cells. The adrenal glands of patient 3 were slightly enlarged at baseline but were not suggestive of metastases on the 18F-FDG PET/CT scan, and the adrenal glands remained unchanged during follow-up CT scans.

Biodistribution of 89Zr-pembrolizumab. (A) Maximum-intensity-projection image of patient 1. White arrow indicates gallbladder. Red circle indicates primary tumor. (B) Tracer uptake per time point, measured as mean SUVmean for first 3 patients at 1.1 ± 0.3, 65.8 ± 0.3, 113.2 ± 0.7, and 161.4 ± 0.81 h after injection. BM = bone marrow.
Tumor Uptake
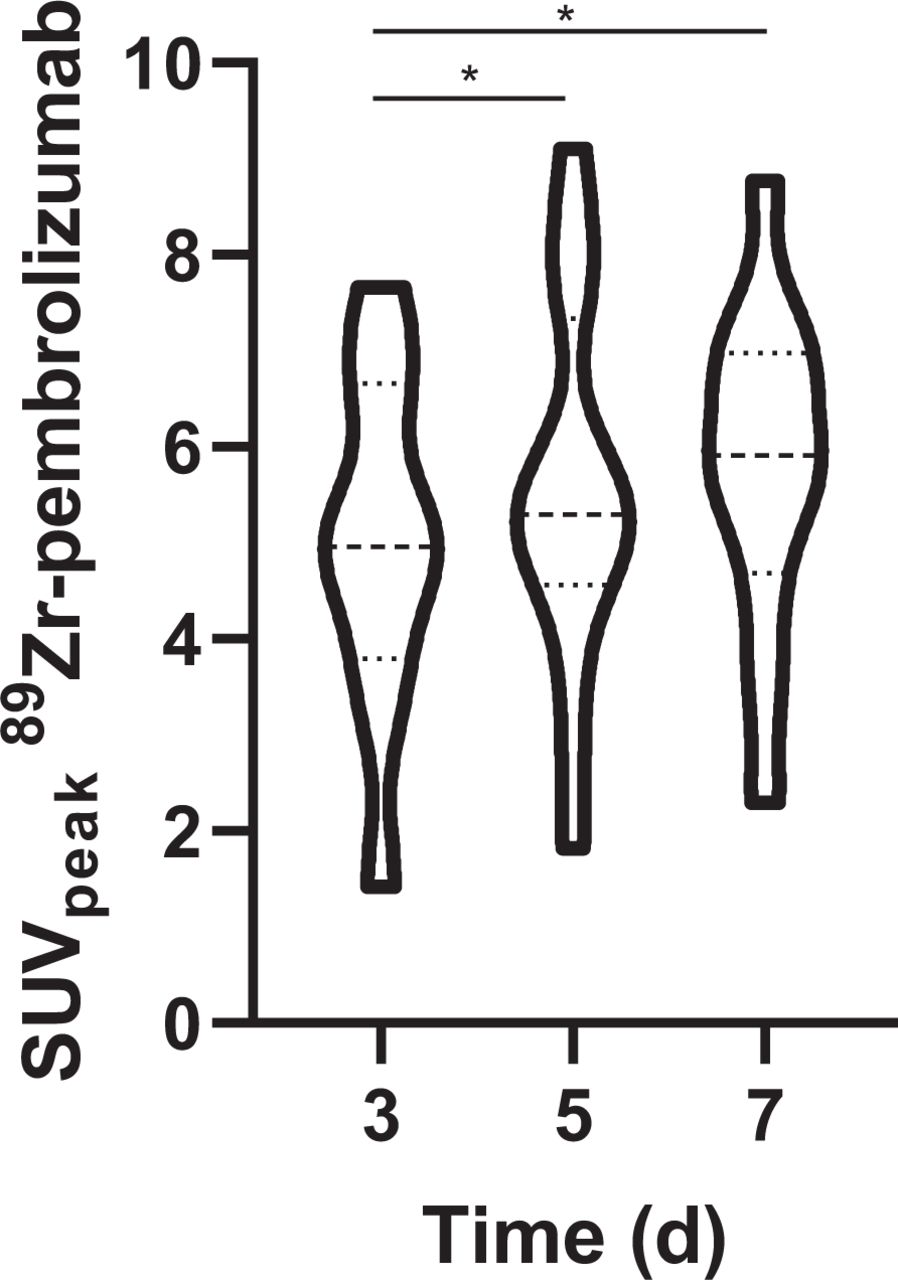
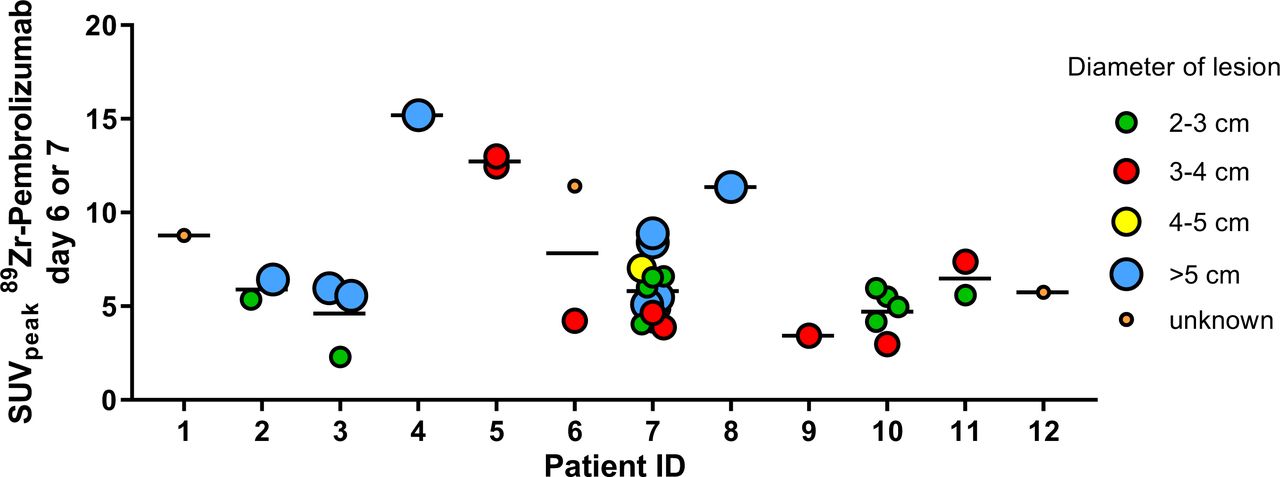
Overall, a total of 216 lesions from 12 patients were delineated on the pretreatment diagnostic CT scan (Table 1). Of these lesions, 140 (64.8%) had a diameter of less than 20 mm, 4 were difficult to measure because of atelectasis, and 72 (33%) had a diameter of greater than or equal to 20 mm. Sixty-two lesions (28.7%) were visible on PET/CT. Of the 140 lesions with a diameter of less than 20 mm, 26 (18.6%) were visible on PET/CT on day 6 or 7. Of the 72 lesions with a long-axis diameter of greater than or equal to 20 mm, 34 (47.2%) were visible. Two lesions were difficult to measure. In all patients, at least 1 malignant lesion showed tracer uptake (median, 4.5; range, 2–17 [per patient]). For the first 3 patients, the median SUVpeak of tumor lesions increased over time from 4.9 (interquartile range, 3.5–6.6) on day 3 to 5.2 (interquartile range, 4.0–6.8) on day 5 to 5.9 (interquartile range, 4.0–7.0) on day 7 after injection (Fig. 2). There was no significant increase between day 5 and day 7 after injection (P = 0.28). Intralesional tracer distribution was heterogeneous (Fig. 3), and uptake patterns were variable (Figs. 4A–4D).
Lesions on Diagnostic CT and 89Zr-Pembrolizumab PET
Median SUVpeak of all lesions for all patients.

89Zr-pembrolizumab tumor uptake for all patients per delineated tumor.
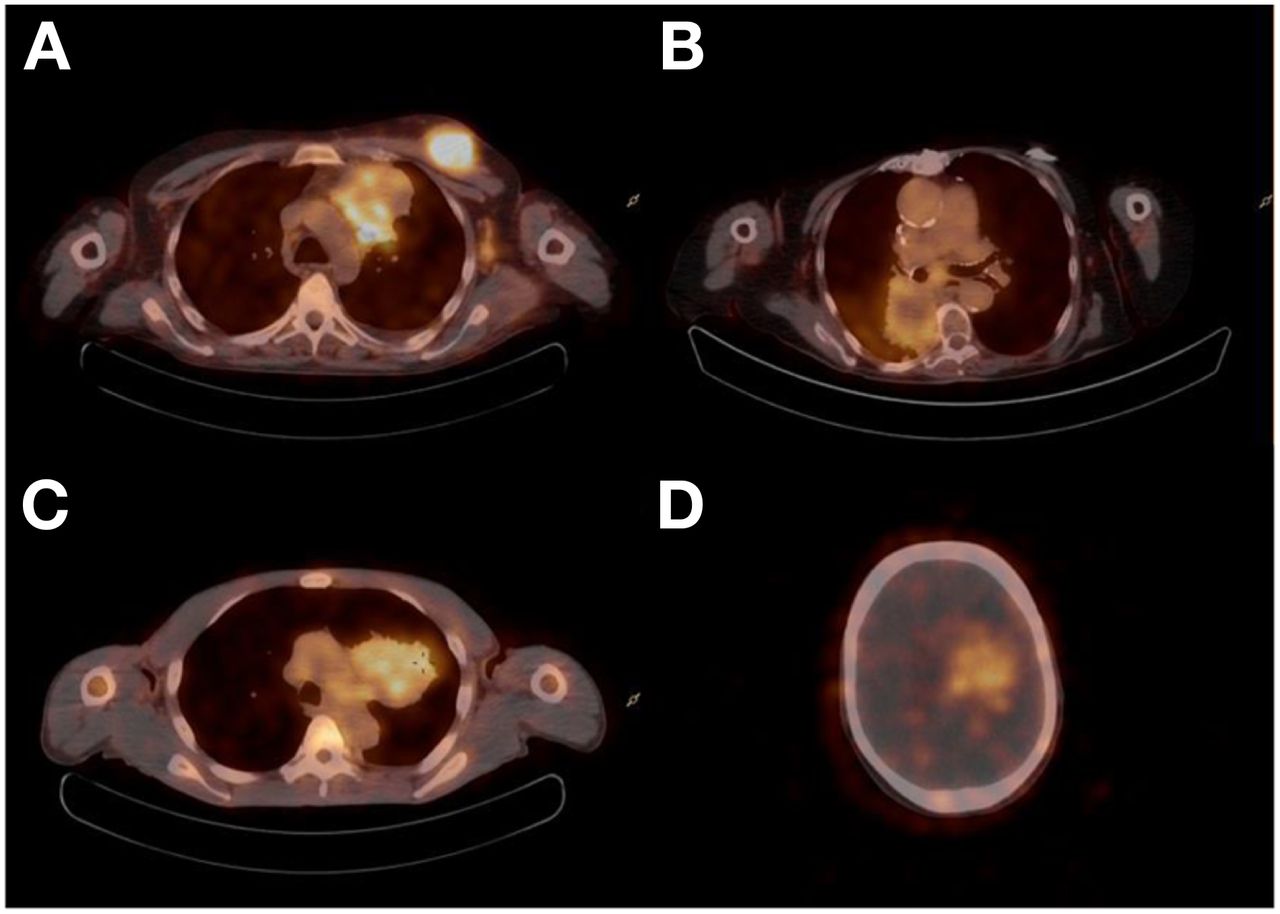
89Zr-pembrolizumab uptake patterns. (A) Heterogeneous uptake in paracardiac mass and homogeneous uptake in soft-tissue mass in left breast. (B) Rim uptake. (C) Heterogeneous uptake. (D) Uptake in brain metastasis.
Of 4 patients who had brain metastases (38 lesions in total), 3 had been treated with (stereotactic) radiotherapy before the start of the present study (18/38 lesions) (Supplemental Table 4). Increased tracer uptake was observed in 2 patients (3 metastases): 1 patient had received whole-brain radiotherapy 9 mo before PET imaging (1 visible brain metastasis; long-axis diameter, 33.1 mm) (Fig. 4D), and 1 patient had not been irradiated before (2 visible brain metastases; long-axis diameters, 31.9 and 19.3 mm).
Response
For response evaluation, we reported the SUVpeak on day 6 or 7 because tumor uptake was the highest and blood-pool activity was the lowest, thus offering the best tumor-to-background ratio.
Three patients had a DCB from pembrolizumab: 1 had a partial response according to RECIST 1.1, and 2 had stable disease. Patients with a DCB had a higher median tracer uptake, but this finding was not significant (median SUVpeak, 11.4 vs. 5.7; P = 0.066) (Fig. 5A). 89Zr-pembrolizumab uptake increased with the best response category according to RECIST 1.1 (P = 0.047) (Fig. 5B). No partial response was observed in lesions with negative PET results. Patients with an SUVpeak higher than the median (SUVpeak, 6.7) had a longer PFS (median PFS, 25.0 wk) than those with an SUVpeak lower than the median (median PFS, 7.0 wk), although this finding was not significant (P = 0.21) (Fig. 5C).

Relationship between tracer uptake and response. (A) Median tracer uptake of all lesions > 20 mm for responders and nonresponders. (B) Median tracer uptake per best RECIST response category. (C) Progression-free survival curve according to median SUVpeak (blue, above median SUVpeak of 6.7; orange, below median SUVpeak). p.i. = postinjection.
Immunohistochemistry
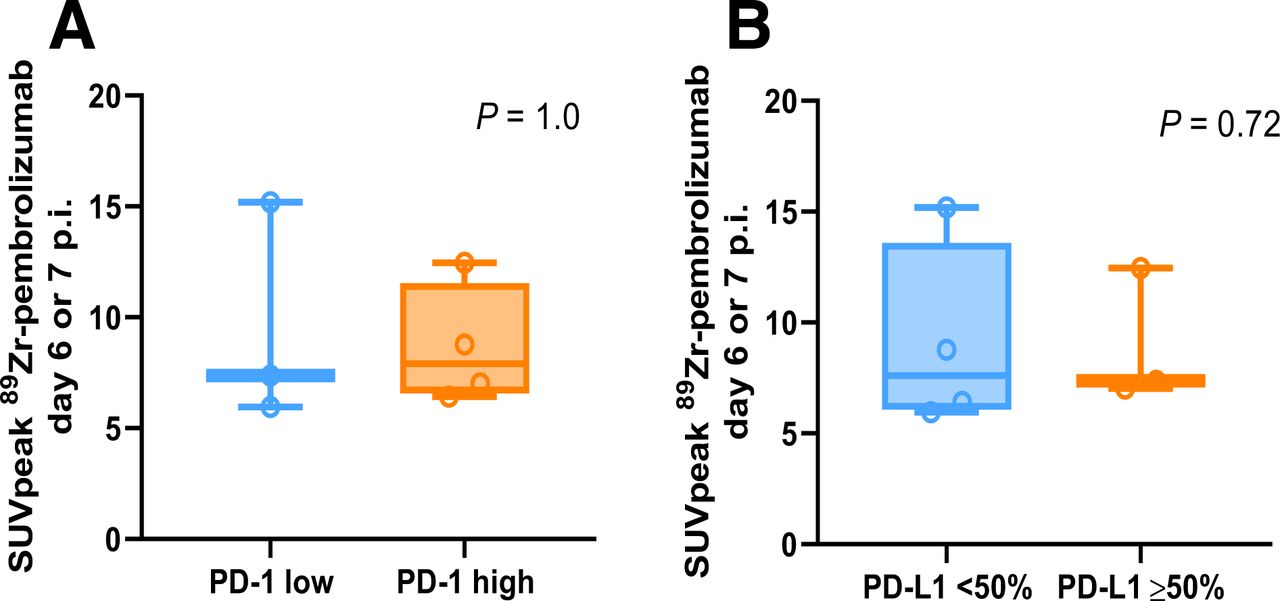
Not all biopsied lesions (n = 7/12) showed 89Zr-pembrolizumab uptake (Supplemental Table 5). PD-1 expression and tracer uptake were not correlated (the median SUVpeak were 7.9 for patients with high PD-1 expression and 7.4 for patients with low PD-1 expression; P = 1.0); neither were PD-L1 expression and tracer uptake (the median SUVpeak were 7.6 for patients with a TPS of <49% and 7.4 for patients with a TPS of ≥50%; P = 0.72) (Figs. 6A and 6B). Pretreatment PD-1 expression did not correlate with a response (P = 0.41), whereas pretreatment PD-L1 expression of greater than or equal to 50% did predict a response (P = 0.049).
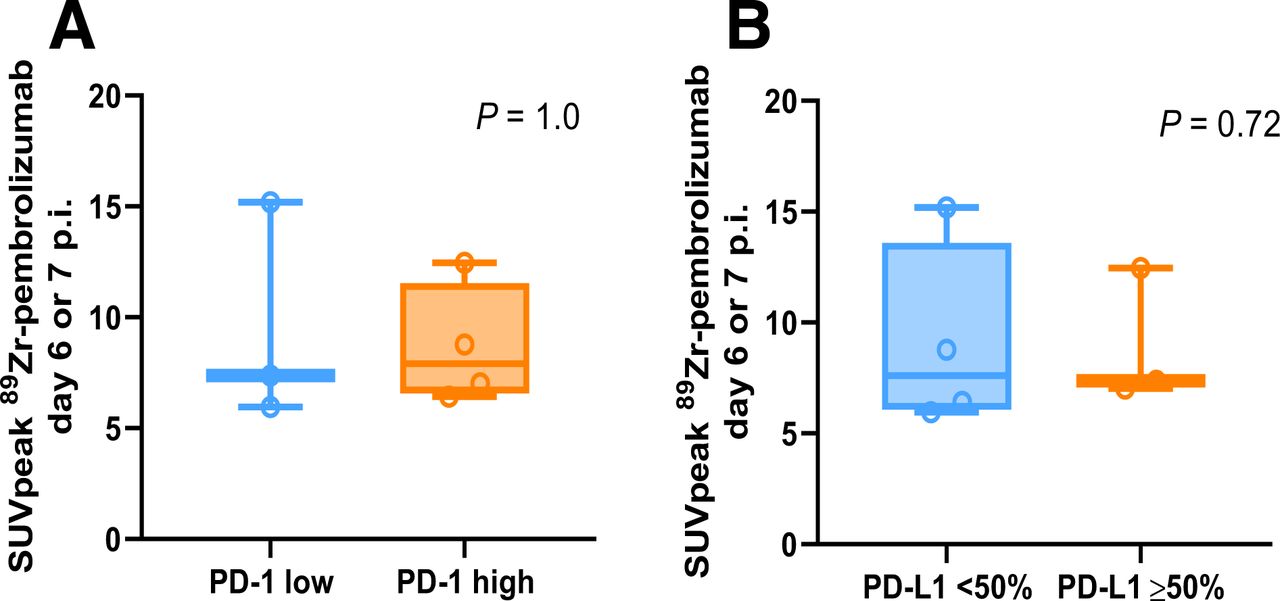
Relationship between tracer uptake and immunohistochemistry. (A) Correlation between SUVpeak and PD-1 expression of biopsied lesion. (B) Correlation between SUVpeak and PD-L1 expression of biopsied lesion. p.i. = postinjection.
DISCUSSION
This first-in-humans study of 89Zr-pembrolizumab shows that injection of 89Zr-pembrolizumab was well tolerated, with 1 possibly related adverse event. Tumor lesions could be visualized and quantified. For all patients, at least 1 tumor lesion showed tracer uptake after a single 89Zr-pembrolizumab injection. Tumor uptake was heterogeneous within and between patients, and only 47.2% of the lesions with a long-axis diameter of greater than or equal to 20 mm showed uptake on the 89Zr-pembrolizumab PET/CT scan.
All patients (except patient 6) underwent 2 imaging acquisitions, 1 without a predose of unlabeled pembrolizumab and 1 with a predose. Plasma clearance was slower when the predose was used. We observed lower tracer uptake in the spleen in part 2 than in part 1, suggesting that the predose saturated the PD-1 receptors in the spleen. In part 2 (with coinjection of a predose), only 10 lesions could be delineated in the first 3 patients, whereas 19 lesions could be delineated in these patients in part 1. We assume that a predose of 200 mg (flat dose of pembrolizumab) occupied most available PD-1 receptors, causing a loss of signal. Recently, a flow cytometry study in patients treated with pembrolizumab showed receptor occupancy on peripheral mononuclear blood cells at the end of the first infusion of 88%–100%, depending on cell type (26). Unfortunately, because of our limited data, we cannot determine an “optimal predose” of unlabeled pembrolizumab.
The biodistribution of 89Zr-pembrolizumab was comparable to that observed in previous NSCLC studies with 89Zr-labeled immune checkpoint inhibitors. High uptake was seen in the liver (likely because of tracer catabolism), the spleen (likely because of binding to PD-1 receptors on lymphocytes and dendritic cells, abundantly present in the spleen), and nonmalignant lymph nodes (7,8). PD-1 is expressed on a variety of immune cells, including activated and exhausted CD8+ T cells, B cells, myeloid dendritic cells, and monocytes; in fact, most patients showed 89Zr-pembrolizumab uptake in nonmalignant lymph nodes (27). Recent preclinical imaging studies with 89Zr-pembrolizumab in mice and monkeys also reported high uptake in lymphoid tissues (28,29). Variable uptake was observed in the intestines, probably because of excretion. In none of the patients included in the present study was colitis observed during pembrolizumab treatment. Low uptake was observed in the kidneys, adrenal glands, bone marrow, lungs, and central nervous system, suggesting that this tracer has a beneficial profile for imaging lung cancer patients. In the present study, we observed tracer uptake in some brain metastases. Since most brain metastases were pretreated with radiotherapy and small in size (<20 mm), these factors could have contributed to the absence of tracer accumulation in several of these lesions.
Tracer uptake in nonmalignant lymph nodes is regarded as specific uptake. Lymph nodes are known for their role in the immune defense to pathogens, and tumor-draining lymph nodes are needed to engage an optimal antitumor immune response (30,31). Nonmalignant lymph nodes are known to contain PD-1–expressing immune cells (27). One lymph node not suggestive of malignant involvement was biopsied because it showed substantial 89Zr-pembrolizumab uptake, and immunohistochemistry did indeed show high PD-1 expression in the follicles. Whether PD-1 expression in lymph nodes is necessary to obtain a response remains uncertain. In 1 patient, 89Zr-pembrolizumab uptake exceeded the local background in benign adrenal glands. Lymphocytic infiltration of the adrenal gland has been described (32).
89Zr-pembrolizumab uptake was higher in responding patients than in nonresponding patients, although this finding was not significant. Tumor uptake of 89Zr-pembrolizumab increased with the best tumor response category according to RECIST 1.1. Similar findings were observed for anti–PD-L1 89Zr-atezolizumab PET/CT (8). We did observe that negative lesions on 89Zr-pembrolizumab PET did not have a response to treatment, supporting our hypothesis that there is a link between uptake and response.
We were not able to find a correlation between PD-1 expression and 89Zr-pembrolizumab uptake. Heterogeneity between surgical specimens and biopsies is well known and could account for the difference in tracer uptake and PD-1 expression in a small tumor biopsy (33,34). This possibility is further supported by the observation that 89Zr-pembrolizumab tracer uptake was heterogeneous both within and between tumor lesions.
CONCLUSION
The present study shows that 89Zr-pembrolizumab PET/CT imaging in patients with NSCLC is safe and feasible. In this limited dataset, we found that 89Zr-pembrolizumab tracer uptake showed a nonsignificant correlation with a response to pembrolizumab treatment. Further research is needed to investigate the value of 89Zr-pembrolizumab as a stand-alone biomarker or as adjunct information for tumor PD-L1 expression determined by immunohistochemistry.
DISCLOSURE
We received a research grant for the implementation of this study from Merck Sharpe & Dohme (MSD). MSD was not involved in the study design, data collection, analysis and interpretation of the data, or the writing of this report. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: The aims of this study were to investigate whether the administration of 89Zr-pembrolizumab was safe, to assess the biodistribution of 89Zr-pembrolizumab, and to correlate the tracer uptake with PD-1 and PD-L1 immunohistochemistry and response to pembrolizumab treatment.
PERTINENT FINDINGS: In this feasibility study, we observed that 89Zr-pembrolizumab uptake was safe and that it was higher in patients with a response (SUVpeak, 11.4) than in patients without a response (SUVpeak, 5.7), although this finding was not statistically significant.
IMPLICATIONS FOR PATIENT CARE: Further research is needed to investigate whether 89Zr-pembrolizumab can be used as a biomarker.
Footnotes
Published online July 16, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
References
- Received for publication January 11, 2021.
- Revision received May 20, 2021.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}