


Abstract
1691
Introduction: Left ventricle (LV) detection and segmentation are essential to calculate LV functional parameters from SPECT myocardial perfusion imaging (MPI). Although several algorithms have been developed for 3D LV segmentation, LV segmentation may fail in the presence of large perfusion myocardium defects. We proposed a novel algorithm for LV clustering in MPI, which is more robust than a commercial processing package in the presence of large defects.
Methods: Two groups of datasets were enrolled in this study. The first group includes 40 patients with extensive perfusion defects who were referred for non-gated rest Tl-201 viability study. This dataset was examined to visually assess the success of automatic LV segmentation by an expert nuclear medicine physician. The second group consists of 15 patients underwent non-gated rest/stress 99mTc-sestamibi MPI and coronary CT angiography (CCTA) within 2.5 months of MPI scan on average. These datasets were used to quantitatively analyze the segmented LV volume. Initially, a preferred LV cluster, and the smallest 3D box circumference of it, are founded in the images similar to the Cedars Sinai algorithm (1). Radial count profiles (10 longitudinally and 10 latitudinally) originating from the box center are generated (center point could be manually change based on user input) and the average is taken over these 100 profiles. The maximum of the averaged profile is proposed as the most optimum threshold. The cluster is updated with this suggested threshold. The best ellipsoid is then fitted to the mid-myocardial surface based on the new LV cluster. Altogether, 320 longitudinal and 240 latitudinal line profiles perpendicular to the ellipsoid surface are extracted. Epicardial and endocardial surface points are chosen on each profile based on minimizing a novel nonlinear cost function. This cost function uses position and amount of the maximum on each profile and whole myocardium maximum count value (named as Cmax) as the independent parameters. Finally, 5th-degree polynomial surfaces (with boundary conditions) are fitted to the points cloud. Valve plane detection is began with splitting the smallest 3D box circumference to the epicardial surface to 100 patches along with long axis. Then, with a threshold of 50% of Cmax, those points which have the uppermost position (closer to the basal) in each long-axis patch are chosen. Among these points, those are determined which their distances to a plane with a preferred angle and position are less than the smallest radius of the endocardial ellipsoid. A plane is fitted to these points proposed as the valve plane.
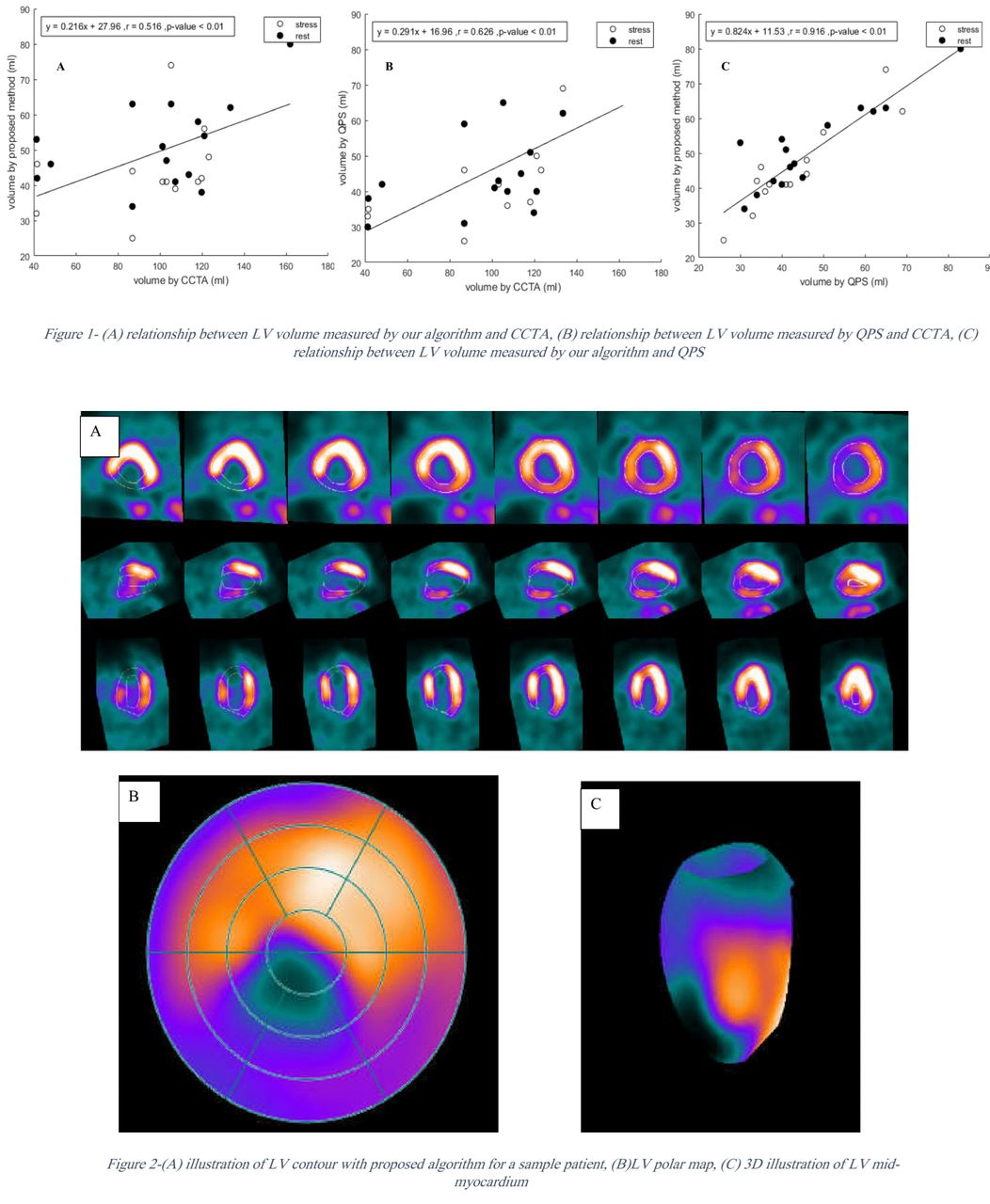
Results: In visual assessment, our proposed algorithm successfully contoured the LV in 100% (both datasets-55 patients) of cases, while the Cedars-Sinai QPS software failed in 3 cases. In quantitative evaluation, LV volumes calculated with the proposed algorithm were correlated with CCTA and QPS outputs with r = 0.516 (p-value<0.01) and r = 0.916 (p-value<0.01), respectively. The ratio of volume obtained from SPECT to CCTA was 0.43 and 0.48 on average by our proposed algorithm and QPS, respectively. Interstudy variability in volume calculation, measured as the variance between rest and stress MPI, was 11% for the proposed method and 4% for QPS.
Conclusions: We develop a novel clustering algorithm for fast and reproducible detection and segmentation of LV in MPI SPECT images, which is more generalizable than commercial software suits in case of the presence of large defects. Proposed user interface and the new approach to determine the intra-patient threshold, paved the road for accurate segmentation of LV in the presence of large perfusion defects.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.