


Abstract
Accurate grading of patients with neuroendocrine neoplasms (NENs) is essential for risk stratification and optimal choice of therapy. Currently, grading is based on histologically assessed degree of tumor proliferation. The aim of the present study was to assess the long-term prognostic value of 18F-FDG PET imaging for risk stratification of NENs and compare it with tumor grading (World Health Organization 2010 classification). Methods: We conducted a prospective cohort study evaluating the prognostic value of 18F-FDG PET imaging and compared it with histologic grading. Enrolled were 166 patients of all grades and with histologically confirmed NENs of gastroenteropancreatic origin. The primary endpoint was overall survival (OS). Progression-free survival (PFS) was a secondary endpoint. In addition, OS in relation to peptide receptor radionuclide therapy (PRRT) was analyzed as an exploratory endpoint. The median follow-up time was 9.8 y. Results: Analysis of the whole cohort revealed that a positive 18F-FDG PET scan was associated with a shorter OS than a negative 18F-FDG PET scan (hazard ratio: 3.8; 95% CI: 2.4–5.9; P < 0.001). In G1 and G2 patients (n = 140), a positive 18F-FDG PET scan was the only identifier of high risk for death (hazard ratio: 3.6; 95% CI, 2.2–5.9; P < 0.001). In multivariate analysis, 18F-FDG PET, G3 tumor, ≥2 liver metastases, and ≥2 prior therapies were independent prognostic factors for OS, and 18F-FDG PET, G3 tumor, and ≥3 liver metastases were independent prognostic factors for PFS. For patients receiving PRRT, 18F-FDG–negative cases had a significantly longer survival than 18F-FDG–positive cases, whereas no difference was identified for tumor grading. 18F-FDG–positive patients receiving PRRT had a significantly longer median survival than patients not receiving PRRT (4.4 vs. 1.4 y, P = 0.001), whereas no difference was seen for 18F-FDG–negative patients. Conclusion: 18F-FDG PET is useful for risk stratification of all NEN grades and is superior to histologic grading. 18F-FDG PET could differentiate G1 and G2 tumors into low- and high-risk groups. In the selection of therapy and for risk stratification of NEN patients, 18F-FDG PET status should be considered.
- 18F-FDG PET
- neuroendocrine tumors
- prognosis
- Ki-67
- prospective study
- peptide receptor radionuclide therapy (PRRT)
Grading of neuroendocrine neoplasms (NENs) is essential for risk stratification and optimal selection of therapy regime, yet it is a great challenge. In the World Health Organization (WHO) 2010 classification, grading relies on degree of tumor proliferation (1–3), and accordingly NENs are divided into grade 1 (G1) (Ki-67 ≤ 2%), grade 2 (G2) (Ki-67 3%–20%), and grade 3 (G3) (Ki-67 > 20%). The immunohistochemical assessment of the percentage of cells proliferating (Ki-67 index) is determined in hotspot areas of resected tumors or biopsies. However, intratumoral and, in the case of disseminated disease, intrapatient heterogeneity in tumor phenotype can easily introduce an erroneous interpretation of disease aggressiveness (4,5). Low- and intermediate-grade tumors (G1 and G2) are particularly challenging to risk stratify. Even if metastatic, some grade 1 and 2 patients have stable disease for years (6). Other G1 and G2 tumors rapidly progress. To aid a more accurate and personalized selection of treatment and to improve risk stratification, new approaches are therefore warranted (7).
PET using the glucose analog 18F-FDG is well established as a functional imaging modality for staging (8,9) and for determination of metabolic response to anticancer therapy (10). 18F-FDG PET is also useful for prediction of prognosis and thereby for risk stratification in several cancer forms (11,12). However, it is currently not routine in the clinical management of NENs.
We have previously shown that imaging with 18F-FDG PET is a promising tool for the assessment of tumor aggressiveness at the whole-body level in NEN patients (13). Although previously considered of little relevance, the recent awareness of the prognostic utility of 18F-FDG PET in the assessment of NENs (14,15) may suggest an important role for 18F-FDG PET imaging for prognostic evaluation and risk stratification in these patients (16).
The aim of this prospective cohort study of 166 NEN patients was to assess and compare with histologic grading the long-term prognostic value of 18F-FDG PET in terms of overall survival (OS) and progression-free survival (PFS).
MATERIALS AND METHODS
Patients
All patients were recruited from Rigshospitalet, Denmark, which is a third-line referral hospital and center for treatment of patients with NENs. Eligible patients were diagnosed with NEN of gastroenteropancreatic (GEP) origin, were 18 y or older, and had measurable disease. All histopathologic diagnoses were performed at Rigshospitalet. Exclusion criteria were pregnancy, lactation, or claustrophobia. Patient demographics and clinical characteristics are listed in Table 1.
Patient Characteristics for 18F-FDG–Negative and 18F-FDG–Positive Groups
Design
A prospective cohort study design evaluating the prognostic value of 18F-FDG PET was used. The study was approved by the regional scientific ethical committee (KF-01-313726 and H-3-2011-092). All patients were part of previously published studies (13,17). Written informed consent was obtained from all patients. Patients were consecutively recruited between 2007 and 2013. All aspects of patient care and treatment were performed at the discretion of the treating clinicians and according to routine procedures of the department. Treating clinicians were masked to the 18F-FDG PET results, and the 18F-FDG PET results were not used for treatment decisions. A total of 838 follow-up years were available at the end of the study.
The primary endpoint was OS, with PFS as secondary endpoint. For assessment of PFS, half-yearly or yearly routine follow-up CT scans were used and evaluated according to RECIST 1.1 (18). The CT scan closest to and before the 18F-FDG PET scan was used as baseline. Time to progression was calculated as the time from the 18F-FDG PET scan until tumor progression as assessed on CT scans.
Retrospectively, data regarding peptide receptor radionuclide therapy (PRRT) were analyzed in relation to 18F-FDG result and tumor grading.
Immunohistochemical Evaluation of Proliferation Index
Grading of tumors was based on proliferation index with immunohistochemical staining for the proliferation marker Ki-67. Tumors were graded according to the WHO 2010 criteria (19). The Ki-67 index was scored according to guidelines with counting the numbers of proliferating cells in hotspot areas. In patients with more than one Ki-67 assessment, the one closest to and before the 18F-FDG PET scan was chosen.
18F-FDG PET/CT
Patients were instructed to fast for 6 h before the 18F-FDG injection, and blood glucose levels were measured to ascertain euglycemia (<8 mmol/L). PET/CT images were acquired at 1 h after injection of 353 (range, 131–467) MBq of 18F-FDG. An expert board-certified specialist in nuclear medicine analyzed all images. An expert board-certified specialist in radiology analyzed all diagnostic CT scans. From December 2011, the CT scan was changed from a low-dose CT to a diagnostic CT scan. CT data were used for attenuation correction.
Statistics
For the analysis of the prognostic value of 18F-FDG PET, OS and PFS were chosen as endpoints. PFS was defined as the time from 18F-FDG PET acquisition to progression or disease-related death, and OS was defined as the time from 18F-FDG PET acquisition to death by any cause, as recommended by the European Organization for Research and Treatment of Cancer guidelines (18,20).
Survival probability and PFS were estimated using the method of Kaplan and Meier (21) and differences between groups analyzed by the log-rank test. Hazard ratios (HRs) were calculated using the Cox proportional hazards regression model. Multivariate analyses were performed using the Cox proportional hazards regression analysis, entering 18F-FDG result, WHO grade, metastatic status, tumor origin, number of prior therapies (0–1 vs. 2 or more), and number of liver metastases (0, 1, 2, ≥ 3, respectively) in the models for OS and PFS. All data analyses were performed using IBM SPSS statistics version 25.0 (SPSS Inc.). A P value of less than 0.05 was considered significant.
RESULTS
A total of 166 patients from a single center with histologically proven GEP-NEN fulfilled the inclusion criteria and underwent an 18F-FDG PET/CT scan (patient demographics are summarized in Table 1). Most included patients had advanced disease and had received NEN-related treatment (144/166; 87%), including 64 (39%) who had received 3 or more treatment regimens. Surgery was performed in 85 patients (40 G1, 36 G2, 7 G3, and 2 of unknown grade), and there was a tendency for more G1 patients undergoing operations with curative intent than G2 and G3 (33 vs. 21 and 4, respectively, Pearson χ2: P = 0.054). There was no significant difference in 18F-FDG–positive versus 18F-FDG–negative patients undergoing operations with curative intent (20 vs. 40 cases, Fishers exact test: P = 0.227). Metastases were identified in 152 patients (92%), of whom 107 (64%) had liver metastases and 16 had bone metastases (10%). The time between the histopathologic diagnosis and the 18F-FDG scan was on average 39 mo (range, −0.8 to 324 mo).
The estimated median follow-up time was 9.8 y, calculated according to the reverse Kaplan–Meier method (22). At the end of follow-up on February 28, 2018, the remaining cases were censored, and at that point 95 of the 166 enrolled patients had died. Median OS time for the whole cohort was 6.3 y (95% CI, 5.0–7.5 y), and PFS time was 2.6 y (95% CI: 1.9–3.2) from baseline (Table 2).
Survival Analysis for the Whole Cohort
Pathologic foci were found on 18F-FDG PET scans in 90 patients (54.2%). Fifteen of the 16 G3 cases (94%) were read as 18F-FDG–positive. There were 140 patients belonging to G1 or G2, and of these, 69 cases (49%) were 18F-FDG–positive.
Risk Stratification Based on 18F-FDG PET Results
For the 166 enrolled patients, OS was significantly better for 18F-FDG–negative when compared with 18F-FDG–positive patients (HR = 3.8; P < 0.001; Fig. 1A and Table 2). PFS was also significantly better for 18F-FDG–negative cases than 18F-FDG–positive cases (HR = 2.5; P < 0.001; Fig. 1A and Table 2). To analyze the prognostic power of 18F-FDG PET for the most challenging subjects (G1 and G2, n = 140), we also performed analysis after excluding G3 tumors. Again, OS was better in the 18F-FDG–negative group than the 18F-FDG–positive group (HR = 3.6; P < 0.001; Fig. 1B and Table 3) and so was PFS (HR = 2.6; P < 0.001; Fig. 1B and Table 3).

Risk stratification of NEN patients based on 18F-FDG PET results. PFS (A and B, left) and OS (A and B, right) are shown for all patients (A) and G1 and G2 patients (B).
Survival Analysis for G1 and G2 Groups
Patients with a negative 18F-FDG PET reading had an estimated 5-y OS rate of 79% in comparison to 35% for 18F-FDG–positive patients from the time of PET scanning. Likewise, 49% of 18F-FDG–negative patients were progression-free at 5-y in comparison to 18% of the 18F-FDG–positive patients. At the end of follow-up, 27 18F-FDG–negative patients (36% of negatives) had died compared with 68 18F-FDG–positive patients (76% of positives).
In the 140 NEN patients of WHO G1 and G2, 25 18F-FDG–negative patients had died (35% of negatives) compared with 50 18F-FDG–positive patients (72% of positives). Of these 50 18F-FDG–positive events, 17 were classified as G1 and 33 as G2.
Risk Stratification Based on WHO Grading and Comparison to 18F-FDG PET
On the basis of available histologic information, we analyzed the difference in outcome based on the WHO 2010 grading, which scored 57 cases as G1, 83 as G2, and 16 as G3 tumors while 10 patients had unsettled proliferation index due to lack of tumor samples. Thus, in total 156 patients were included in this analysis.
The Kaplan–Meier analysis found the OS to be shorter in G3 than in both G1 (HR = 11.1; P < 0.001) and G2 (HR = 9.7; P < 0.001) (Fig. 2A and Table 2). PFS was also shorter in G3 than in both G1 (HR = 11.9; P < 0.001) and G2 (HR = 8.2; P < 0.001) (Fig. 2A and Table 2). However, when analyzing the prognostic power of WHO grading for the most challenging patients (G1 and G2), there were no significant differences in outcome either in terms of OS (HR = 1.3; P = 0.224) or in terms of PFS (HR = 1.2; P = 0.391) between G1 and G2 patients (Fig. 2A).

Risk stratification of NEN patients based on histology scoring. PFS (A and B, left) and OS (A and B, right) are shown. Results are dichotomized based on WHO grading (A) and Ki-67 score of 5% (B).
Next, for the 140 patients of G1 or G2, we analyzed whether a stratification based on a proliferation index cutoff of 5% instead of 2% was better for prediction of outcome. On the basis of this altered cutoff for G1 or G2, it was possible to better risk stratify patients both in terms of OS (HR = 1.7; P = 0.024) and in terms of PFS (HR = 1.6; P = 0.016) (Fig. 2B).
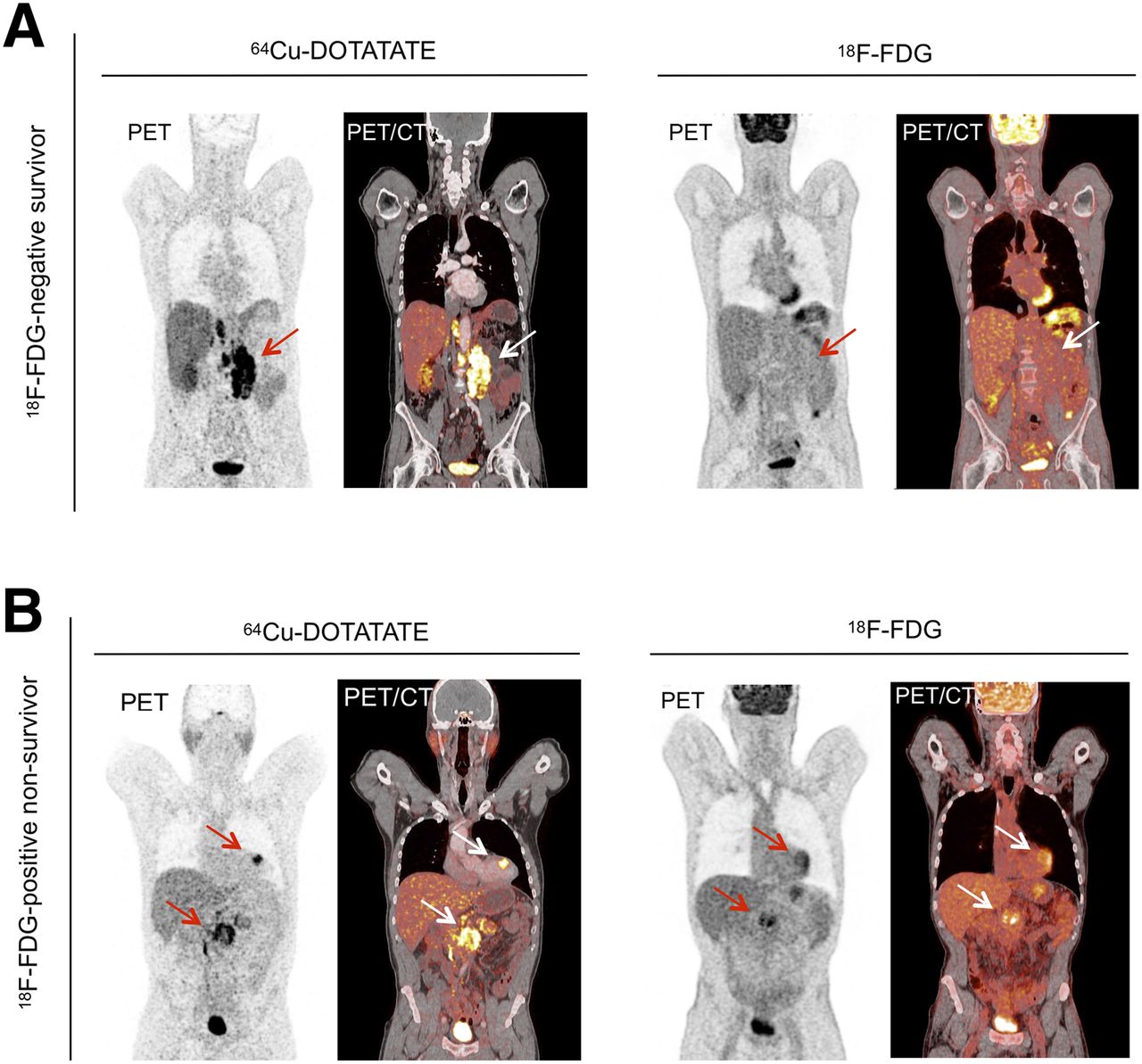
The estimated 5-y OS rates from the time of 18F-FDG PET scans were 67%, 58%, and 0% for G1, G2, and G3, respectively. Likewise, the 5-y PFS rates were 42%, 29%, and 0% for the 3 grading groups, respectively. At the end of follow-up, 31 of 57 G1 (54%), 44 of 83 G2 (53%), and all 16 G3 patients (100%) had died. Imaging results for 2 patients with G2 tumors are shown in Figure 3.
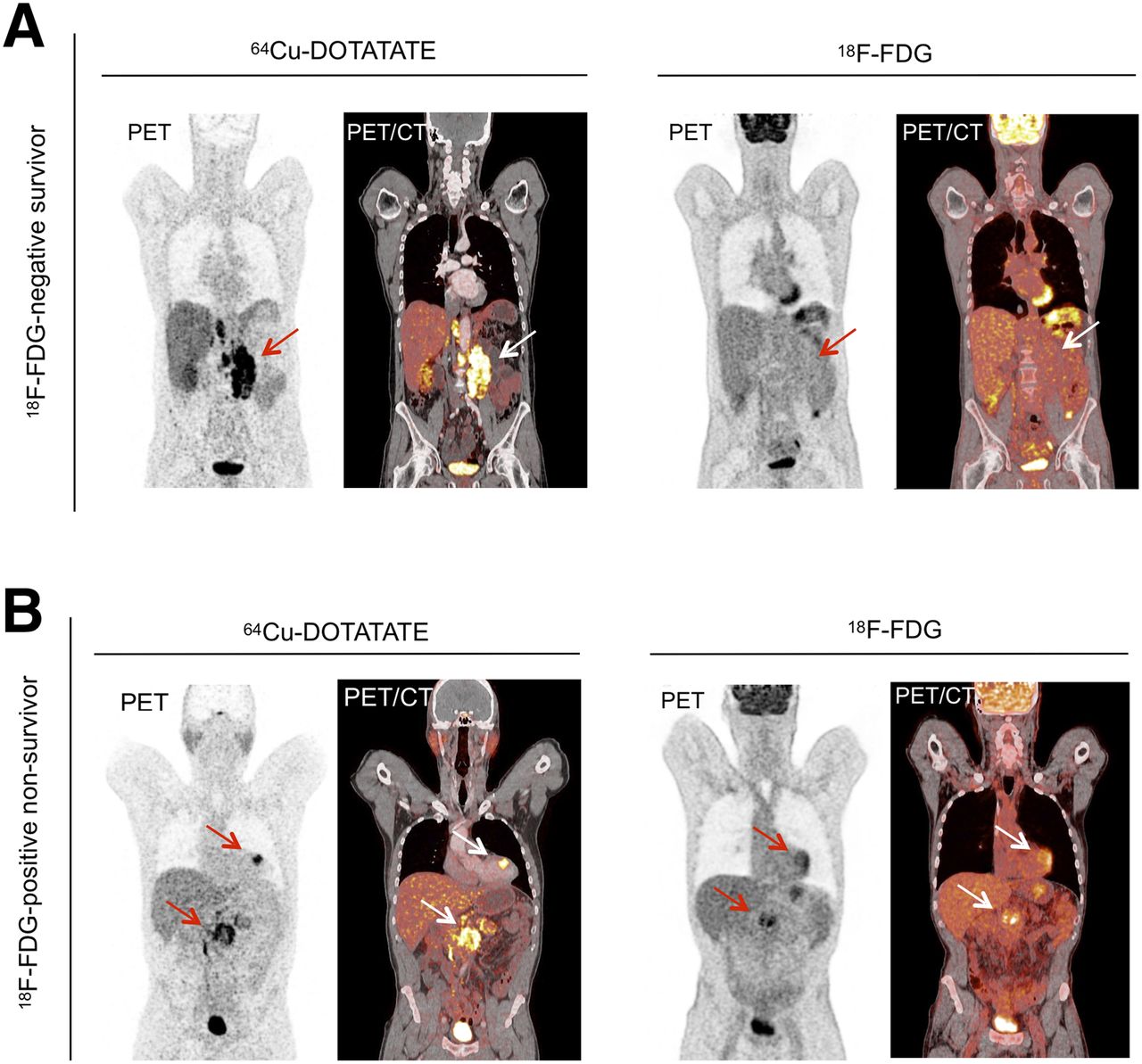
Examples of 18F-FDG PET and somatostatin receptor imaging results for patient (A) with G2 NEN tumor, Ki-67 index of 14%, a positive 64Cu-DOTATATE reading (left), and a negative 18F-FDG PET reading (right), and alive at the end of follow-up (73 mo after 18F-FDG PET scan). (B) Patient with G2 NEN, Ki-67 index of 5%, a positive 64Cu-DOTATATE reading (left), a positive 18F-FDG PET reading (right), and dead 18 mo after 18F-FDG PET scan. Arrows indicate location of tumors.
Multivariate Cox regression analysis revealed that 18F-FDG, G3, 2 or more prior therapies, and 2 or more liver metastases were independent prognostic factors for OS whereas G1 versus G2, metastatic status, and tumor origin were not prognostic. 18F-FDG result, G3, and 3 or more liver metastases were independent prognostic factors for PFS, whereas G1 versus G2, metastatic status, tumor origin, and number of prior therapies were not prognostic factors.
Risk Stratification Based on Tumor Origin
Next, we evaluated the role of 18F-FDG PET and WHO 2010 grading for risk stratification of G1 and G2 NENs based on tumor origin. Enrolled in these analyses were 87 cases of small intestinal origin and 28 of pancreatic origin. These 2 locations were the most abundantly represented in our cohort.
In line with the whole cohort, 18F-FDG PET was able to risk-stratify both pancreatic and small intestinal NENs. This was the case both in terms of OS and in terms of PFS (Table 3). Again, WHO grading held little prognostic information, especially for NENs of small intestinal origin, but also failed to accurately risk stratify NENs of pancreatic origin (Table 3).
18F-FDG PET and PRRT
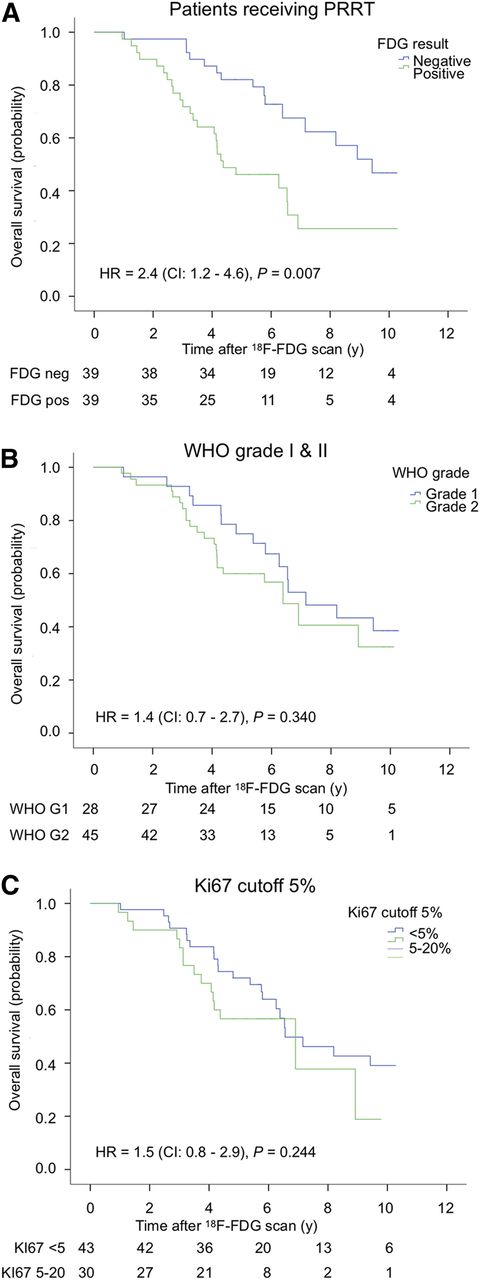
PRRT was given to 78 (47% of enrolled) patients, of whom 64 had undergone a pre-PRRT 18F-FDG PET scan. There were 39 18F-FDG–negative and 39 18F-FDG–positive cases. Of the 78 cases, PRRT was given to 28 with G1 tumors, 45 with G2 tumors, 3 with G3 tumors, and 2 with unknown tumor grade.
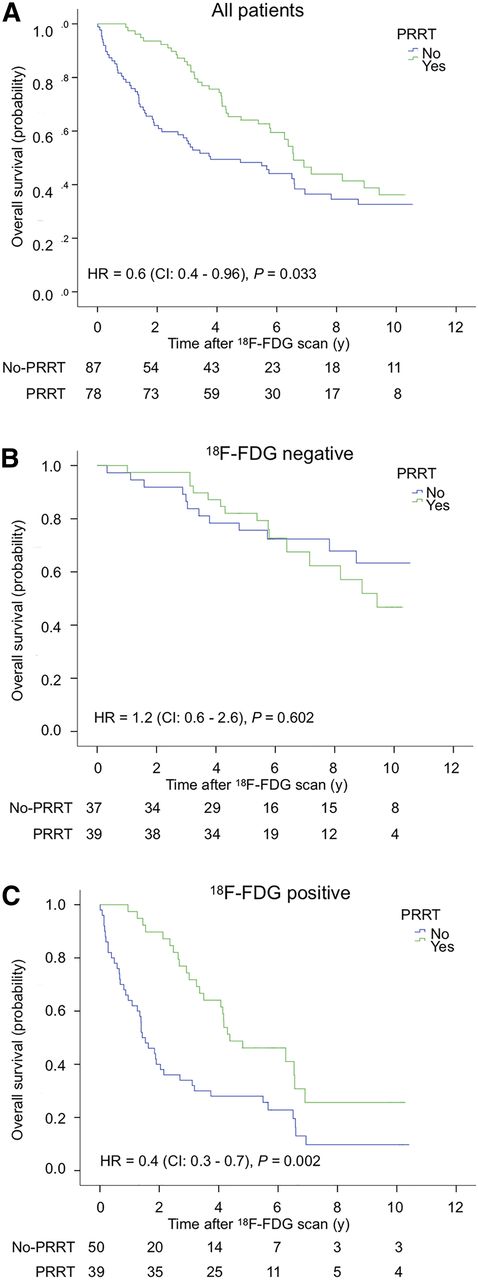
For patients receiving PRRT (Fig. 4), 18F-FDG–negative patients had a longer survival than 18F-FDG–positive patients. For all 18F-FDG–positive cases, survival was longer if patients had received PRRT compared with 18F-FDG–positive cases not receiving PRRT. In contrast, there was no significant difference in survival for 18F-FDG–negative patients receiving PRRT compared with 18F-FDG–negative patients not receiving PRRT (Fig. 5).
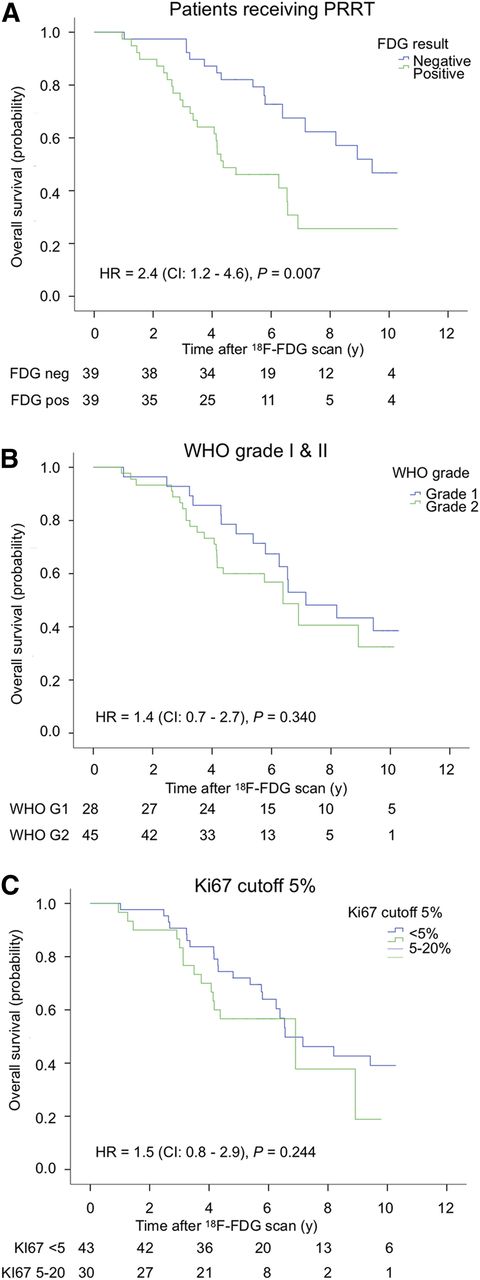
Kaplan–Meier curves for patients receiving PRRT, stratified by 18F-FDG status (A), by WHO grade (G1 vs. G2) (B), and by modified grading score (Ki-67 index < 5% vs. 5%–20%).

Kaplan–Meier curves for patients receiving PRRT vs. patients not receiving PRRT. All patients enrolled in the study (A), 18F-FDG–negative patients (B), and 18F-FDG–positive patients (C) stratified by PRRT status.
DISCUSSION
In this prospective cohort study, we found 18F-FDG PET to be most valuable and better than histologic grading for risk stratification of GEP-NENs. Patients with a positive 18F-FDG PET reading had a shorter OS and PFS than patients with a negative 18F-FDG PET, resulting in a 3-y longer median PFS time for 18F-FDG–negative patients (median OS for 18F-FDG–negative patients not reached). A G3 tumor was also associated with a shorter survival. However, in our cohort, risk stratification based on grading (WHO 2010 classification) was not possible for G1 and G2 NENs. We hereby confirm previous findings (7,23) that grading based on proliferation index cannot alone identify the patients with a poor prognosis in G1 and G2. In contrast, we found that 18F-FDG PET was able to discriminate patients G1 and G2 with poor outcome from those with better outcome both in terms of PFS and most notably also in terms of OS. 18F-FDG PET could also risk stratify both pancreatic and small intestinal NENs of G1 and G2 in contrast to WHO grading.
Our cohort of 166 patients, with the majority being G1 and G2 tumors, represents the largest cohort of GEP-NENs so far evaluated for the prognostic role of 18F-FDG PET in a prospective design. Our results here and previously (13,17) are in agreement with the few studies so far evaluating the role of functional metabolic imaging for risk stratification of NENs in different settings, but all confirming the value of adding 18F-FDG PET in the clinical workup of NENs (23–27).
The diagnostic sensitivity of 18F-FDG PET in NENs is as low as 50% (28), which we also confirmed in our cohort. This is reflected in a lower expression level of glycolytic markers in these tumors (29) and has limited its use in NENs. Moreover, other SPECT and PET tracers have a much higher diagnostic sensitivity, visualizing overexpressed tumor biomarkers (28,30–33), especially somatostatin receptors (34). However, because of the large proportion of GEP-NENs being 18F-FDG–negative, we were able to risk stratify patients solely based on negative and positive 18F-FDG results, which makes it an easily applicable prognostic tool and therefore also clinically implementable. We have previously evaluated other cutoffs for dichotomizing 18F-FDG PET in NENs and found no better cutoff than categorizing into positive and negative (13).
In an urge to better risk stratify G1 and G2 tumors, it has been proposed (7) that a cutoff of 5% may be better than the 2% currently used. In our cohort, the risk of death as well as disease progression was indeed lower in the Ki5 group (Ki-67 < 5%) than the Ki20 group (Ki-67 5%–20%). However, by multivariate survival analysis, entering histologically assessed (Ki-67) and metabolically assessed (18F-FDG PET) parameters, only 18F-FDG PET was an independent predictor of both OS and PFS regardless of the Ki-67 cutoff used. Moreover, we found that 31 of 57 (54%) patients scored as G1 died during follow-up and of these 31 events, 17 (55%) had 18F-FDG–avid tumors, confirming that a substantial part of high-risk patients when scored according to the WHO grading are missed, but could be identified by the implementation of an 18F-FDG PET scan.
18F-FDG PET in relation to PRRT revealed that 18F-FDG–negative patients had a longer survival after PRRT than 18F-FDG–positive patients, which was in agreement with recent findings (27). Approximately half of the enrolled patients in our cohort received PRRT, and in addition to a longer survival for the patients receiving PRRT, we also found that the survival benefit seemed most pronounced in the 18F-FDG–positive patients in whom the median survival time for those who received PRRT was 4.4 y compared with 1.4 y for patients not receiving PRRT. Our results indicate that there might be a greater survival benefit of PRRT for 18F-FDG–positive patient than 18F-FDG–negative patients, in whom we did not find any difference between PPRT receivers and nonreceivers. One could, therefore, speculate whether 18F-FDG PET could serve as a tool for selection of patients eligible for PRRT.
18F-FDG uptake is a composite measure of several factors including, but not limited to, proliferation. Tumor hypoxia, degree of neovascularization, and oncogenic pathway activation have all been proven as factors determining tumor aggressiveness and 18F-FDG uptake (35,36). The wide range in biologic phenotype poses a continuous challenge for selection of optimal treatment for cancer patients including NENs. Histologic scoring provides detailed information at a microscopic level about the proliferation potential of the investigated tumor samples but lacks information at a whole-body level concerning tumor heterogeneity and aggressiveness (37). Moreover, the method has limitations related to sampling errors and variability in scoring (5), and sequential tumor sampling for confirmation of progressive disease is often not feasible. In contrast, a PET scan can easily be implemented in both the initial assessment and in the follow-up of NEN patients and provides detailed prognostic information at the whole-body level. It can simultaneously assess the overall aggressiveness and heterogeneity of the disease. In addition, we have recently shown, by use of the proliferation tracer 3′-deoxy-3′-18F-fluorothymidine, that even at the whole-body level, assessment of proliferation does not surpass the prognostic information achieved by an 18F-FDG scan (17). Finally, 18F-FDG PET is available in all PET centers.
Although we demonstrated that 18F-FDG PET is a powerful prognostic tool surpassing current methods, only future studies can reveal if selection of treatment based on the 18F-FDG PET translate into prolonged survival for patients with NENs. In particular, it is of interest to see whether patients histologically assessed as low grade, who have a positive 18F-FDG PET scan, will benefit from a more aggressive treatment regimen.
CONCLUSION
We have demonstrated in a prospective study of a large group of GEP-NEN patients that 18F-FDG PET is a powerful prognostic tool of relevance for patients with all grades of NEN. In multivariate analysis, 18F-FDG PET, G3 tumor, ≥2 liver metastases, and ≥2 prior therapies were independent prognostic factors for OS. We suggest implementing 18F-FDG PET in the routine workup of NEN patients for improved clinical decision making and selection of therapy. In addition, 18F-FDG PET may be of relevance in selecting patients for PRRT.
DISCLOSURE
Research grants from the following funds are greatly acknowledged: The European Union’s Horizon 2020 research and innovation programme under grant agreements no. 670261 (ERC Advanced Grant) and 668532 (Click-It), the Lundbeck Foundation, the Novo Nordisk Foundation, the Innovation Fund Denmark, the Danish Cancer Society, Arvid Nilsson Foundation, Svend Andersen Foundation, the Neye Foundation, the Research Foundation of Rigshospitalet, the Danish National Research Foundation (grant 126), the Research Council of the Capital Region of Denmark, the Danish Health Authority, the John and Birthe Meyer Foundation and Research Council for Independent Research. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: What is the long-term prognostic value of 18F-FDG PET imaging for risk stratification of NENs?
PERTINENT FINDINGS: In a prospective cohort study, the prognostic value of 18F-FDG PET in 166 patients with NEN was evaluated. Patients with a positive 18F-FDG PET reading had a shorter OS and PFS than patients with a negative 18F-FDG PET, resulting in a 3-y longer median PFS for 18F-FDG–negative patients.
IMPLICATIONS FOR PATIENT CARE: Implementing 18F-FDG PET in the clinical workup of NENs would be useful for risk stratification and for selection of therapy.
Footnotes
Published online Oct. 16, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 20, 2020.
- Accepted for publication September 17, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Latest Advances in Peptide Receptor Radionuclide Therapy for Gastroenteropancreatic Neuroendocrine Tumors
- Prospective Phase II Trial of [68Ga]Ga-NODAGA-E[c(RGDyK)]2 PET/CT Imaging of Integrin {alpha}v{beta}3 for Prognostication in Patients with Neuroendocrine Neoplasms
- Prospective Phase II Trial of Prognostication by 68Ga-NOTA-AE105 uPAR PET in Patients with Neuroendocrine Neoplasms: Implications for uPAR-Targeted Therapy