


Abstract
Aortic stenosis is a common condition associated with major morbidity, mortality, and health-care costs. Nevertheless, we currently lack any effective medical therapies that can treat or prevent disease development or progression. Modern advances in echocardiography and CT have helped improve the assessment of aortic stenosis severity and monitoring of disease progression, whereas cardiac MRI informs on myocardial health and the development of fibrosis. In a series of recent studies, 18F-NaF PET/CT has been shown to assess valvular disease activity and progression, providing mechanistic insights that can inform potential novel therapeutic approaches. This review will examine the latest advances in the imaging of aortic stenosis and bioprosthetic valve degeneration and explore how these techniques can assist patient management and potentially accelerate novel therapeutic developments.
- aortic stenosis
- CT calcium scoring
- CT-AVC
- coronary CT angiography
- microcalcification
- 18F-sodium fluoride PET/CT
Aortic stenosis is the commonest form of valve disease in the Western world and is associated with major morbidity, mortality, and health-care costs. The number of aortic valve replacements performed in the United States and Europe has risen exponentially (1), and with an increasingly elderly population, the prevalence of aortic stenosis is likely to double over the next 20 years (2). To improve patient care and outcomes, we need a better understanding of the underlying pathophysiology. Aortic stenosis is a disease of the valve and the myocardium characterized by progressive valve narrowing and left ventricular remodeling (3). Technologic advances in cardiovascular imaging now allow us to image both the valve and the myocardium in unprecedented detail. Echocardiography and cardiac MRI offer a detailed investigation of the health of the myocardium, as well as aortic valve structure and function. Both approaches can identify abnormalities in cardiac function, whereas cardiac MRI allows imaging of the myocardial fibrosis associated with aortic stenosis. The presence of such scarring can inform whether the ventricle is starting to decompensate in the face of the increased pressure afterload and potentially optimize the timing of aortic valve replacement.
Calcification remains one of the central pathologic processes driving aortic stenosis progression and therefore a key imaging target (4). CT calcium scoring can accurately quantify the calcium burden of the valve, providing a novel assessment of aortic stenosis severity to complement the latest advances in echocardiography. 18F-NaF PET/CT allows assessment of calcification activity in the valve, providing novel insight into the underlying pathology, identifying new treatment targets, and providing a novel biomarker by which to test their efficacy. 18F-NaF PET also has an exciting potential clinical role in the assessment and prediction of bioprosthetic valve degeneration. Indeed, with the development of multiple novel PET radiotracers targeting inflammation, fibrosis, and thrombosis, molecular PET imaging holds major promise in transforming our understanding of aortic valve disease both before and after intervention. This review will focus mainly on addressing the key concepts around the assessment of the valve in patients with aortic stenosis.
CT ANGIOGRAPHY FOR VALVULAR CALCIFICATION AND FIBROSIS
The initiation phase of aortic stenosis development involves mechanical injury leading to an inflammatory response within the valve leaflets, followed by the propagation phase, in which progressive valve fibrosis and calcification promote worsening valvular stenosis (5). Echocardiography remains the first-line imaging assessment for aortic stenosis, providing gold standard hemodynamic assessment of aortic stenosis severity as well as aortic valve morphology (tricuspid vs. bicuspid) and left ventricular function (6). However, a key limitation of echocardiography is that assessment of disease severity is discordant in a quarter to a third of cases, leading to uncertainty about true disease severity (7). Recently, multidetector-CT aortic valve calcium scoring has emerged as an alternative flow-independent marker of aortic stenosis severity to help resolve this clinical conundrum (4).
Electrocardiography-gated unenhanced CT provides a detailed, reproducible, and accurate assessment of the calcific burden in the aortic valve, using the same imaging and analysis protocols as are used for coronary calcium scoring (Fig. 1) (8). However, until recently, we lacked appropriate thresholds that might differentiate patients with and without severe aortic stenosis, thereby limiting its utility (9). The appreciation that men and women require different amounts of calcium to develop severe stenosis led to the identification of sex-specific thresholds (≥2,000 arbitrary units [AU] or ≥480 AU/cm2 for men and ≥1,200 AU or ≥290 AU/cm2 for women). These thresholds provide excellent and robust diagnostic accuracy for the presence of severe disease (4), which has been validated across large multicenter international datasets (9,10). On this basis, the recent European Society of Cardiology, American College of Cardiology, and American Heart Association guidelines have suggested the use of CT for the assessment of patients with discordant echocardiographic measurements (11,12).

role of CT calcium scoring, contrast-enhanced CT, and 18F-NaF PET/CT in evaluation of aortic stenosis. CT aortic valve calcium score can reliably quantify aortic valve calcification, with sex-specific thresholds (≥2,000 AU or ≥480 AU/cm2 for men and ≥1,200 AU or ≥290 AU/cm2 for women) being sensitive, specific, and accurate for presence of severe disease. Contrast-enhanced CT allows accurate visualization of aortic valve anatomy and quantification of fibrocalcific volume in young patients and patients with bicuspid aortic valve. 18F-NaF PET allows quantification of disease activity, which is predictive of future disease progression and can be utilized as endpoint in mechanistic and medical therapy studies. AS = aortic stenosis; CT-AVC = CT aortic valve calcium; TAVI = transcatheter aortic valve implantation.
The aortic valve calcium burden quantified by CT is a powerful predictor of aortic stenosis progression and of the development of clinical events, such as aortic valve replacement and death (13). Clavel et al. showed that severe aortic valve calcification was an independent predictor of overall mortality (13) and outperformed standard echocardiographic measures of disease severity, signifying that CT can provide information complementary to that obtained during routine clinical care. Pawade et al. demonstrated similar results for aortic valve replacement or death, an effect that persisted in the patients with discordant echocardiographic findings in whom this technique is most likely to be used (4).
Although CT aortic valve calcium scoring can reliably quantify calcification, it lacks the ability to quantify fibrosis, which is an important component of aortic stenosis, particularly in young women (14). Development of dedicated stand-alone software has allowed accurate quantification of the calcific leaflet volume and combined fibrocalcific leaflet volume from contrast-enhanced CT images (15,16). In a recent study, Cartlidge et al. showed that the calcified leaflet volume and combined fibrocalcific leaflet volume correlated well with hemodynamic assessments of aortic stenosis severity on echocardiography, as well as with the unenhanced-CT aortic valve calcium score (15). The investigators showed that the addition of the fibrocalcific leaflet volume to the calcific leaflet volume particularly strengthened the correlation with echocardiography in female patients (15). In another recent study, Grodecki et al. recruited 447 patients with aortic stenosis awaiting transcatheter aortic valve implantation and 224 matched control subjects to quantify calcific and noncalcific volumes (16). They showed that the burden of calcification was higher among patients with typical high-gradient aortic stenosis, whereas the noncalcified burden was higher in the low-gradient, low-flow aortic stenosis group. Moreover, total tissue volume was the best predictor of severe aortic stenosis, followed by noncalcified tissue volume, and more importantly, adding noncalcified tissue volume to aortic valve calcium score added incremental value for the prediction of severe aortic stenosis. Finally, the noncalcified tissue volume was an independent predictor of a major adverse cardiovascular event 30 d after transcatheter aortic valve implantation (Fig. 1).
PET/CT
Modern hybrid PET/CT scanners provide detailed molecular information about the activity of any biologic process subject to the availability of a targeted PET radiotracer. They combine disease activity information from PET with precise anatomic information from CT. The impact of cardiac, respiratory, and gross patient movement on PET image quality has been a major obstacle to both coronary and aortic valve PET/CT imaging. These challenges have been the focus of several image optimization studies, leading to the design and use of novel designated software platforms and techniques that now allow the robust assessment of disease activity in the heart and more specifically within the aortic valve.
Originally, cardiac PET/CT scans did not account for cardiac motion. Initial attempts to reduce cardiac motion exploited PET counts acquired during the end-diastolic phase, when the heart is relatively still (between 50% and 75% of the R–R interval). These attempts led to reduced blurring from cardiac motion but increased noise because 75% of the counts were effectively disregarded (17). In a reproducibility study, Pawade et al. (17) recruited 15 patients with aortic stenosis who then underwent repeat 18F-NaF PET/CT scanning. They compared data acquired using the original nongated PET and unenhanced-CT approach with a modified approach that combined contrast-enhanced CT angiography and electrocardiogram-gated PET. They demonstrated that the modified technique allowed more accurate image coregistration, which allowed more precise localization of the tracer activity in the areas of peak mechanical stress, such as the leaflet tips and the commissures. Finally, they demonstrated improved scan–rescan reproducibility in the quantification of valvular 18F-NaF uptake, particularly when a most-diseased-segment approach was used. Indeed, these enhanced analysis techniques markedly improved reproducibility, resulting in a reduction in percentage error from ±63% to ±10%. Doris et al. (18) have further optimized 18F-NaF PET/CT imaging of the aortic valve. Using a diffeomorphic, mass-preserving, anatomy-guided registration algorithm, they managed to achieve motion correction without excluding any PET data. This novel approach improved the signal-to-noise ratio, with the median noise decreasing by more than half.
These studies have advanced image analysis, allowing for precise image coregistration and highly reproducible tracer localization at the aortic valve leaflet level, with excellent scan–rescan reproducibility of uptake values. These achievements have paved the way for PET imaging in aortic stenosis both as a research tool to improve our pathophysiologic understanding of disease and as an efficacy endpoint in randomized clinical trials of novel potential therapies (19).
AORTIC VALVE DISEASE ACTIVITY
To better understand the pathophysiology of aortic stenosis, we need markers of disease activity that ideally target the principle pathologic processes occurring within the valve. To date, research has concentrated largely on 18F-NaF, a marker of microcalcification and developing calcification activity that is associated with vascular injury and disease progression across multiple different cardiovascular disease states (20–22).
In the first observational prospective cardiovascular 18F-NaF PET study of aortic stenosis, Dweck et al. sought to better describe the relative contribution of inflammation and calcification activity in aortic stenosis using PET (20). One hundred twenty-one patients with calcific aortic valve disease (20 control subjects; 20 patients with aortic sclerosis; and 25 patients with mild, 33 with moderate, and 23 with severe aortic stenosis) underwent both 18F-NaF and 18F-FDG PET/CT at baseline with repeat echocardiography and CT calcium scoring to track disease progression. Compared with control subjects, both patients with aortic sclerosis and patients with aortic stenosis showed increased 18F-FDG uptake. Up to 20% of patients with aortic sclerosis and 35% of patients with aortic stenosis showed 18F-FDG uptake, which progressively increased with disease severity, emphasizing the underlying metabolically active nature of the disease and confirming previous observations (23). Increased 18F-NaF uptake was clearly observed in patients with aortic valve disease compared with control subjects, with activity increasing more rapidly and progressively with advancing disease severity. In total, 45% of patients with aortic sclerosis and 91% of those with aortic stenosis had increased uptake. The proportion of patients with increased activity rose sharply with increasing disease severity, so that by the later stages of the disease 18F-NaF uptake greatly outweighed 18F-FDG uptake, despite the reverse being true in coexistent regions of aortic atheroma (24). This finding underlined the central importance of calcification activity in aortic stenosis, particularly in those with moderate and severe disease, as well as providing a potential explanation for the discrepant effects of statin therapy in the 2 conditions.
Progression of aortic stenosis disease after baseline PET/CT imaging was assessed at 1 and 2 y using CT aortic valve calcium scoring and transthoracic echocardiography. On repeat CT imaging, new valvular calcium was visible in a distribution similar to that of 18F-NaF uptake observed on the baseline PET images (Fig. 1). Indeed, baseline 18F-NaF uptake correlated strongly with the subsequent rate of progression in the CT aortic valve calcium score and with echocardiographic measures of hemodynamic progression. Increased 18F-NaF uptake was also an independent predictor of cardiovascular death and aortic valve replacement (hazard ratio, 1.55, and 95% CI, 1.33–1.81 [P < 0.001], after adjusting for age and sex). Although there is a clear need for imaging techniques that can predict aortic stenosis progression and events, the CT aortic valve calcium score provides a broadly similar prediction and, as the cheaper and more widely available technique, has therefore assumed the dominant clinical role. However, 18F-NaF PET has a role in providing novel insights into the pathogenesis of aortic stenosis, in identifying novel treatment targets, and in serving as an endpoint in phase 2 clinical trials seeking to demonstrate their efficacy.
MECHANISTIC INSIGHTS AND CLINICAL TRIALS
The initial 18F-NaF PET studies highlighted the key pathologic role that calcification plays in aortic stenosis, emphasizing that any potential novel therapy would have to try to break the self-perpetuating cycle of valve calcification that drives the propagation phase of this disease. Other PET studies have also highlighted other potential targets, most notably lipoprotein(a) (Lp[a]) (25–27). In a recent multicenter multicohort multimodality imaging study, Zheng et al. (28) investigated the importance of Lp(a) in determining disease activity, disease progression, and clinical events in patients with aortic stenosis. The study included 145 patients with available blood samples for Lp(a) and oxidized phospholipids on apolipoprotein B-100 measurements. On baseline PET/CT, patients having the highest Lp(a) tertile had increased valve 18F-NaF PET/CT uptake and, therefore, calcification activity compared with those in lower tertiles. After follow-up, these PET data translated into accelerated disease progression (assessed by both echocardiography and CT aortic valve calcium score) and more clinical events in patients with the highest Lp(a) tertile. This effect appeared to be mediated by the procalcific, proosteoblastic effects of Lp(a) on valve interstitial cells via the actions of oxidized phospholipid. These findings therefore indicate that Lp(a) lowering or oxidized phospholipid inactivation may slow aortic stenosis progression and, alongside other observational data (29), provide a clear rationale for randomized controlled trials of this strategy.
The capacity of 18F-NaF PET/CT to measure calcification activity in aortic stenosis, combined with its excellent scan–rescan reproducibility, makes it an attractive endpoint for clinical studies looking to establish the efficacy of novel therapies for this condition. Changes in valvular 18F-NaF uptake may potentially be detectable earlier than with standard assessments of disease progression made with echocardiography and CT aortic valve calcium scoring, which require several years to demonstrate a treatment effect. Several recent studies utilized 18F-NaF PET/CT to gain insights into the pathophysiology underlying aortic stenosis and as an endpoint of clinical interventional trials. Indeed, this hypothesis is being evaluated in numerous ongoing clinical trials of novel therapies and mechanistic insights in aortic stenosis—trials in which 18F-NaF PET is being used as an exploratory endpoint (Table 1).
Studies Using PET Radiotracers in Patients with Aortic Stenosis
In a recently published double-blind randomized controlled trial (Scottish Aortic Stenosis and Lipid Lowering Trial, Impact on Regression—SALTIRE II; NCT02132026) (19), 18F-NaF PET/CT was utilized as an exploratory secondary endpoint to establish whether alendronate or denosumab could reduce disease activity and slow disease progression in patients with aortic stenosis. Participants underwent serial assessments with Doppler echocardiography, CT aortic valve calcium scoring (baseline and 24 mo), 18F-NaF PET (baseline and after 1 y of therapy), and coronary CT angiography. The study clearly demonstrated that denosumab and alendronic acid have no effect on calcification activity as assessed with 18F-NaF PET, nor do they affect disease progression as assessed with either echocardiography or CT aortic valve calcium scoring. Nevertheless, baseline aortic valve 18F-NaF maximum target-to-background ratio was once again associated with subsequent progression in the CT aortic valve calcium score and peak aortic jet velocity, confirming previous observations (30). The ongoing BASIK-2 trial (NCT02917525) seeks to influence calcification activity in aortic stenosis via an alternative pathway, investigating the effects of vitamin K2 on 18F-NaF PET activity and CT aortic valve calcium scoring progression in patients with bicuspid aortic valve disease (31).
BIOPROSTHETIC VALVE DEGENERATION
An aging population and the lack of suitable medical therapies have led to a marked rise in the implantation of bioprosthetic heart valves (32). In the United States, there were more than 65,000 surgical bioprosthetic valves implanted and more than 72,000 transcatheter aortic valve implantation procedures in 2019 alone (32). Bioprosthetic valve degeneration remains a major issue, but noninvasive methods for detecting this degenerative process have been lacking. Current modalities (echocardiography and CT) struggle to visualize leaflet degeneration because of the blooming artifact and acoustic shadowing caused by the valve stent struts. Detection of prosthetic valve degeneration relies on Doppler echocardiography and identification of apparent hemodynamic valve dysfunction: a very late finding in the natural history of the disease. Consequently, even with meticulous clinical follow-up and serial echocardiography, many patients present with unheralded valve failure, requiring an emergent repeat operation accompanied by a high mortality (22.6%, compared with 1.4% for elective repeat surgery) (33). The development of imaging modalities that can detect bioprosthetic valve degeneration earlier is therefore a critical unmet clinical need. Calcification is the common final pathway of bioprosthetic valve degeneration, leading Cartlidge et al. (34) to hypothesize that 18F-NaF PET imaging, using protocols similar to those applied to aortic stenosis, might identify the early stages of bioprosthetic valve degeneration and predict subsequent deterioration in bioprosthetic valve function. In the “18F-Fluoride Assessment of Aortic Bioprosthesis Durability and Outcome Study” (18F-FAABULOUS) (34), 71 patients with surgical bioprosthetic aortic valve replacements of different ages and no clinical or echocardiographic evidence of bioprosthetic valve degeneration or dysfunction underwent baseline 18F-NaF PET/CT imaging using motion-correction and contrast-enhanced CT angiography, as well as echocardiographic and clinical follow-up. Patients with increased 18F-NaF uptake exhibited overt deterioration in bioprosthesis function during follow-up, with a strong correlation observed between baseline valve PET activity and a subsequent change in bioprosthetic peak aortic velocity. On multivariable analysis, 18F-NaF uptake was the only independent predictor of future bioprosthetic dysfunction, outperforming all other variables, including valve type and age, and echocardiographic and CT findings (Fig. 2).
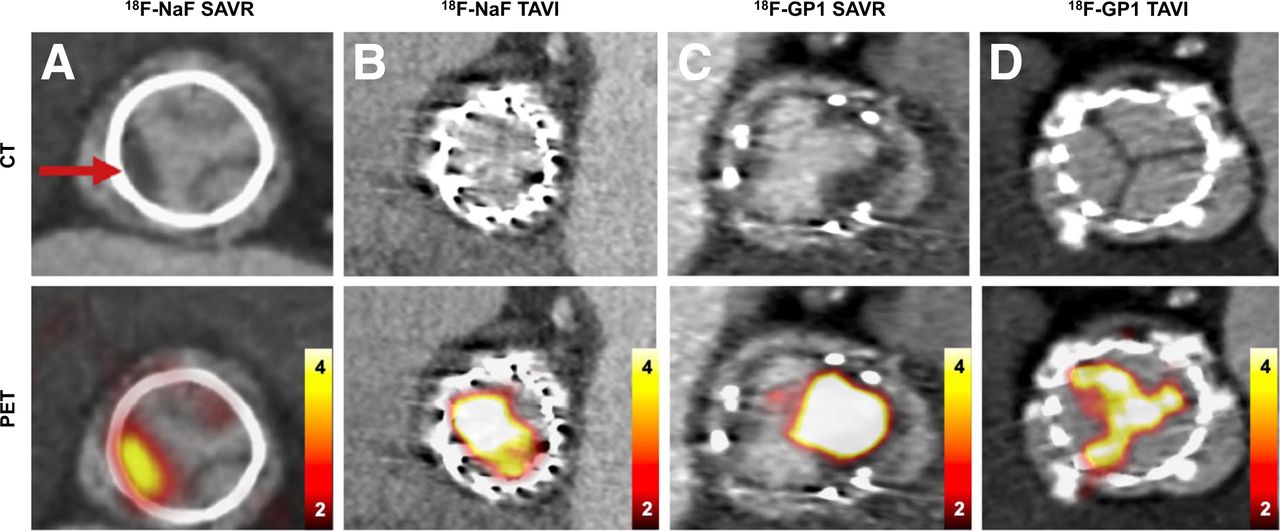
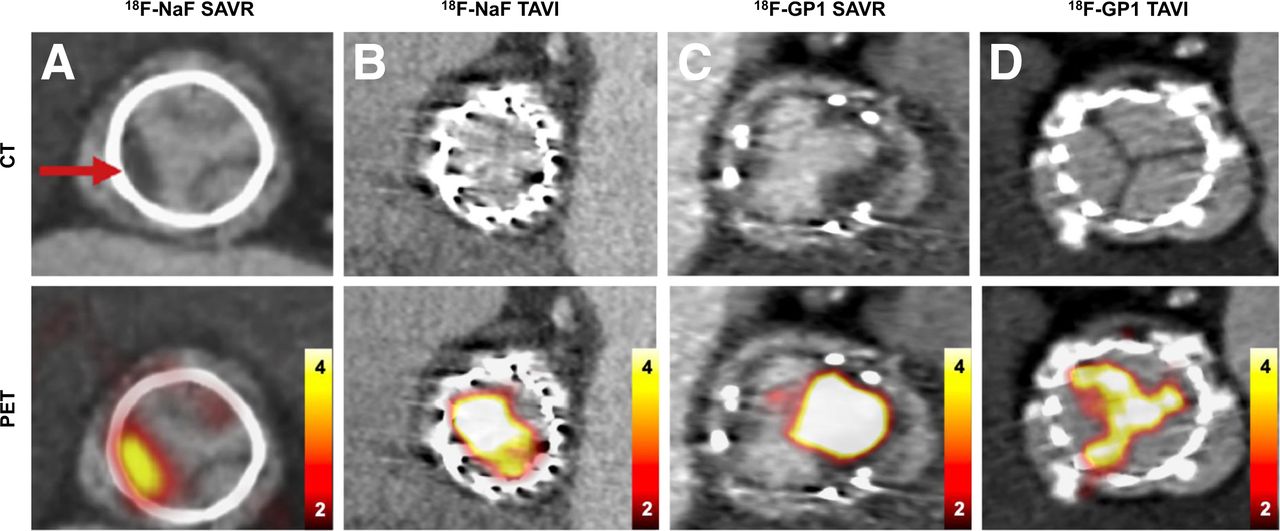
Surgical aortic valve replacement and transcatheter aortic valve implantation. (A) CT en face of surgical aortic valve replacement with evidence of hypoattenuated leaflet thickening, and hybrid 18F-NaF PET/CT with intense tracer activity originating from area of hypoattenuated leaflet thickening. (B) CT en face of transcatheter aortic valve implantation with no evidence of structural leaflet abnormalities and normal baseline echocardiography results, and 18F-NaF PET CT with intense tracer activity originating from transcatheter aortic valve implantation leaflets. Patient required transcatheter aortic valve implantation 12 mo later. (C) In patient with clinical bioprosthetic valve thrombosis, CT showing extensive hypoattenuated leaflet thickening on aortic aspect of right coronary cusp, consistent with thrombus, and very intense 18F-GP1 PET uptake in region of heaviest thrombus burden. (D) Normal transcatheter aortic valve implantation and normal baseline echocardiography results as seen on CT, and 18F-GP1 PET uptake confirming ongoing platelet activation on transcatheter aortic valve implantation leaflet tips. SAVR = surgical aortic valve replacement; TAVI = transcatheter aortic valve implantation.
We have recently confirmed these data using a cohort of 47 patients who had undergone transcatheter aortic valve implantation (35). In these patients, baseline 18F-NaF uptake once again demonstrated a close association, with the subsequent change in bioprosthetic valve performance emerging as the most powerful predictor of future bioprosthetic valve dysfunction. Interestingly, similar rates of valve degeneration were observed using 18F-NaF PET, CT, and echocardiography, indicating similar midterm durability of transcatheter aortic valve implantation and surgical bioprosthetic aortic valve replacements. Given the apparent advantages of 18F-NaF PET in the detection of bioprosthetic valve degeneration over CT and echocardiography, and the clinical need to identify such degeneration, further studies are now required to confirm how 18F-NaF might best be used to aid clinical assessment in this area (Fig. 2).
FUTURE TRACERS
Recently, new radiotracers targeting thrombus formation, inflammation, and fibrosis activity with major potential for both aortic stenosis and bioprosthetic valve degeneration have become available. 18F-GP1 is a novel radiotracer that binds with high affinity to the glycoprotein IIb/IIIa receptor on activated platelets (36). It can detect in vivo venous and arterial thrombosis and shows higher sensitivity than other current imaging modalities (36–39). In the “18F-GP1 PET/CT to Detect Bioprosthetic Aortic Valve Thrombosis Study” (NCT04073875), we have used this tracer in a cross-sectional analysis involving 72 participants: 50 with bioprosthetic aortic valves and 22 with normal native valves. We showed that all bioprosthetic valves but no native aortic valves demonstrated focal 18F-GP1 uptake in the valve leaflets. Higher 18F-GP1 uptake was independently associated with hypoattenuated leaflet thickening and duration of valve implantation but not with valve type (Fig. 2). This finding suggests widespread platelet activation on the surface of all bioprosthetic valves, with further work now required to understand whether and how this activation relates to subsequent bioprosthetic valve degeneration (40).
68Ga-labeled fibroblast-activation protein inhibitor is a novel tracer that is highly specific for activated fibroblasts and demonstrates intense signal in regions of developing fibrosis activity across multiple organ systems. We are currently exploring the utility of this tracer in patients after myocardial infarction and in patients with aortic stenosis.
68Ga-DOTATATE targets the somatostatin receptor expressed by activated macrophages and might therefore also prove of value in better understanding the role of inflammation in aortic stenosis and improving on the data provided by 18F-FDG, which has been limited by nonspecific physiologic tracer activity in the myocardium (41).
Finally, ammonia 13N PET myocardial perfusion imaging has recently been used to assess myocardial ischemia in patients with aortic stenosis. Zhou et al. (42), in a prospective observational study involving 34 patients with aortic stenosis, showed that rest and stress myocardial flow reserve were associated with adverse myocardial characteristics and markers of myocardial stress and injury, suggesting that ischemia has an important role in left ventricular decompensation in patients with aortic stenosis and that perfusion assessments may prove useful diagnostic information.
LIMITATIONS
PET/CT has evolved significantly over the last decade. Nevertheless, significant challenges remain in place. Among others, these include radiation exposure, high costs of imaging, and relatively limited access to PET scanners. Moreover, cardiac PET imaging is made more complicated by motion (cardiac, respiratory, and patient) and by long acquisition times (≤30 min). Variations in the time between tracer injection and imaging can affect quantitative assessments of disease activity. Image-quality degradation, caused by patient motion during imaging protocols with long acquisition times, leads to impaired quantitative accuracy. Optimization studies have helped to overcome these hurdles and led to improved disease activity quantification (17,18).
CONCLUSION
Echocardiography will remain the cornerstone of clinical evaluation for most patients with aortic stenosis. However, CT aortic valve calcium scoring has already assumed an important clinical role as an alternative assessment of disease severity for those with intermediate or discordant findings. PET imaging with 18F-NaF provides complementary information on disease activity in both native and bioprosthetic valves and has become an established and exciting research tool that has altered our understanding of the pathology of aortic stenosis and is advancing development of the effective medical therapies urgently required for this increasingly prevalent condition. There are several emerging tracers that promise to expand our ability to track several pathophysiologic mechanisms and to help us understand, treat, and perhaps prevent aortic stenosis and bioprosthetic valve degeneration.
DISCLOSURE
Evangelos Tzolos was supported by a British Heart Foundation grant (BHF Clinical Research Training Fellowship Application, case reference FS/CRTF/20/24086). David Newby is supported by the British Heart Foundation (CH/09/002, RG/16/10/32375, and RE/18/5/34216). Marc Dweck is supported by the British Heart Foundation (FS/14/78/31020 and FS/SCRF/21/32010) and is the recipient of the Sir Jules Thorn Award for Biomedical Research 2015 (15/JTA). This research was supported in part by grants R01HL135557 from the National Heart, Lung, and Blood Institute/National Institute of Health (NHLBI/NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online December 09, 2021.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication September 28, 2021.
- Revision received December 6, 2021.
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Evolution of Cardiac Nuclear Imaging
- Multimodality Imaging of Aortic Valve Calcification and Function in a Murine Model of Calcific Aortic Valve Disease and Bicuspid Aortic Valve
- Multimodality Imaging of Aortic Valve Calcification and Function in a Murine Model of Calcific Aortic Valve Disease and Bicuspid Aortic Valve
- Radiotracers to Address Unmet Clinical Needs in Cardiovascular Imaging, Part 2: Inflammation, Fibrosis, Thrombosis, Calcification, and Amyloidosis Imaging