


Visual Abstract

Abstract
Our objective was to compare the respective value of 68Ga-DOTATOC and 18F-DOPA PET/CT for initial staging or presurgical work-up of patients with small-intestine neuroendocrine tumors (SiNETs). Methods: This was a retrospective, multicenter, noninterventional investigation involving 53 non–surgically treated SiNET patients who underwent both 68Ga-DOTATOC and 18F-DOPA PET/CT within a 6-mo interval without surgical intervention or therapeutic change between the 2 PET/CT studies. Percentage detection rate was calculated according to per-region and per-lesion analyses. Sensitivity for primary tumor detection was assessed in 37 surgically treated patients, taking surgical results (76 SiNETs) as the diagnostic gold standard. Results: 68Ga-DOTATOC PET/CT and 18F-DOPA PET/CT individually identified at least 1 primary SiNET in 92% (34/37) of the patients. Intestinal tumor multifocality was confirmed by histology in 8 patients. 68Ga-DOTATOC and 18F-DOPA PET/CT were concordantly positive for tumor multifocality in 5 patients, discordantly positive in 2 patients, and concordantly negative in 1 patient. The detection rate for subdiaphragmatic nodal metastases on per-region–based analysis was 91% and 98% for 68Ga-DOTATOC and 18F-DOPA PET/CT, respectively (P = 0.18). 18F-DOPA PET/CT detected a higher number of abnormal subdiaphragmatic nodes (P = 0.009). Regarding mesenteric nodes only, 18F-DOPA PET/CT detected more positive regions (P = 0.005) and nodal lesions (P = 0.003) than 68Ga-DOTATOC PET/CT, including nodes at the origin of mesenteric vessels. For detection of distant metastases, 68Ga-DOTATOC and 18F-DOPA PET/CT performed equally well on a per-region–based analysis. As compared with 68Ga-DOTATOC, 18F-DOPA PET/CT detected more hepatic (P < 0.001), peritoneal (P < 0.001), and lung metastases (P < 0.001). Conclusion: 18F-DOPA PET/CT detected more lesions than 68Ga-DOTATOC PET/CT in the studied patients. The respective roles of the two should be discussed in terms of disease staging and treatment selection.
Neuroendocrine tumors (NETs) originating from the gastroenteropancreatic system account for approximately 60% of all NETs. The small intestine, mainly the ileum, is the most common site of primary tumor origin. Despite their slow pace of progression, small-intestine NETs (SiNETs) can extensively spread to mesenteric nodal stations, liver, and bone and can cause pronounced fibrosis locally in the mesentery and at distant sites, as in the heart, leading to extremely serious complications. Surgery is the only potentially curative treatment for nonmetastatic SiNETs (1,2). Identification of distant metastases usually does not prevent (if indicated) surgical resection of primary SiNETs, mesenteric lymph nodes, and mesenteric fibrosis to avoid potential complications (2,3). If curative surgery is possible, the extent of lymph node metastasis must be carefully evaluated because a complete lymphadenectomy decreases the risk of recurrence (4–6). In addition, a 19% rate of missed metastases was reported in the retropancreatic area, a region not systematically explored during surgery (7).
Imaging plays a central role in initial diagnosis for staging (screening for primary multifocality, lymph nodes, systemic metastases, and fibrosis) and for determining operability, the latter being related to the location of nodal lesions or mesenteric fibrosis with regard to the mesenteric arteries (8). Functional imaging can be performed in addition to whole-body CT and liver MRI (9). 68Ga-labeled somatostatin analogs used for somatostatin receptor (SSTR) PET/CT have achieved consensus or near consensus among expert panels as a forefront radiopharmaceutical for SiNETs. 68Ga-somatostatin analog PET/CT has indeed been shown to provide results comparable to those of 18F-DOPA PET/CT at the patient-based level, adding information on SSTR expression status for theranostic application, which is tightly linked to tumor differentiation and patient prognosis. However, a systematic review (10) has shown that despite similar high patient- and region-based pooled sensitivities (83% and 89%, respectively, for 18F-DOPA PET; 88% and 92%, respectively, for SSTR PET), 18F-DOPA was superior in lesion detection (lesion-based pooled sensitivity, 95% vs. 82%). These data agree with 2017 European Association of Nuclear Medicine guidelines positioning 18F-DOPA and 68Ga-somatostatin analogs as first-choice radiotracers for SiNETs, except when evaluation of SSRT expression is mandatory before treatment (11). Moreover, the most accurate modality should be required when the assessment of tumor extension needs to be as precise as possible. To this end, in the present study we compared 68Ga-DOTATOC and 18F-DOPA PET/CT in initial staging or in the presurgical work-up of patients with SiNETs.
MATERIALS AND METHODS
Patient Population
This was a retrospective, multicenter, noninterventional investigation conducted in the department of nuclear medicine of 5 academic NET centers in France (Beaujon, Lyon, Marseille, Nancy, and Strasbourg), involving patients with SiNETs evaluated by PET/CT between 2017 and 2021. Patients were retrospectively included according to the following criteria: well-differentiated SiNETs, PET investigations performed for initial staging or presurgical work-up, 68Ga-DOTATOC and 18F-DOPA PET/CT performed within a 6-mo period, and absence of any surgical intervention or therapeutic change between the 2 PET studies. Patients with a history of oncologic intestinal surgery for SiNETs were not considered for the study. Demographics, presence of carcinoid syndrome, imaging results, and pathologic results after surgical resection were collected. Values of serum chromogranin-A (CgA) and 24-h urinary 5-hydroxyindoleacetic acid (5-HIAA) were collected when available. Tumors were graded according to the 2019 World Health Organization classification (12). In accordance with local guidelines, all patients gave written informed consent to the use of anonymous data extracted from their medical records for scientific or epidemiologic purposes. The institutional review board approved this study (Comité d’Ethique 2021-93).
68Ga-DOTATOC and 18F-DOPA PET/CT: Acquisition/Reconstruction Parameters
All examinations were performed on combined PET/CT devices equipped with 3-dimensional time-of-flight technology and without iodinated contrast medium. Patients in a given center were scanned on the same instrument regarding the 2 tracers. Patients were injected with a 2–3 MBq/kg dose of 68Ga-DOTATOC and a 3–4 MBq/kg dose of 18F-DOPA. 68Ga-DOTATOC (SomaKit TOC; Advanced Accelerator Applications) and 18F-DOPA (Dopacis; Cisbio International) were used in the setting of marketing authorization. In cases of concurrent octreotide therapy, 68Ga-DOTATOC PET/CT was performed just before the next octreotide injection. Carbidopa premedication (200 mg orally) was done in 24 cases (45%) 60–90 min before 18F-DOPA intravenous injection. The PET/CT protocol included an acquisition from the upper thigh to the top of the skull (3–5 min/step or continuous bed motion when available), starting approximately 60 or 30 min after injection of 68Ga-DOTATOC or 18F-DOPA, respectively. PET image datasets were reconstructed iteratively (ordered-subset expectation maximization algorithm) using non–contrast-enhanced data for attenuation correction. CT, PET (attenuation-corrected), and PET/CT were independently interpreted by 1 experienced nuclear medicine physician who was aware of patients’ clinical data and the results of biologic, pathologic, and anatomic imaging investigations but not the results of the other PET study. 68Ga-DOTATOC and 18F-DOPA PET/CT from the same patients were analyzed more than 7 d apart.
Interpretation Criteria of PET Studies
PET findings were interpreted as either positive or negative. A positive PET result was defined as detection of at least 1 focus of pathologically increased uptake relative to surrounding tissue and physiologic biodistribution. For per-region analysis, the following 9 anatomic regions were analyzed: small intestine (i.e., primary tumors), peritoneum, liver, abdominal lymph nodes, left-sided supraclavicular lymph nodes, supradiaphragmatic lymph nodes (excluding the left supraclavicular region), lungs/pleura, bones, and others. Moreover, mesenteric lymph nodes were analyzed independently, according to the Pasquer et al. (7) classification: group 1 included those in contact with the small bowel; group 2, in the middle of the mesentery; and group 3, at the origin of the mesenteric vessels under the pancreatic uncus. A region was considered positive when it contained at least 1 focal uptake abnormality, regardless of the number of positive foci. Finally, for per-lesion analysis, the number of lesions in each region was recorded. If the number exceeded 20, the count was fixed at 20.
Statistical Analysis
Results for continuous variables were expressed as mean and SD or range, as appropriate, whereas categoric variables were expressed as frequencies and percentages. For ethical reasons, histologic proof of all potentially metastatic lesions was not possible, and pathologic 68Ga-DOTATOC or 18F-DOPA uptake was considered a true-positive result. The sum of positive regions and lesions on either 68Ga-DOTATOC or 18F-DOPA PET/CT was considered the total number of involved regions and lesions. The percentage detection rate (DR) of 68Ga-DOTATOC and 18F-DOPA PET/CT was calculated according to per-region and per-lesion analyses. 68Ga-DOTATOC and 18F-DOPA PET/CT sensitivity for primary tumor detection was assessed in surgically treated patients using surgical findings as the diagnostic gold standard. Region-to-region and lesion-to-lesion comparisons between 68Ga-DOTATOC and 18F-DOPA PET/CT were performed using the McNemar test. Correlations were assessed using the Spearman ρ-correlation test. A 2-sided P value of less than 0.05 was considered significant. Statistical analyses were performed using freely available statistical software (Jamovi, version 1.8).
RESULTS
Patient Population
Of 59 screened patients, 2 were excluded because they had undergone surgery before PET/CT, 2 because of more than a 6-mo delay between the 2 PET/CT studies, 1 because 18F-DOPA PET/CT data were not available, and 1 because there were more than 100 SiNETs. Hence, 53 patients were included in the analysis. Their characteristics are summarized in Table 1. The population comprised 31 (58%) women and 22 (42%) men, with a mean age of 65 ± 13 y (range, 33–89 y). Fifteen patients (28%) were referred because of clinical and radiologic suspicion of SiNETs (afterward histologically confirmed), and 38 (72%) patients presented with biopsy-proven metastatic SiNETs.
Patient Population and Tumor Characteristics
Tumors were classified as grade 1 in 23 (43%) patients, grade 2 in 25 (47%) patients, and well-differentiated grade 3 in 3 (6%) patients (mean Ki-67, 5.8% ± 8.7%; median Ki-67, 3.7%; range, 1%–44%). The Ki-67 index was not available for 2 (4%) patients with well-differentiated tumors. Nineteen (36%) patients had carcinoid syndrome. Serum CgA and urinary 5-HIAA were elevated in 28 (53%) and 14 (26%) patients, respectively. At the time of PET/CT, 13 (25%) patients were treated by long-acting somatostatin analogs. The mean interval between the 2 modalities was 29 ± 76 d (range. 1–161 d), and 68% of patients had the 2 examinations within 28 d. After PET/CT, 37 of 53 (70%) patients underwent oncologic surgery, and histology revealed a total of 76 primary SiNETs.
Similar Primary SiNET Detection Rates Shown by 18F-DOPA and 68Ga-DOTATOC PET/CT
68Ga-DOTATOC and 18F-DOPA PET/CT sensitivity for primary SiNET detection was assessed from the analysis of 37 surgically treated patients and 76 histologically detected SiNETs. The ability of both imaging modalities to detect a multifocal intestinal disease was also evaluated.
In 32 (86%) patients, 68Ga-DOTATOC and 18F-DOPA PET/CT were concordant and identified at least 1 primary SiNET. PET/CT was discordant in an additional 4 (11%) patients: 2 patients showed positive uptake on 68Ga-DOTATOC PET/CT only, and 2 other patients showed positive uptake on 18F-DOPA PET/CT only. The Ki-67 of tumors detected by 18F-DOPA PET (44% and 10%) was higher than that of tumors revealed by 68Ga-DOTATOC PET (1% and 2%). However, no statistical considerations were possible.
In the remaining case (3%), no primary SiNET was revealed by either PET/CT modality despite 2 SiNETs detected by pathology. Accordingly, per-region sensitivity was 94% for both techniques (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
According to a lesion-based analysis, 45 of 76 (59%) histologically confirmed SiNETs were detected by both modalities, 13 (17%) by 68Ga-DOTATOC only, and 8 (11%) exclusively by 18F-DOPA. Ten (13%) tumors were not detected by either modality. The sensitivity of 68Ga-DOTATOC and 18F-DOPA was, respectively, 76% and 70% (P = 0.275) (Table 2). CgA and 5-HIAA did not differ with metabolic tumor imaging profile (P = 0.73 for CgA, P = 0.80 for 5-HIAA). Tumor intestinal multifocality was confirmed by histology in 8 (16%) patients. Among them, 68Ga-DOTATOC and 18F-DOPA PET/CT were concordantly positive for tumor multifocality in 5 (63%) patients. In 2 patients (25%), PET/CT studies were discordantly positive (1 patient with only 68Ga-DOTATOC PET/CT positivity, and 1 patient with only 18F-DOPA PET/CT positivity). In the last patient, both 68Ga-DOTATOC and 18F-DOPA PET/CT failed to detect multifocal disease.
Comparison Between 68Ga-DOTATOC and 18F-DOPA PET/CT for Primary SiNETs and Metastases (DR): Per-Lesion Analysis
Better Performance of 18F-DOPA Than of 68Ga-DOTATOC PET/CT for the Evaluation of LN Metastases
Mesenteric Lymph Nodes
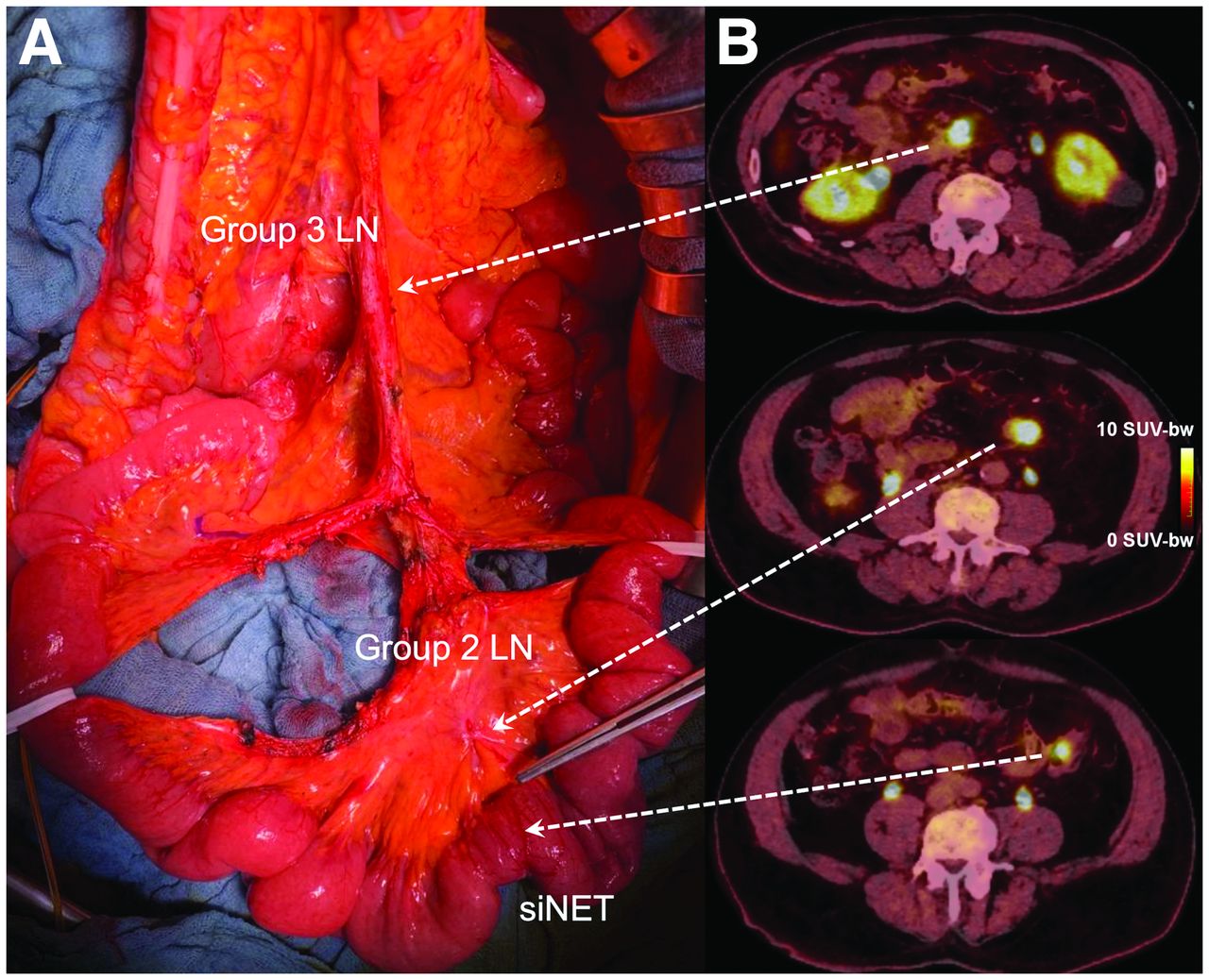
Three lymph node groups were considered (7), group 1 being lymph nodes in contact with the small bowel; group 2, in the middle of the mesentery; and group 3, at the origin of the mesenteric vessels under the pancreatic uncus. Pathologic data about nodal PET/CT positivity according to this 3-scale classification were available for 32 selected patients (Fig. 1) from Strasbourg and Beaujon University Hospitals.

Correlation of surgical exploration and 18F-DOPA PET/CT findings in patient with grade 1 SiNETs and metastatic mesenteric lymph nodes of groups 2 and 3 according to Pasquer et al. (7).
On a per-region analysis, 33 of the 96 (34%) analyzed regions were considered positive by both modalities and 5 (5%) were only 18F-DOPA–positive. No regions showed an exclusively 68Ga-DOTATOC abnormality. 18F-DOPA detected significantly more positive regions than did 68Ga-DOTATOC (100% vs. 87%; P = 0.025). Regarding subgroup analysis, 2 group 1 regions (17%) (P = 0.157), 2 group 2 regions (10%) (P = 0.157), and 1 group 3 region (17%) (P = 0.317) were positive only on 18F-DOPA PET/CT (Supplemental Table 1).
Per-lesion–based analysis revealed a total of 67 nodal mesenteric pathologic foci of either 68Ga-DOTATOC or 18F-DOPA uptake, of which 58 (87%) were common to both modalities: 14 of 16 (88%) for group 1, 33 of 36 (92%) for group 2, and 11 of 14 (79%) for group 3. No lymph node was positive only on 68Ga-DOTATOC PET/CT, and 9 (14%) were positive only on 18F-DOPA PET/CT. Global DR of 18F-DOPA PET/CT was significantly higher than that of 68Ga-DOTATOC PET/CT (100% vs. 88%, P = 0.003). Moreover, a statistically significant difference was observed for group 3 when considered independently (100% vs. 79%, P = 0.046) or pooled with group 2 (100% vs. 86%, P = 0.008). Finally, DR was equivalent for both group 1 (100% vs. 88%, P = 0.16) and group 2 (100% vs. 92%, P = 0.32) when analyzed independently. Results are summarized in Table 2.
Subdiaphragmatic Lymph Nodes
On a per-region analysis, 40 (75%) patients had at least 1 subdiaphragmatic lymph node detected by 68Ga-DOTATOC and 18F-DOPA PET/CT; 1 (2%), by 68Ga-DOTATOC only; and 4 (8%), by 18F-DOPA only. In 8 (15%) patients, no pathologic subdiaphragmatic lymph nodes were detected by both modalities. DR did not significantly differ between 68Ga-DOTATOC and 18F-DOPA (91% vs. 98%, P = 0.18; Supplemental Table 1).
On a per-lesion analysis, 184 subdiaphragmatic foci of lymph node pathologic uptake of either 68Ga-DOTATOC or 18F-DOPA were revealed, and 159 (86%) were common to both modalities. Six (3%) and 19 (10%) additional nodal abnormalities were detected by 68Ga-DOTATOC and by 18F-DOPA PET/CT, respectively (DR, 90% vs. 97%; P = 0.009). Results are summarized in Table 2.
Detection of More Distant Metastases with 18F-DOPA PET/CT Than with 68Ga-DOTATOC PET/CT
On a per-region–based analysis, 28 (53%) patients showed liver uptake abnormalities. Among them, 26 (93%) showed such abnormalities on both 68Ga-DOTATOC and 18F-DOPA PET/CT. In the remaining 2 (7%) patients, only 18F-DOPA PET revealed liver metastases (P = 0.346) (Fig. 2). No patient had hepatic lesions detectable only on 68Ga-DOTATOC PET/CT. No significant difference was seen between 68Ga-DOTATOC and 18F-DOPA PET/CT for the remaining anatomic regions (i.e., peritoneum, abdominal lymph nodes, left-sided supraclavicular lymph nodes, supradiaphragmatic lymph nodes [excluding the left supraclavicular region], lung/pleura, bones, and other metastatic sites). Results are summarized in Supplemental Table 1.
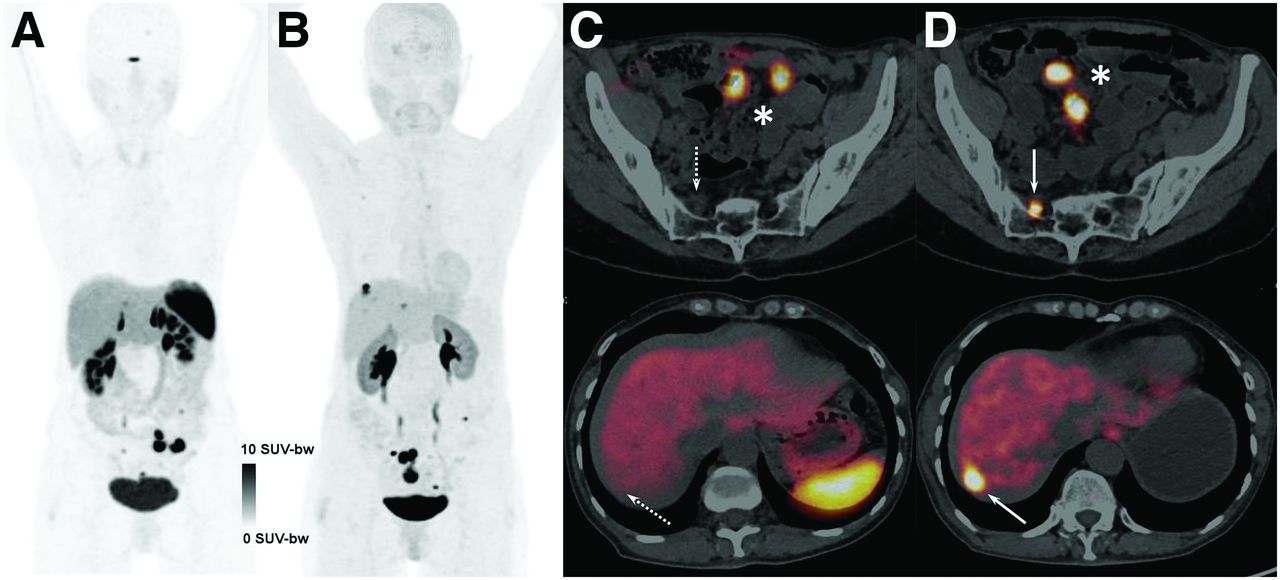
Head-to-head comparison between 68Ga-DOTATOC (A and C) and 18F-DOPA PET/CT (B and D) in oligometastatic patient with bifocal SiNETs (*). 68Ga-DOTATOC PET/CT failed to detect hepatic and peritoneal metastases (dotted arrows), visible only on 18F-DOPA PET/CT (solid arrows). SUV-bw = (PET image pixel value) * (weight in grams) / (injected dose).
On a per-lesion–based analysis, 671 foci of pathologic uptake on either 68Ga-DOTATOC or 18F-DOPA indicating extranodal metastases were detected (Table 2). Among them, 491 (73%) were common to both modalities, 38 (6%) were detected on 68Ga-DOTATOC only, and 142 (21%) were detected on 18F-DOPA only. 18F-DOPA had a better global DR for detection of distant metastases than did 68Ga-DOTATOC (94% vs. 79%, P < 0.001). 18F-DOPA PET/CT performed better than 68Ga-DOTATOC PET/CT for the detection of liver metastases (98.9% vs. 87.4%, P < 0.001), peritoneal carcinomatosis (95.5% vs. 47.3%, P < 0.001), and lung metastases (100% vs. 50.0%, P < 0.001). 68Ga-DOTATOC PET/CT detected significantly more left supraclavicular lymph nodes than did 18F-DOPA (100% vs. 82.6%, P = 0.046). Finally, no statistically significant difference was observed for bone metastases and supradiaphragmatic lymph nodes.
Imaging Protocol, Ki-67, Tumor Grade, and Biologic Markers
Thirty-one and 22 patients underwent 68Ga-DOTATOC before 18F-DOPA PET/CT and vice versa, respectively. In both cases, 18F-DOPA PET revealed more lesions than did 68Ga-DOTATOC PET (P = 0.002, 18F-DOPA first; P < 0.001, 68Ga-DOTATOC first). The number of discordant lesions did not correlate with the time between the 2 PET studies (ρ = 0.286; P = 0.081), suggesting a minor influence of the imaging sequence on final PET/CT results.
No correlation was showed between Ki-67 index and the number of discordant lesions in the entire population (ρ = 0.06; P = 0.67) and only in patients with discordant PET results (ρ = 0.23; P = 0.17).
The lesion-based detection rate of 18F-DOPA PET was better than that of 68Ga-DOTATOC PET regardless of the tumor grade (grade 1, P < 0.001; grade 2, P < 0.001; grade 3, P < 0.004) and patient treatment (long-acting somatostatin analogs, P < 0.001; no treatment, P < 0.001).
Quantitative values of serum CgA and urinary 5-HIAA were available for 35 (66%) and 26 (49%) patients, respectively. CgA and 5-HIAA levels were increased in 28 and 14 patients, respectively. A moderate statistically significant correlation was found between the total number of lesions detected by either 68Ga-DOTATOC or 18F-DOPA and the level of CgA (ρ for DOTATOC = 0.32, P = 0.003; ρ for DOPA = 0.36, P = 0.016) and 5-HIAA (ρ for DOTATOC = 0.34, P = 0.043; ρ for DOPA = 0.44, P = 0.013).
DISCUSSION
Only a few studies have compared 68Ga-DOTATOC and 18F-DOPA PET/CT in patients with SiNETs. Before further considerations, it is necessary to distinguish diagnostic from theragnostic applications. 68Ga-somatostatin analog PET/CT remains mandatory for selecting candidates for PRRT. By contrast, the choice of the most appropriate diagnostic imaging modality should rely on diagnostic performance. Thus, there is no reason to disqualify 18F-DOPA PET/CT in a purely diagnostic setting (13).
In our series, 68Ga-DOTATOC and 18F-DOPA PET/CT identified at least 1 primary SiNET in 86% of cases, achieving a similar per-lesion sensitivity of 76% and 70%, respectively. Several reasons may decrease the detectability of small primaries on PET/CT, such as the partial-volume effect and bowel peristalsis. The sensitivity of conventional presurgical diagnostic investigations remains suboptimal, and intraoperative palpation of the entire small intestine should routinely be performed to improve the detection of multifocal primary SiNETs (14).
Resection of at least 8 lymph nodes is advocated (when possible), along with resection of the primary SiNET (6,15). A systematic extensive nodal resection including the retropancreatic area around the origin of the superior mesenteric vessels has been proposed to prevent unresectable local recurrence (3,16). Moreover, up to 67% of patients could present with skip metastases, of which 19% are retropancreatic (group 3), without nodal invasion around the mesenteric vessels (7). In our study, the DR of subdiaphragmatic metastatic lymph nodes during initial staging was significantly higher for 18F-DOPA than for 68Ga-SSTR PET/CT. Moreover, when we focused exclusively on mesenteric lymph node metastases, 18F-DOPA PET/CT detected more positive regions (groups 1–3) and metastatic lymph nodes than did 68Ga-DOTATOC PET/CT (P = 0.005 and 0.003, respectively). Noteworthy, a statistically significant difference (P = 0.046) was also shown for the detection of group 3 pathologic lymph nodes. This result appears to be novel, and given its potential therapeutic impact on patients with SiNETs, it will need to be confirmed by prospective clinical trials.
18F-DOPA performed better than 68Ga-DOTATOC PET/CT for the detection of lesions in the liver (P < 0.001), peritoneum (P < 0.001), and lung (P < 0.001). Similar results have been recently reported by our group from the retrospective comparison of 68Ga-DOTATOC and 18F-DOPA PET/CT in a series of 41 patients with well-differentiated SiNETs during the postsurgical follow-up (17). 18F-DOPA PET/CT was found to have a significantly higher metastatic DR than did 68Ga-DOTATOC PET/CT (P < 0.001). Of 605 lesions, 122 (20%) were revealed exclusively by 18F-DOPA PET/CT. The liver was the region with the highest number of discordant results. Moreover, a trend toward significance (P = 0.07) was shown for the detection of bone metastases, in favor of 18F-DOPA PET/CT. In the recent study of Deleval et al. (18), 18F-DOPA PET/CT detected bone metastases in 46 of 155 (29.7%) SiNET patients, with negative prognostic impact.
Ansquer et al. (19) retrospectively compared 18F-DOPA and 68Ga-DOTANOC PET/CT in 30 patients with SiNETs. PET/CT was performed for primary staging in 9 patients, including 4 patients before surgery and 5 after surgical removal of the primary SiNET. The remaining 21 patients were investigated during regular follow-up. In total, 221 lesions were detected. Even in this case, 18F-DOPA PET/CT identified significantly more lesions than did 68Ga-DOTANOC PET/CT, with a sensitivity of 95.5% and 88.2%, respectively (P < 0.0001). 18F-DOPA PET/CT detected more lesions than did 68Ga-DOTANOC PET/CT in 9 patients (30%) and revealed 22 additional lesions from variable locations. Concerning the detection of primary SiNETs, both imaging methods showed excellent sensitivity, with detection in all 14 patients without previous surgery. When considering only liver metastases visualized by both radiotracers, the ratio of tumor SUVmax to liver SUVmean was higher for 18F DOPA than for 68Ga-DOTANOC for 30 of 46 lesions (62.5%). These findings could explain the better sensitivity of 18F-DOPA for liver metastasis detection. Perhaps the upcoming clinical availability of SSTR antagonists will allow better detection of lesions (20), warranting further head-to-head comparative studies. In these 2 comparative reports, different 68Ga-SSTR analogs were used for PET/CT imaging (i.e., DOTATOC and DOTANOC), but the results always remained in favor of 18F-DOPA. The choice of the SSTR subtype remains probably marginal without explaining the diagnostic difference between 18F-DOPA and 68Ga-SSTR PET/CT (21).
Veenstra et al. (22) retrospectively compared the detection rates of 18F-DOPA and 68Ga-DOTATOC PET/CT for the localization of primary tumor and metastases in 45 patients with NETs, including 23 (51%) SiNETs. 18F-DOPA revealed significantly more lesions than did 68Ga-DOTATOC in 16 SiNET patients (70%) with high circulating biomarker levels. The relationship between tumor markers, clinical features, and primary tumor location has been previously highlighted to optimize radiotracer selection in patients with NETs (23,24).
We acknowledge that the present study like previous ones (17,19,22), was not tailored for assessing the potential therapeutic impact of the detection of additional sites on 18F-DOPA PET/CT compared with SSTR PET/CT. An additional limitation of our study was the lack of an objective gold standard as an imaging comparator for all pathologic uptake findings. However, histologic proof of all metastatic lesions was neither reasonable nor feasible.
CONCLUSION
18F-DOPA PET/CT detected more lesions than did 68Ga-DOTATOC PET/CT in the studied patients. Our results provide a great impetus toward the use of 18F-DOPA PET/CT in the evaluation of SiNETs at initial diagnosis or prior surgery. We believe that the respective role of 18F-DOPA and 68Ga-DOTATOC PET/CT should be discussed according to the expected results in terms of disease staging and treatment selection.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Which is the most sensitive nuclear imaging modality for tumor metastasis assessment at initial staging or presurgical work-up in patients with SiNETs?
PERTINENT FINDINGS: 18F-DOPA PET/CT detected more lesions than did 68Ga-DOTATOC PET/CT in the studied patients. When clinically available, 18F-DOPA should be considered the first-choice PET tracer for exhaustive metastasis assessment.
IMPLICATIONS FOR PATIENT CARE: Our results encourage the use of 18F-DOPA PET/CT in the evaluation of SiNETs at initial diagnosis or prior surgery. The respective role of 18F-DOPA and 68Ga-DOTATOC PET/CT should be discussed according to the expected results in terms of disease staging and treatment selection.
Footnotes
Published online May. 19, 2022.
- © 2022 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 9, 2022.
- Revision received April 27, 2022.





{kind=link}
{kind=link}
{kind=link}