


Abstract
1221
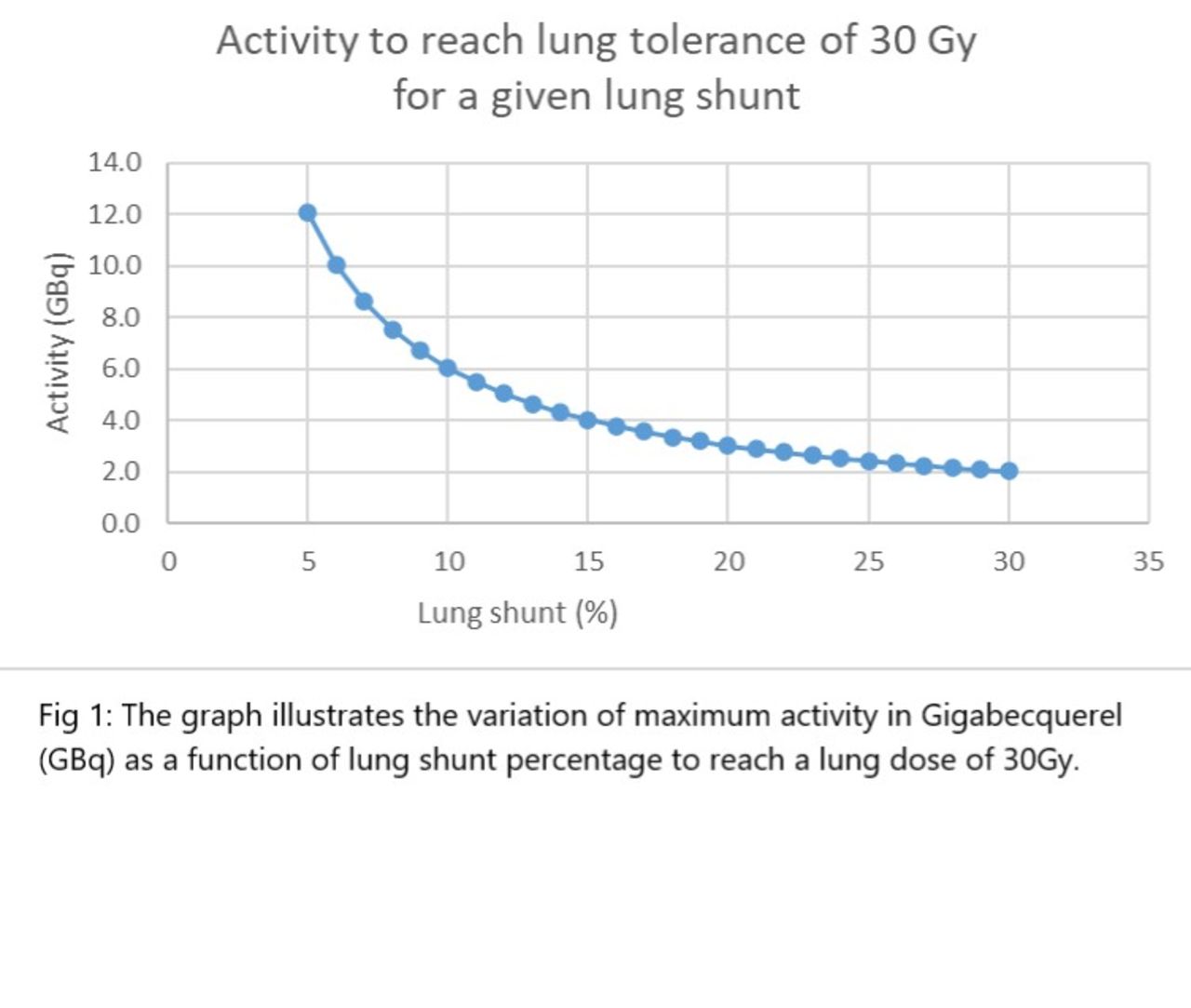
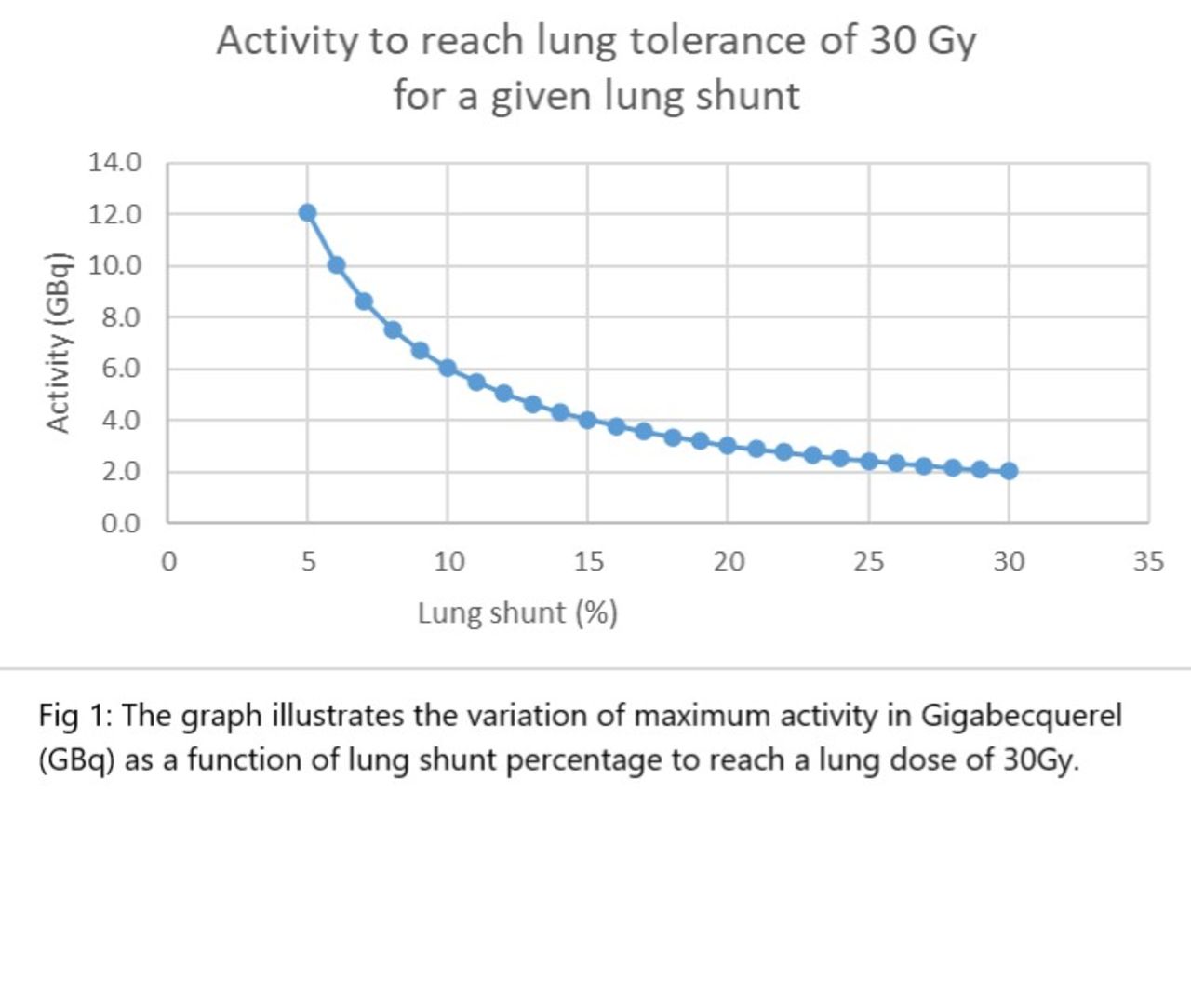
Purpose: Transarterial radioembolization (TARE) is an established brachytherapy for the treatment of unresectable primary or secondary liver malignancy. The current standard of TARE protocol is to perform planning arteriography with technetium 99m macroaggregated albumin before Yttrium 90 (90Y) microsphere radioembolization. The clinical rationale for this step is to quantify lung shunt fraction (LSF) and mitigate the risk of radiation pneumonitis (RP), if any, secondary to arteriovenous shunting in the diseased liver. The pathophysiology in primary liver malignancy is more likely to result in higher hepatopulmonary shunting than other tumors. The objective of this study was to investigate the lung doses observed in patients with metastatic liver malignancy treated by 90Y. Methods: Single institution, IRB approved, retrospective analysis of patients with metastatic liver disease who were referred for TARE between January 2017-September 2020 was performed. Exclusion criteria was defined as presence of underlying cirrhosis, portal hypertension, transjugular intrahepatic portosystemic shunt and portal vein thrombosis.
Results: 35 patients (Male = 20, Female= 15) with a mean age of 57.2 years and adequate liver function (Total bilirubin <2, INR <1.5) underwent 57 planned TARE treatments. 12 patients (34%) had unilobar disease and 23 patients (66%) had bilobar disease. One patient had same day dual segmentectomy. Hepatic metastasis was secondary to colorectal cancer (n=21), cholangiocarcinoma (n=3), neuroendocrine tumor (n=3) and other tumors (n=8). Mean and median LSF was 5.6 and 4.9% (IQR 3.9-7.1). For a median Y90 administered activity of 24.3 millicurie (0.89 GBq) (IQR 0.6-1.3 GBq), the median dose to the treated lobe was 50.6 Gy (IQR 45.2-57.8 Gy) and the median lung dose was 2.4 Gy (IQR 1.3-2.9Gy). Conclusion: In our cohort of patients with metastatic liver disease, the lung dose was clinically negligible while safely delivering an adequate dose to the treated lobe. Hence, pre-planning angiography to determine lung shunt fraction can be omitted in the select patient population, which will lead to decreased time to treatment and more importantly, reduced number of procedures and overall cost of treatment.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.