


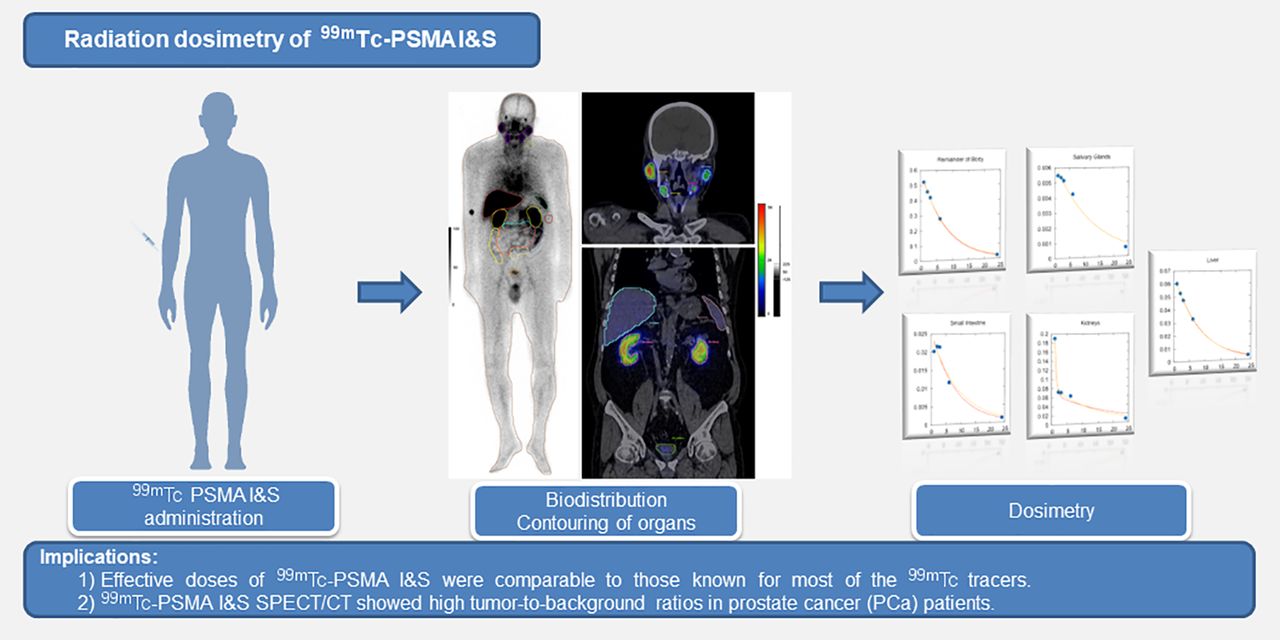
Visual Abstract
Abstract
99mTc-PSMA I&S is a prostate-specific membrane antigen (PSMA) tracer that can be used for planar and SPECT/CT γ-imaging and radioguided surgery. The primary aim of this study was to estimate the dosimetry of 99mTc-PSMA I&S using a hybrid method (sequential γ-planar imaging and 1 single SPECT/CT) in healthy volunteers. The secondary aim was to depict the tracer biodistribution and tumor-to-background ratios (TBRs) in patients with prostate cancer (PCa). Methods: Dosimetry of 99mTc-PSMA I&S was investigated in 4 healthy volunteers. Whole-body planar imaging was acquired at 1, 2, 3, 6, and 24 h and SPECT/CT at 6 h after tracer injection. Contours of organs were drawn on all acquisitions to determine organ activity at each time point. Absorbed dose was estimated using 2 methods: independent curve-fitting manual method (Levenberg-Marquardt–based algorithm using dose factors from RAdiation Dose Assessment Resource [RADAR] website) and OLINDA/EXM software (version 2.0; HERMES Medical Solutions). Biodistribution of 99mTc-PSMA I&S was assessed in 10 patients with PCa on SPECT/CT images at 6 h. Tumor uptake (SUVmax), and TBR (tumor SUVmax/background organ SUVmean) using muscle (T/M), bladder (T/B), and intestine (T/I) as background organs were determined. Results: The mean injected activity of 99mTc-PSMA I&S was 717 MBq (range: 562–828 MBq). No adverse events related to the injection of 99mTc-PSMA I&S were reported. The average radiation effective dose was 0.0055 mSv/MBq with the RADAR manual method and 0.0052 mSv/MBq with OLINDA/EXM. Total body effective dose ranged between 3.33–4.42 and 3.11–4.23 mSv, respectively. All PCa patients showed high tracer uptake in primary and metastatic lesions with T/M, T/B, and T/I ranging from 5.29–110, 0.11–7.02, and 0.96–16.30, respectively. Conclusion: Effective doses of 99mTc-PSMA I&S were comparable to those known for most of the 99mTc tracers and was lower than for the 68Ga-labeled and 18F-labeled agents. 99mTc-PSMA I&S SPECT/CT showed high TBR in PCa patients. This study can provide required data for translation and approval of 99mTc-PSMA I&S by regulatory agencies.
Prostate-specific membrane antigen (PSMA) is a transmembrane metallopeptidase protein highly overexpressed on the surface of prostate cancer (PCa) cells, thus representing a relevant target for PCa nuclear theranostics (1). In the past decade, thousands of PSMA PET scans have been obtained worldwide for staging and restaging PCa, reflecting the rapid and profound clinical adoption by the urooncologist community. 99mTc is the most widely used radionuclide for diagnostic imaging; therefore, 99mTc-labeled PSMA compounds could be a valuable cost-effective alternative in regions in which access to PSMA PET imaging is limited. 99mTc-PSMA imaging can also enable radioguided surgery (RGS) with intraoperative γ-detection. PSMA-targeted RGS can help and guide urologists to detect PCa lymph node (LN) metastasis during surgery. Different 99mTc-PSMA compounds have been developed. 99mTc-Mas3-y-nal-k(Sub-KuE) (99mTc PSMA I&S) is a nonpatented compound derived from the PSMA I&T precursor that can be obtained with a reliable kit-labeling procedure (2). Previous work has shown the utility of 99mTc-PSMA I&S for RGS in large retrospective cohorts with improved treatment outcome (3,4). As a required step for further translation and approval by regulatory agencies, the primary objective of this study was to provide the radiation dosimetry analysis of 99mTc-PSMA I&S in healthy volunteers using a hybrid imaging method (sequential γ-planar imaging and a single SPECT/CT). The secondary aim was to describe the biodistribution of 99mTc-PSMA I&S in PCa patients at 6 h after tracer injection.
MATERIALS AND METHODS
Study Design and Patients
This is a prospective study of radiation dosimetry and biodistribution of a novel 99mTc-PSMA imaging probe. The study protocol was approved by the local institutional ethics committee for human biomedical trials at the University of Szeged (license no. 229/2017-SZTE, date of approval November 20, 2017). The imaging data were acquired at the University of Szeged, in Hungary. Four healthy men clinically free from any malignant disease were enrolled in the dosimetry study. Ten patients with newly diagnosed PCa were enrolled in the biodistribution study. All patients provided oral and written consent after receiving detailed information of the study and agreed to the collection of data. The analysis was conducted at the University of Szeged in Hungary and at the University of California in Los Angeles, California (material transfer agreement MTA2020-00000538).
Synthesis and Quality Control of 99mTc-PSMA I&S
Synthesis of Mas3-y-nal-k(Sub-KuE) peptide-lyophilisate has been previously reported (2). 99mTc-pertechnetate was obtained from a 99Mo/99mTc generator. A single-dose freeze-dried kit contains 25 μg of peptide. Radiolabeling was performed with 5.87–7.53 GBq of 99mTc-pertechnetate. Radiochemical purity analysis was performed by instant thin-layer chromatography medium paper impregnated with a silica gel. As a solvent, we used methyl ethyl ketone. Radiochemical purities were in all cases greater than 95%.
Image Acquisition
A hybrid imaging method was used to determine the dosimetry of 99mTc-PSMA I&S: multiple-time-point whole-body (WB) planar imaging and a single quantitative SPECT/CT scan. In all healthy subjects (n = 4), WB anterior and posterior scintigraphy was performed at 1, 2, 3, 6, and 24 h after radiopharmaceutical administration (Fig. 1) using a triple-head γ-camera (AnyScan Trio SPECT/CT; Mediso Medical Imaging Systems Ltd.), equipped with low-energy, high-resolution collimators. The scanning speed was 18 cm/min, a matrix size of 256 × 1,024 pixels was used, and a symmetric 20% window was set at 140 keV. In all volunteers and PCa patients (n = 14), WB (mid thighs to vertex) SPECT/CT images were acquired at 6 h after radiopharmaceutical administration (Fig. 2). Quantitative SPECT images were acquired using a 128 × 128 matrix with a 20% energy window centered at 140 keV with adjacent scatter correction windows. A total of 96 projection views were acquired over 360° in 3.75° steps at 10 s per view. The number of bed positions was 3. Reconstruction of raw SPECT data was performed using the iterative Tera-Tomo (Mediso Medical Imaging Systems Ltd.) software, which is based on the order of sets and subsets (48 iterations/4 subsets) method. CT-based attenuation correction and point spread function correction were used. CT images were acquired using low-dose CT (120 keV, 100 mAs, 1.5 pitch factor, and 2.5 mm slice thickness). To improve the visibility of the gastrointestinal tract, Macrogol 1500 (50 g/L) (Molar Chemicals Ltd.) was administered orally 1 h before SPECT/CT imaging.

Example of source organs and background ROIs in a healthy volunteer (patient 003) on planar scintigraphy images (A); WB anterior and posterior 99mTc-Mas3-y-nal-k(Sub-KuE) scintigraphy was performed at 1, 2, 3, 6, and 24 h after injection (A–E).

(A) Example of organ delineation in healthy/PCa patient (patient 003) on SPECT/CT images. (B) 99mTc-PSMA I&S SPECT 3-dimesional maximum-intensity projection.
Determination of Absorbed Doses
The source organs consisted of the salivary glands, kidneys, liver, small intestine, large intestine, spleen, urinary bladder, and the body remainder. Source organ contours and appropriate background regions of interest (ROIs) were delineated manually on the anterior and posterior WB images at 1 h after injection (Fig. 1). All ROIs were manually relocated on the subsequent images and were validated by 2 experienced nuclear medicine physicians.
The mean counts were obtained for each organ and background ROI. Background-corrected organ counts were then calculated (based on the number of pixels from the organ ROI) for both anterior and posterior WB images. The geometric mean count was determined for every organ from the background-corrected anterior and posterior counts.
Source organ volumetric contours were delineated manually on CT images. The volumes of interest (VOIs) were transferred to the registered quantitative SPECT scans to determine the activity inside the source organs at 6 h after injection (Fig. 2). The fraction of injected activities were determined at each time point using the geometric mean counts from the planar images and the activity from the SPECT images.
The time–activity-curves were fitted with a mono- or biexponential function using the Levenberg-Marquardt–based algorithm and were generated for every source organ.
Absorbed doses for the target organs were estimated based on the RAdiation Dose Assessment Resource (RADAR, www.doseinfo-radar.com) scheme using the equation  , where DT is the dose of a given target organ, NS is the number of disintegrations that occur in a source organ, and DF is the dose factor, which gives the absorbed dose in a target per disintegration in a source (5). Integration of the time–activity curve was calculated for every source organ. Patient-specific volumes were used for the liver, kidneys, small intestines, spleen, salivary glands, and body remainder mass determination.
, where DT is the dose of a given target organ, NS is the number of disintegrations that occur in a source organ, and DF is the dose factor, which gives the absorbed dose in a target per disintegration in a source (5). Integration of the time–activity curve was calculated for every source organ. Patient-specific volumes were used for the liver, kidneys, small intestines, spleen, salivary glands, and body remainder mass determination.
In a second step, the curve-fitting and dose calculations were performed using OLINDA/EXM software (version 2.0; Hermes Medical Solutions), for comparison and method validation. For each volunteer, the non–decay-corrected percentage injected activity in the source organs at each time point was used to generate time–activity curves. The same patient-specific volumes were used as in the manual method. Biexponential curve-fitting in OLINDA/EXM version 2.0 was used to fit the time–activity curves. The individual volunteer dose reports were compiled as mean ± SD. Effective dose calculations were done using tissue-weighting factors according to recommendations of the International Commission on Radiological Protection (6).
Biodistribution in PCa Patients
The PROMISE miTNM scoring system was used to report the scan findings (7). Tumor, bladder, and intestine volumetric contours were manually delineated on the SPECT/CT images (+6 h) by 2 experienced nuclear medicine physicians. A background VOI with the same size as the tumor VOI was placed on gluteal muscles to quantify muscle background uptake. Using patient weight, injected activity, and 99mTc camera calibration factor, we calculated the SUVs as follows: SUVmean (g/mL) = (total radioactivity/volume of VOI)/(injected radioactivity/body weight) and SUVmax (g/mL) = (maximum radioactivity/volume of VOI)/(injected radioactivity/body weight). TBRs were calculated as follows: tumor/muscle (T/M, tumor SUVmax/muscle SUVmean), tumor/bladder (T/B, tumor SUVmax/bladder SUVmean), and tumor/intestine (T/I, tumor SUVmax/intestine SUVmean) ratios.
Statistics
Descriptive statistics were used (median, mean, range). The Wilcoxon signed-rank test was used to compare the doses obtained with the 2 methods.
RESULTS
Patients
Patients were enrolled from December 14, 2017, to November 14, 2018. In the dosimetry cohort of healthy volunteer men (n = 4), the median age was 66 y (range: 57–70 y), and the median weight was 88 kg (range: 83–95 kg) (Table 1). In the biodistribution cohort of patients with newly diagnosed PCa (n = 10), the median age was 67 y (range: 63–74 y), and the median weight was 88 kg (range: 54–130 kg) (Table 1). The median prostate-specific antigen (PSA) was 10.1 ng/mL (range: 0.34–44.3 ng/mL). The number of patients with a PCa disease Gleason score of 6, 7, 8, 9, and 10 was 1 (10%), 5(50%), 1 (10%), 1 (10%), and 2 (20%), respectively.
Patients Characteristics
Radiation Dosimetry in Healthy Volunteers
The median injected activity of 99mTc-PSMA I&S was 739 MBq (range: 562–828 MBq). No adverse events related to the injection of 99mTc-PSMA I&S were reported. 99mTc-PSMA I&S uptake was observed mainly in the salivary glands, liver, kidneys, spleen, small intestine, large intestine, and urinary bladder. Figure 3 depicts an example of time–activity curves of normal organs in a healthy volunteer (patient 003). Absorbed and effective doses using the manual RADAR and OLINDA/EXM methods are presented in Table 2. Detailed fitting parameters are presented in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).

Time–activity curves of normal organs in a healthy volunteer (patient 003).
Organ Absorbed and Effective Doses of 99mTc-Mas3-Y-nal-k(Sub-KuE) Using Manual RADAR and OLINDA/EXM 2.0 Methods
When the OLINDA/EXM method was used, the mean absorbed dose (mGy/MBq) was the highest in the kidneys (0.0733 mGy/MBq) followed by the salivary glands (0.0221 mGy/MBq), the adrenals (0.0217 mGy/MBq), the liver (0.0123 mGy/MBq), the spleen (0.0119 mGy/MBq), and the small intestine (0.0119 mGy/MBq). Total-body effective doses of the 4 volunteers were: 0.0053 (patient 001), 0.0048 (patient 002), 0.0051 (patient 003), and 0.0055 (patient 004) mSv/MBq. The average total-body effective dose was 0.0052 mSv/MBq. When the injected activities (range: 562–828 MBq) were considered, the effective doses of the 4 volunteers were between 3.11 and 4.23 mSv.
When the manual RADAR method was used, the effective doses of the 4 volunteers were: 0.0052 (patient 001), 0.0056 (patient 002), 0.0053 (patient 003), and 0.0059 (patient 004) mSv/MBq, with an average effective dose of 0.0055 mSv/MBq. When the injected activities (range: 562–828 MBq) were considered, the effective doses of the 4 volunteers were between 3.33 and 4.42 mSv. Between methods, the dose values were very similar; the largest difference observed in mean effective dose was for the liver (9.5% difference), except gastrointestinal tract, which was defined differently in the 2 methods. There was no statistically significant difference between the paired mean effective doses (mSv/MBq) obtained by the 2 methods (paired Wilcoxon signed-rank test, P > 0.05, lower large intestine/upper large intestine and left/right colon were excluded).
Biodistribution Study in Patients with Prostate Cancer
The median injected activity of 99mTc PSMA I&S was 695 MBq (range: 553–821 MBq). No adverse events related to the injection of 99mTc-PSMA I&S were reported. High uptake of 99mTc-PSMA I&S was observed 6 h after injection both in primary tumors (10/10 patients [100%], mean SUVmax: 13.37 [range: 3.25–44.00]), and in metastatic lesions (3/10 patients [30%], mean SUVmax: 5.71 [range: 1.80–8.48]) (Table 3). The mean T/M ratio, T/B ratio, and T/I ratio in the primary tumors was 30.22 (range: 7.95–110.00), 1.59 (range: 0.11–7.02), and 5.56 (range: 0.96–16.30), respectively, and in the metastasis 14.97 (range: 5.29–24.23), 0.60 (range: 0.33–0.92), and 3.16 (range: 1.20–4.82), respectively. Figure 4 shows pathologic tracer uptake in primary PCa (patient 012) and in patients with metastases in bone (patient 011) and LNs (patient 014). On the basis of the SPECT counts, the average activity of the pathologic lesions 6 h after tracer injection was 0.16 MBq (range: 0.01–0.96 MBq). On the basis of the physical half-life of 99mTc, the average lesion activity after 24 and 48 h was estimated to be 19.73 kBq (range: 1.25–120.00 kBq) and 1.23 kBq (range: 0.08–7.55 kBq), respectively.

Low-dose CT (A) and 99mTc-PSMA SPECT/CT (B) images of a PCa primary tumor lesion (patient 012) with high TBR (SUVmax: 22.00, TBR: 42.30 [arrowheads]). Low-dose CT (C) and 99mTc-PSMA SPECT/CT (D) images of a PCa bone metastasis (patient 011) with high TBR (SUVmax: 11.89, TBR: 25.85 [arrowheads]). Low-dose CT (E) and 99mTc-PSMA SPECT/CT (F) images of PCa LN metastases (patient 014) with high TBR (SUVmax: 8.23, TBR: 23.51 and SUVmax: 8.48, TBR: 24.23 [arrowheads]).
Biodistribution Study of 99mTc-PSMA I&S in Patients with PCa
DISCUSSION
Herein we report the radiation dose deposition of 99mTc-PSMA I&S in organs of 4 healthy volunteer patients with a hybrid imaging method (multiple sequential time-point planar imaging and a single SPECT/CT). Radiation dosimetry analysis is required for further clinical translation and approval by regulatory agencies. The average effective whole-body dose for administration of 700 MBq of 99mTc-PSMA I&S was 3.63 ± 0.64 mSv (OLINDA/EXM). The mean effective dose of 99mTc-PSMA I&S (0.0052 mSv/MBq) is similar to conventional 99mTc- MDP (8) used in SPECT/CT scans (0.004 mSv/MBq).
Several other 99mTc-PSMA compounds have been developed including, among others, Tc-EDDA/HYNIC-iPSMA (9), 99mTc-tricarbonyl-iPSMA (10), 99mTc-MIP-1404, and 99mTc-MIP-1405 (11). In comparison with currently available Tc-labeled PSMA inhibitors, the effective dose of 99mTc-PSMA I&S (0.0052 mSv/MBq) is similar to 99mTc-EDDA/HYNIC-iPSMA (0.0046 mSv/MBq) and lower than 99mTc-MIP-1404 (0.0088 mSv/MBq) and 99mTc-MIP-1405 (0.0079 mSv/MBq) agents. The radiation-absorbed dose of 740 MBq of 99mTc PSMA I&S in the liver (9.10 mSv) was lower than that of 99mTc-EDDA/HYNIC-iPSMA (liver = 10.73 mSv); however, the small intestine (8.83 mSv), spleen (8.83 mSv), kidneys (54.24 mSv), and salivary glands (16.35 mSv) had higher doses than 99mTc-EDDA/HYNIC-iPSMA (small intestine = 2.42 mSv, spleen = 7.06 mSv, kidney = 28.80 mSv, salivary glands = 9.69 mSv) (9). In comparison to the PET tracers, the effective dose of 99mTc-PSMA I&S is lower than 68Ga-labeled (68Ga-PSMA-11 (0.0236 mSv/MBq (12)) and 18F-labeled (0.0220 mSv/MBq (13)) PSMA-targeted tracers.
The dose calculation and verification using OLINDA/EXM (version 2.0) software contained the same main steps. The largest difference was in the exponential curve-fitting method: OLINDA was used for biexponential curve fitting in every case, whereas the manual method used mono- or biexponential fitting, based on visual assessment. As shown in Figure 3, there were cases when the monoexponential fit was adequate (liver, spleen, remainder of body by visual inspection). Therefore, there were only minor differences in the calculated number of disintegrations of source organs between both methods. Another difference was the segment definition of the gastrointestinal tract: RADAR contains dose factors for the upper large intestine and lower large intestine, whereas OLINDA/EXM calculates doses to the left and right colon.
Detailed biodistribution data for 99mTc-PSMA I&S has been published by Robu et al. (2). Relatively high blood and background activity were observed due to the high plasma protein binding of the radiopharmaceutical (94%). 99mTc-PSMA I&S is excreted primarily by the urinary system, although increased lipophilicity of the tracer enhanced liver uptake and produced a higher constant rate of hepatobiliary clearance, which led to increased intestinal activity. In our study, intestinal tracer accumulation was found to be highly variable as well as bladder activity.
Both SPECT/CT imaging systems and SPECT tracers are more affordable than PET/CT systems. 99mTc-PSMA I&S can represent a valuable alternative to PSMA PET imaging in countries in development. Another potential application of 99mTc-PSMA I&S is RGS. PSMA-targeted RGS can help guide urologists to detect PCa LN metastasis during surgery. PSMA-expressing LNs can be detected intraoperatively using a γ-probe. Despite the use of PSMA-targeted PET as a tool for preoperative guidance, intraoperative detection and resection of small lesions remains challenging, especially because of the small dimension of the LN metastasis, the technical difficulty of pelvic LN dissection, and atypical anatomic localization of the LNs. Farolfi et al. reported that in up to two thirds of patients who experienced disease recurrence after surgery, at least 1 lesion had already been detected on the preoperative PSMA-targeted PET imaging, suggesting that LN dissection was often not complete (14). PSMA-targeted RGS might increase a surgeon’s confidence in intraoperative detection and complete dissection of metastatic LNs lesions detected in the preoperative PSMA-targeted SPECT and PET imaging. European retrospective studies conducted in large cohorts reported high rates of intraoperative tumor detection validated by histopathology, as well as improved treatment outcome (3,4). Of note, a first European clinical trial is currently investigating the feasibility of PSMA-targeted RGS (TRACE: NCT03857113).
The timing of tracer administration for RGS has been determined empirically and may be improved. In this cohort, the activity in the target lesions of between 24 and 48 h after injection remains in the detectable range for commercially available γ-probes. The minimum acceptable sensitivity of a γ-probe system sensitivity for clinical use is 2.5 cps/kBq (15). Therefore, the γ-probe could detect the tumors between 24 and 48 h after tracer administration. Even though 99mTc-PSMA I&S showed good TBR in both primary and metastatic lesions, differentiation between pathologic and physiologic uptake can be difficult because of the urinary and intestinal tracer accumulation. On the basis of our TBRs, tumor differentiation from the intestine seems to be easier than from the bladder on the SPECT/CT at more than 6 h. However, after 24 h, a lower activity is expected due to urinary and intestinal elimination in contrast with the stable tumor uptake.
CONCLUSION
This dosimetry study of 99mTc-PSMA I&S showed that injected activities of 562–828 MBq translate to estimated effective doses of 3.33–4.42 mSv (manual RADAR method) and 3.11–4.23 mSv (OLINDA/EXM method), which is similar to the effective doses from other 99mTc-PSMA inhibitors. Preliminary data suggest high TBR of primary and metastatic PCa lesions. Larger trials are needed to further define its capabilities in the management of PCa.
Disclosure
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the radiation dosimetry and biodistribution of 99mTc-PSMA I&S?
PERTINENT FINDINGS: On the basis of a hybrid method using serial planar γ-imaging and a SPECT/CT scan acquired in 4 healthy volunteers, the average effective whole-body dose estimation for administration of 700 MBq of 99mTc-PSMA I&S was 3.64 mSv, which is comparable to other 99mTc-based tracers.
IMPLICATIONS FOR PATIENT CARE: This study provides required data for translation and approval of 99mTc-PSMA I&S by regulatory agencies.
Footnotes
↵* Contributed equally to this work.
Published online December 4, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 15, 2020.
- Accepted for publication November 16, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}