


Visual Abstract

Abstract
Targeted therapies for multiple myeloma (MM) include the anti-CD38 antibody daratumumab, which, in addition to its inherent cytotoxicity, can be radiolabeled with tracers for imaging and with β- and α-emitter radionuclides for radioimmunotherapy. Methods: We have compared the potential therapeutic efficacy of β- versus α-emitter radioimmunotherapy using radiolabeled DOTA-daratumumab in a preclinical model of disseminated multiple myeloma. Multiple dose levels were investigated to find the dose with the highest efficacy and lowest toxicity. Results: In a dose–response study with the β-emitter 177Lu-DOTA-daratumumab, the lowest tested dose, 1.85 MBq, extended survival from 37 to 47 d but did not delay tumor growth. Doses of 3.7 and 7.4 MBq extended survival to 55 and 58 d, respectively, causing a small equivalent delay in tumor growth, followed by regrowth. The higher dose, 11.1 MBq, eradicated the tumor but had no effect on survival compared with untreated controls, because of whole-body toxicity. In contrast, the α-emitter 225Ac-DOTA-daratumumab had a dose-dependent effect, in which 0.925, 1.85, and 3.7 kBq increased survival, compared with untreated controls (35 d), to 47, 52, and 73 d, respectively, with a significant delay in tumor growth for all 3 doses. Higher doses of 11.1 and 22.2 kBq resulted in equivalent survival to 82 d but with significant whole-body toxicity. Parallel studies with untargeted 225Ac-DOTA-trastuzumab conferred no improvement over untreated controls and resulted in whole-body toxicity. Conclusion: We conclude, and mathematic modeling confirms, that maximal biologic doses were achieved by targeted α-therapy and demonstrated 225Ac to be superior to 177Lu in delaying tumor growth and decreasing whole-body toxicity.
Multiple myeloma (MM), a malignancy of fully differentiated plasma cells, is normally confined to the bone marrow compartment, although extramedullary malignancies are often observed. Approximately 30,000 new cases of MM, with over 12,000 deaths, occur per year (1). Daratumumab is a humanized anti-CD38 IgG1 antibody against the surface receptor CD38, which is highly expressed on MM plasma cells but also on natural killer cells and monocytes in MM patients. Daratumumab, either as a single agent or in combination with other agents, has yielded substantially favorable outcomes. Given the especially strong efficacy afforded by daratumumab with immunomodulatory drugs (lenalidomide and pomalidomide) (2–6), the use of daratumumab plus immunomodulatory drugs is now Food and Drug Administration–approved for advanced relapsed MM (2). The main anti-MM effect of daratumumab has thus far been attributed to its ability to target the MM cells via the immune system (7), but unfortunately, a subset of patients does not respond to the treatment, whereas others may experience disease progression within a few months. Even in patients experiencing a long-lasting response, resistance eventually occurs. Although CD38 is highly expressed in MM, patient response to this therapy is variable, with some patients developing resistance despite continued high expression of the CD38 antigen on MM cells (8), supporting the possibility that antigen loss is not necessarily a consideration in the design of daratumumab-based therapies, as we recently published (9).
Since CD38 is ubiquitously expressed on the myeloma cells independently of the line of therapy, and daratumumab is able to directly target myeloma cells in the bone marrow (10,11), it is anticipated that the addition of a therapeutic agent, such as a radionuclide, to daratumumab would dramatically increase its potency compared with the antibody alone, especially in patients whose disease is progressing under regimens containing daratumumab. In this respect, several groups have explored the use of α- and β-emitting radionuclides conjugated to anti-CD38 antibodies for improved therapy. Kang et al. showed that a diethylenetriamine pentaacetic acid–based chelate conjugate of daratumumab labeled with 177Lu, a β-emitter with a tissue path-length of about 2 mm, reduced tumor growth in a subcutaneous model of MM (12). Although β-emitter radionuclides have enjoyed some success in the treatment of disseminated diseases such as leukemia and lymphoma, they suffer from extensive bone marrow suppression, often the rate-limiting toxicity (13). Recently, investigators have become interested in α-emitter radionuclides because of their shorter tissue path-lengths (50–80 μm, several cell diameters) and high linear energy transfer (LET) (14,15). In this regard, several α-emitters, including 213Bi, 212Pb, and 225Ac, have been evaluated for targeting CD38 in MM models (16–18). Each of these α-emitters differs in their radiologic half-lives, with implications for their suitability for therapeutic studies, since the anti-CD38 antibody biologic half-life may be measured in weeks (19). With this consideration in mind, the 10-d radiologic half-life of 225Ac, plus its decay scheme delivering 4 α-particles over its half-life, is especially attractive. Accordingly, in a subcutaneous model of MM treated with 225Ac-labeled daratumumab, Dawicki et al. showed a decreased tumor growth rate in treated versus control groups (18).
In this study, we compared daratumumab labeled with the β-emitter 177Lu to that labeled with the α-emitter 225Ac in a disseminated model of MM, and on the basis of these data, we performed mathematic modeling as a tool for quantifying the radiobiologic effect for future applications of dose optimization.
MATERIALS AND METHODS
Antibodies, Reagents, and Cell Lines
Daratumumab, an anti-CD38 antibody, was obtained from Janssen Biotech Inc. Green fluorescent protein luciferase–positive MM1-S MM cells were provided by Dr. Irene Ghobrial (Dana-Farber Cancer Institute). DOTA-mono-N-hydroxysuccinimide ester was from Macrocyclics, Inc. 225Ac and 177Lu were obtained from the Department of Energy, Oak Ridge National Laboratory.
Animal Studies and Bioluminescence Imaging (BLI)
All animal studies were performed on 6- to 10-wk-old NOD.Cg-Prkdcscid Il2rgtm1Wjl/SzJ mice (NSG; Jackson Laboratory) in accordance with National Institutes of Health Office of Laboratory Animal Welfare guidelines and protocol 14043 of the City of Hope Institutional Animal Care and Use Committee, and with the approval of that committee. The animals were housed in pie cages, in a specific-pathogen-free room, with a maximum of 5 mice per cage. The MM1-S cell line was injected intravenously, at 5 × 106 cells/200 μL of phosphate-buffered saline per mouse. Tumor distribution and growth were followed by serial whole-body imaging on the Lago X (Spectral Instruments Imaging). Before undergoing in vivo imaging, the animals were anesthetized with 4% isoflurane and injected intraperitoneally with 200 μL of d-luciferin (15 mg/mL) in sterile phosphate-buffered saline. All BLI data are depicted in radiance units (photons/s/cm2/steradian) measured over the whole body as the region of interest. Mice were grouped so that the average BLI was similar across all groups. Whole-body toxicity was measured by monitoring weight loss over time, with weight loss of more than 20% considered an experimental endpoint. Paralysis of the mouse hind legs, a common symptom of the MM tumor models, was used as an alternative endpoint.
Radiolabeling
Daratumumab or control trastuzumab antibodies were reacted with a 30 M excess of the chelator DOTA-mono-N-hydroxysuccinimide ester as previously described (20). DOTA conjugation was confirmed by quadrupole time-of-flight liquid chromatography–mass spectrometry (model 6510; Agilent Technology) as follows: 6 μg of antibody was reduced with 1 μL of 0.2 M Tris(2-carboxyethyl)phosphine for 2 h at 37°C and then analyzed on a high-performance liquid chromatography protein chip (Agilent Technologies). DOTA-conjugated antibody (200 μg) was incubated with 177Lu at a labeling ratio of 0.37 MBq/μg for 45 min at 43°C, chased with 1 mM diethylenetriamine pentaacetic acid, and purified on a size-exclusion, preparative column (Superdex-200; GE Healthcare Life Sciences). DOTA-conjugated antibody (50 μg) was incubated with 225Ac at a labeling ratio of 1.85 kBq/μg for 45 min at 43°C and chased with 1 mM diethylenetriamine pentaacetic acid. Radiolabeling efficiencies determined by instant thin-layer chromatography were between 89% and 100% for all reactions.
Therapy
Mice injected intravenously with MM1-S were randomized by BLI after 9–19 d, before the start of radioimmunotherapy. The mice were given intravenous immunoglobulin by intraperitoneal injection 2 h before the start of radioimmunotherapy. For the high-dose 177Lu study, the mice were treated with saline, unlabeled daratumumab, or 11.1 MBq of 177Lu-DOTA-daratumumab. In a follow-up study, the mice were treated with saline or with 1.85, 3.7, or 7.4 MBq of 177Lu-DOTA-daratumumab. For 225Ac radioimmunotherapy, the mice were treated with saline, 22.2 kBq of untargeted 225Ac-DOTA-trastuzumab, or 11.1 kBq or 22.2 kBq of targeted 225Ac-DOTA-daratumumab. For the lower-dose radioimmunotherapy study, the mice were treated with saline; with 0.925, 1.85, or 3.7 kBq of untargeted 225Ac-DOTA-trastuzumab; or with 0.925, 1.85, or 3.7 kBq of targeted 225Ac-DOTA-daratumumab. All therapy doses were made up to 30 μg of antibody, for a total volume of 200 μL.
Statistical Analysis
ANOVA (Tukey multiple-comparison test) was applied to analyze the tumor growth curves—and the log-rank Mantel–Cox test, to analyze survival curves—using Prism, version 7.02 (GraphPad Software). P values for each group are reported as a measure of statistical significance compared with the vehicle control group. Differences were considered significant if the P value was less than 0.05.
Dosimetry and Mathematic Modeling Calculations
The dosimetry and mathematic modeling calculations are provided in the supplemental materials (supplemental materials are available at http://jnm.snmjournals.org) (21–28).
RESULTS
177Lu-DOTA-Daratumumab Radioimmunotherapy
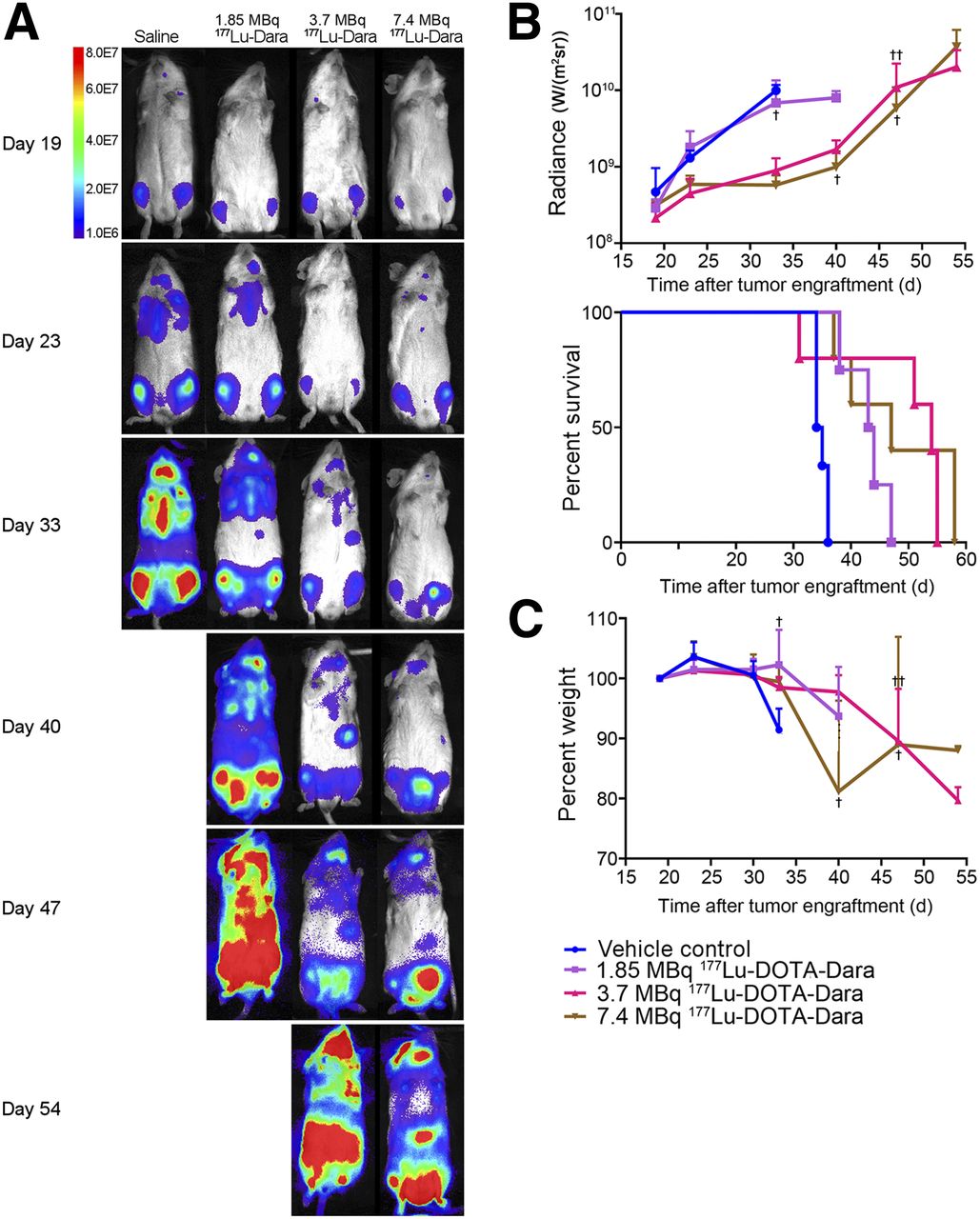
The antitumor activity of 177Lu-DOTA-daratumumab was evaluated in a disseminated MM model using luciferase-transfected MM1-S cells injected intravenously in NSG mice, after cancer progression as determined by BLI. The mice were treated 19 d after MM1-S injection, at which point all mice showed disseminated MM by BLI. Weight loss was used as an appropriate measure of whole-body toxicity. Although BLI measurements demonstrated that a dose of 11.1 MBq of 177Lu-DOTA-daratumumab caused significant regression of MM (Figs. 1A and 1B), there was little increase in median survival (36 d) compared with the control groups (33 d), likely indicating the mice died because of whole-body toxicity (Fig. 1C; Table 1; Supplemental Fig. 1). Because the 11.1-MBq dose had a minimal effect on survival, lower doses of 177Lu-DOTA-daratumumab were investigated (Fig. 2; Supplemental Fig. 2). The 1.85-MBq group had an extended median survival of 44 d, in contrast to 33 d in the untreated control group (Fig. 2B). The median survival of the 3.7- and 7.4-MBq groups was extended to 54 and 47 d, respectively (Fig. 2B; Table 1). Because the median survival of the 7.4-MBq group was less than that of the 3.7-MBq group, 7.4 MBq was the maximum tolerated dose. Notably, the control group exhibited substantial weight loss by day 30, because of MM burden (Figs. 1C and 2C). We thus found that β-emitter–based radioimmunotherapy led to high toxicity, with a maximum increase of 60% in median survival in this model of disseminated MM.

High-dose 177Lu-DOTA-daratumumab (11.1 MBq) for treatment of disseminated MM. (A) Representative bioluminescence images for each group, imaged weekly, with intensity as indicated by color bar. Single mouse survived until day 36 (not shown in A). (B) Myeloma burden as quantified on BLI images, in radiance (daratumumab, P > 0.999; 11.1 MBq of 177Lu-DOTA-daratumumab, P = 0.038) and as quantified on Kaplan–Meier survival plot (daratumumab, P > 0.999; 11.1 MBq of 177Lu-DOTA-daratumumab, P = 0.045). (C) Whole-body toxicity as measured by weight (daratumumab, P = 0.883; 11.1 MBq of 177Lu-DOTA-daratumumab, P = 0.914). n = 4 for all groups. Dara = daratumumab.

Dose response of 177Lu-DOTA-daratumumab (1.85, 3.7, and 7.4 MBq) for treatment of disseminated MM model. (A) Representative BLI images for each group, with intensity as indicated by color bar. (B) MM burden as quantified on BLI images, in radiance (1.85 MBq of 177Lu-DOTA-daratumumab, P = 0.91; 3.7 MBq of 177Lu-DOTA-daratumumab, P = 0.015; 7.4 MBq of 177Lu-DOTA-daratumumab, P = 0.014) and as quantified on Kaplan–Meier survival plot (1.85-MBq dose, P < 0.01; 3.7-MBq dose, P = 0.0310; 7.4-MBq dose, P < 0.01). Crosses indicate days on which mice were euthanized. (C) Whole-body toxicity as measured by weight (1.85-MBq dose, P = 0.997; 3.7-MBq dose, P = 0.821; 7.4-MBq dose, P = 0.750). n = 6 for saline group, 4 for 1.85-MBq group, and 5 for 3.7- and 7.4-MBq groups. Dara = daratumumab.
Efficacy, Toxicity, and Whole-Body Absorbed Dose for 177Lu Radioimmunotherapy in MM1-S Disseminated MM
Efficacy, Toxicity, and Whole-Body Absorbed Dose for 225Ac-Targeted α-Therapy in MM1-S Disseminated MM
225Ac-DOTA-Daratumumab Radioimmunotherapy
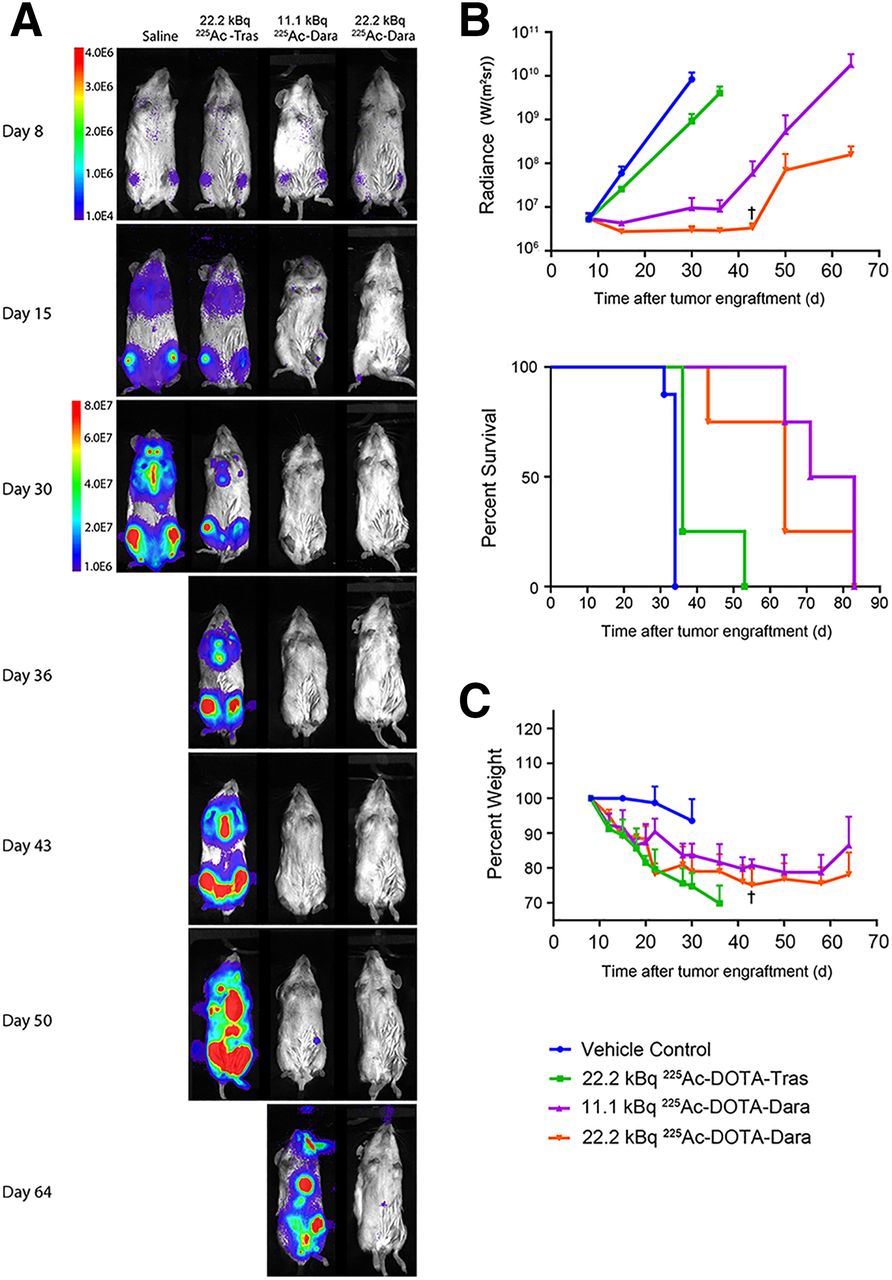
The α-emitter 225Ac was investigated with the hypothesis that there would be less off-target toxicity because of its lower penetrative power, while still maintaining a therapeutic effect due to its higher LET. A preliminary study was performed with 2 predicted high doses of 225Ac-DOTA-daratumumab, 11.1 and 22.2 kBq, in the interest of defining whole-body toxicity. 225Ac-DOTA-trastuzumab was used as an untargeted control, since the MM1-S cell line does not express human epidermal growth factor receptor 2 (29). There was a dose-dependent reduction in the tumor growth curves, with the targeted 22.2 kBq having the highest impact on the delay of tumor regrowth, as measured by whole-body BLI (Figs. 3A and 3B). The targeted 22.2-kBq group had almost double the median survival (64 d) of the untreated controls (33 d), with an even greater improvement (77 d) observed in the targeted 11.1-kBq group (Fig. 3B; Supplemental Fig. 3; Table 2). The lower median survival of the targeted 22.2-kBq group means that this group likely reached the maximum tolerated dose, reflected by greater whole-body toxicity as measured by weight loss (Fig. 3C). The 22.2-kBq untargeted control group had an insignificant median survival of 36 d, compared with untreated controls, and exhibited the highest level of whole-body toxicity (Table 2; Fig. 3C).
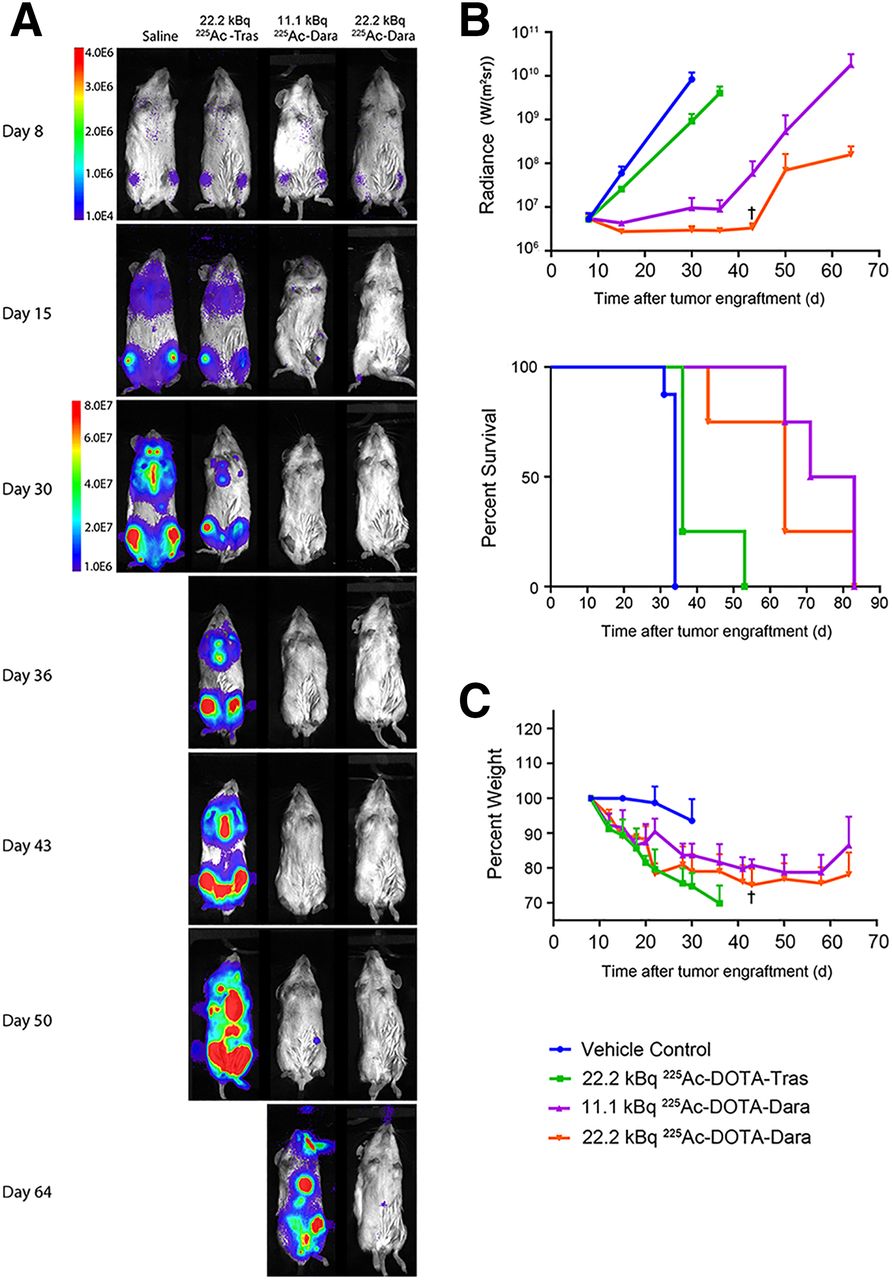
High dose of 225Ac-DOTA-daratumumab (11.1 and 22.2 kBq) for treatment of disseminated MM. (A) Representative BLI for each group, with intensity as indicated by color bar. To visually compare groups, >30-d separate scale was used. (B) MM burden as quantified on BLI, in radiance (22.2 kBq of 225Ac-DOTA-trastuzumab, P = 0.035; 11.1 kBq of 225Ac-DOTA-daratumumab, P = 0.015; 22.2 kBq of 225Ac-DOTA-daratumumab, P = 0.015) and as quantified on Kaplan–Meier survival plot (22.2 kBq of 225Ac-DOTA-trastuzumab, P < 0.01; 11.1 kBq of 225Ac-DOTA-daratumumab, P < 0.01; 22.2 kBq of 225Ac-DOTA-daratumumab, P < 0.01). Crosses indicate days on which mice were euthanized. (C) Whole-body toxicity as measured by weight (22.2 kBq of 225Ac-DOTA-trastuzumab, P = 0.0096; 11.1 kBq of 225Ac-DOTA-daratumumab, P = 0.0306; 22.2 kBq of 225Ac-DOTA-daratumumab, P = 0.0048). n = 8 for saline group and 4 for treated groups. Dara = daratumumab; Tras = trastuzumab.
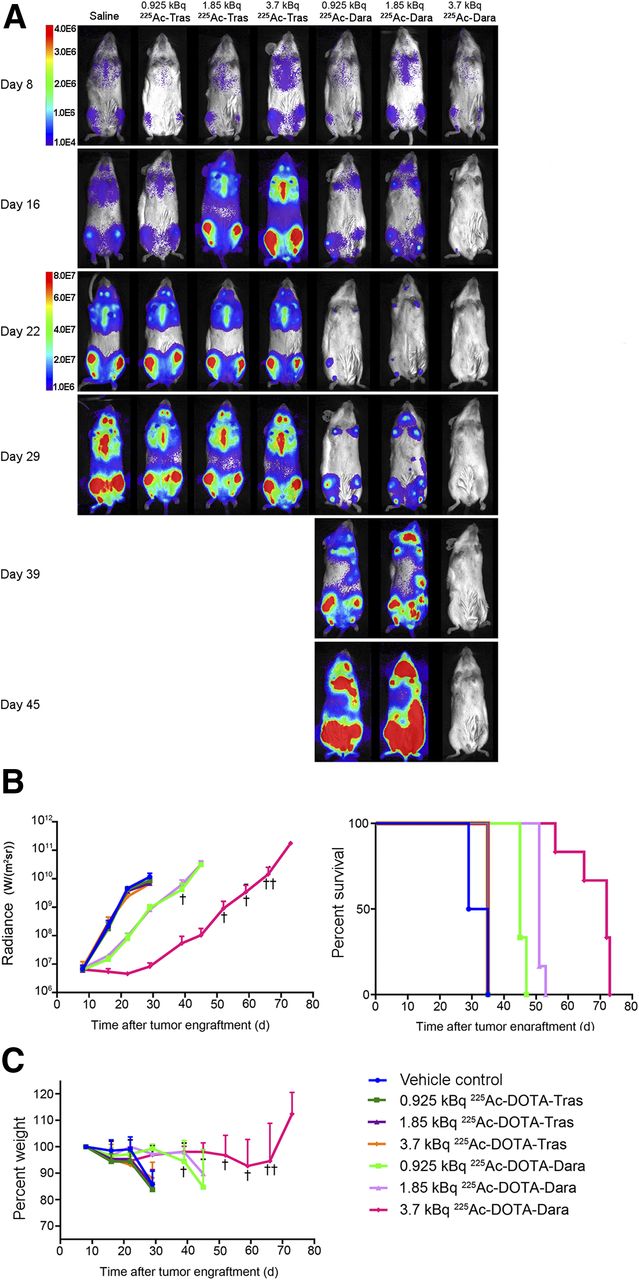
Targeted α-therapy with lower doses of targeted 225Ac-DOTA-daratumumab was performed to determine an optimal therapeutic effect while maintaining low whole-body toxicity. The untargeted control groups with doses of 0.925, 1.85, and 3.7 kBq showed an insignificant difference in median survival (35 d), compared with the untreated control (33 d) survival curves (Fig. 4; Supplemental Fig. 4; Table 2). Both the targeted 0.925-kBq and the targeted 1.85-kBq dose groups had a similar reduction in tumor growth, with a median survival of 45 and 52 d, respectively (Fig. 4B; Table 2). The targeted 3.7-kBq dose group showed the second highest therapeutic effect (72 d), after the targeted 11.1-kBq dose group (77 d), more than doubling the median survival (Fig. 4B) while showing no significant difference in weight loss compared with the untreated controls (Fig. 4C).
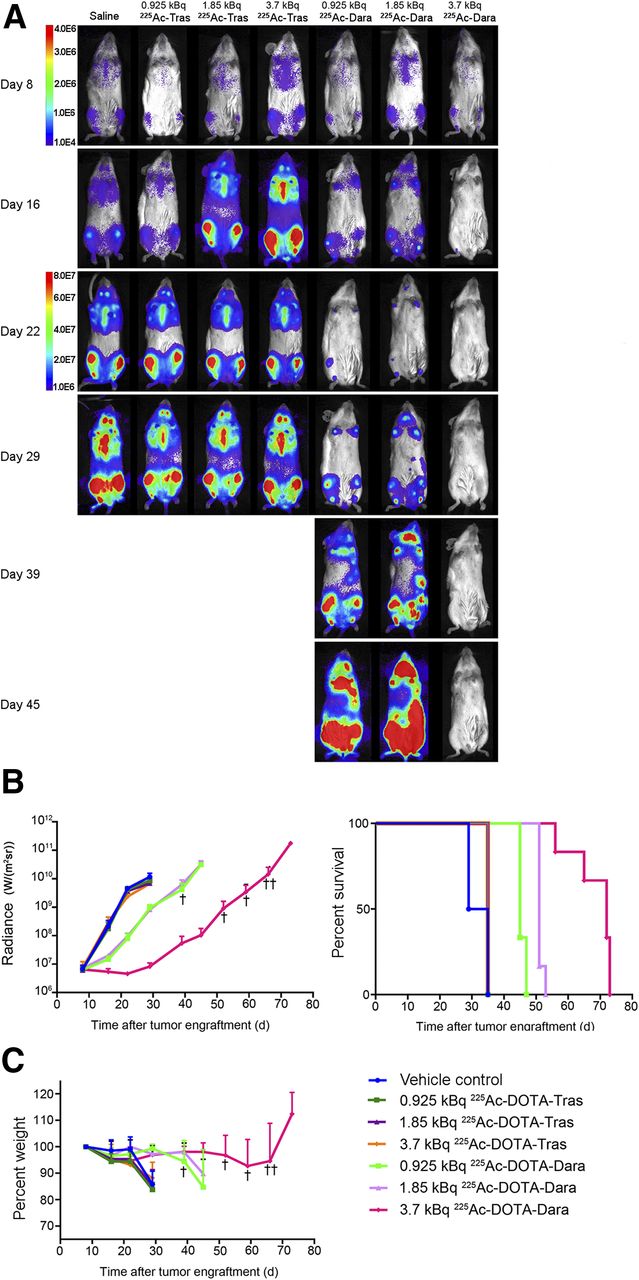
Dose response of 225Ac-DOTA-daratumumab (0.925, 1.85, and 3.7 kBq) for treatment of disseminated MM. (A) Representative BLI for each group, with intensity as indicated by color bar. After day 52, single mouse survived until day 66 (not shown in A). To visually compare groups, >30-d separate scale was used. (B) MM burden as quantified on BLI, in radiance (225Ac-DOTA-trastuzumab groups: 0.925 kBq, P = 0.96; 1.85 kBq, P = 0.67; 3.7 kBq, P = 0.42) (225Ac-DOTA-daratumumab groups: 0.925 kBq, P < 0.01; 1.85 kBq, P < 0.01; 3.7 kBq, P < 0.01) and as quantified on Kaplan–Meier survival plot (225Ac-DOTA-trastuzumab groups: 0.925 kBq, P = 0.048; 1.85 kBq, P = 0.048; 3.7 kBq, P = 0.048) (225Ac-DOTA-daratumumab groups: 0.925 kBq, P < 0.01; 1.85 kBq P < 0.01; 3.7 kBq, P < 0.01). Crosses indicate days on which mice were euthanized. (C) Whole-body toxicity as measured by weight (225Ac-DOTA-trastuzumab groups: 0.925 kBq, P = 0.992; 1.85 kBq, P = 0.999; 3.7 kBq, P = 0.999) (225Ac-DOTA-daratumumab groups: 0.925 kBq, P ≥ 0.999; 1.85 kBq, P ≥ 0.999; 3.7 kBq, P = 0.995). n = 8 for saline group and 6 for therapy groups. Dara = daratumumab; Tras = trastuzumab.
Radiobiologic Modeling
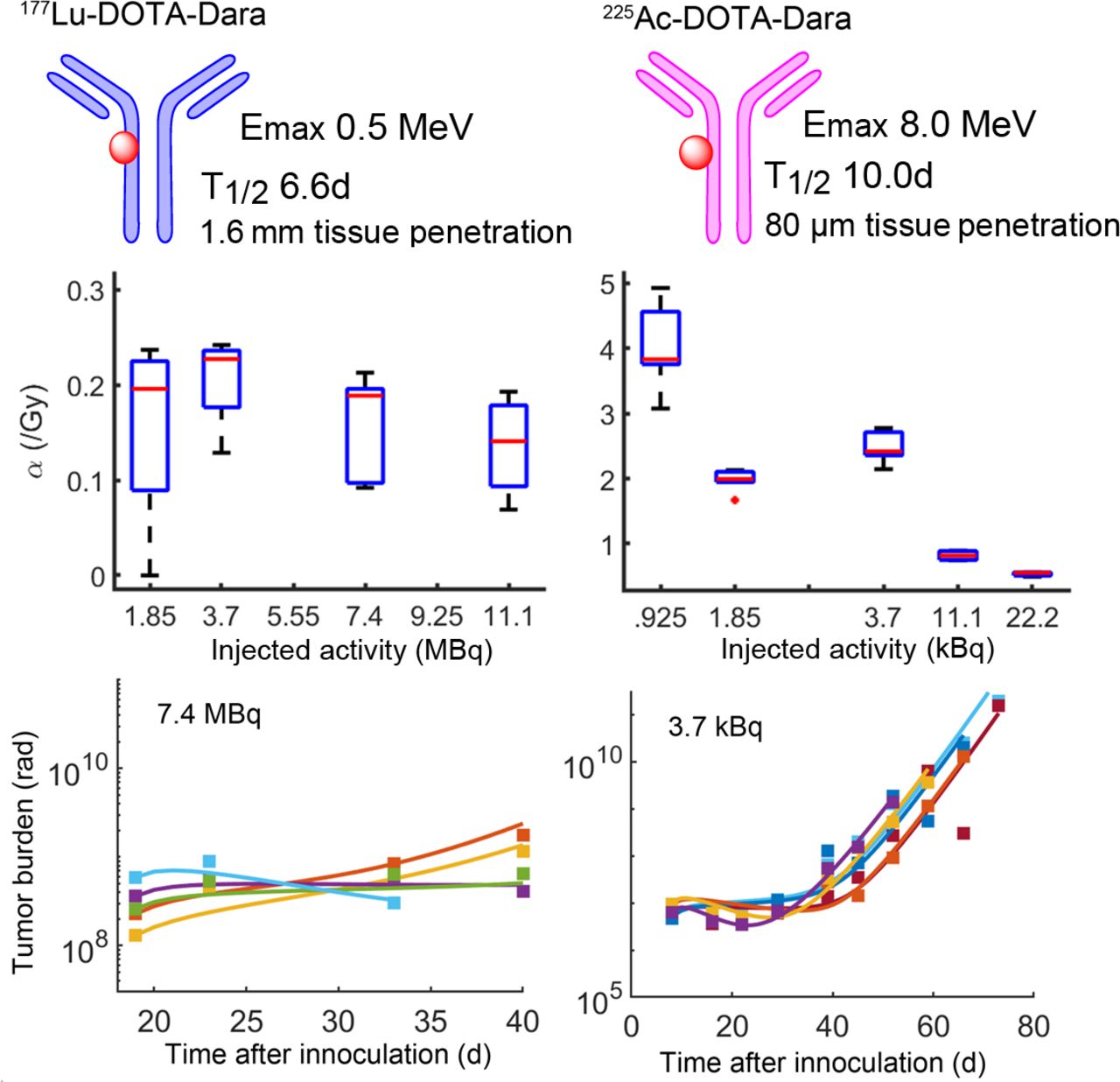
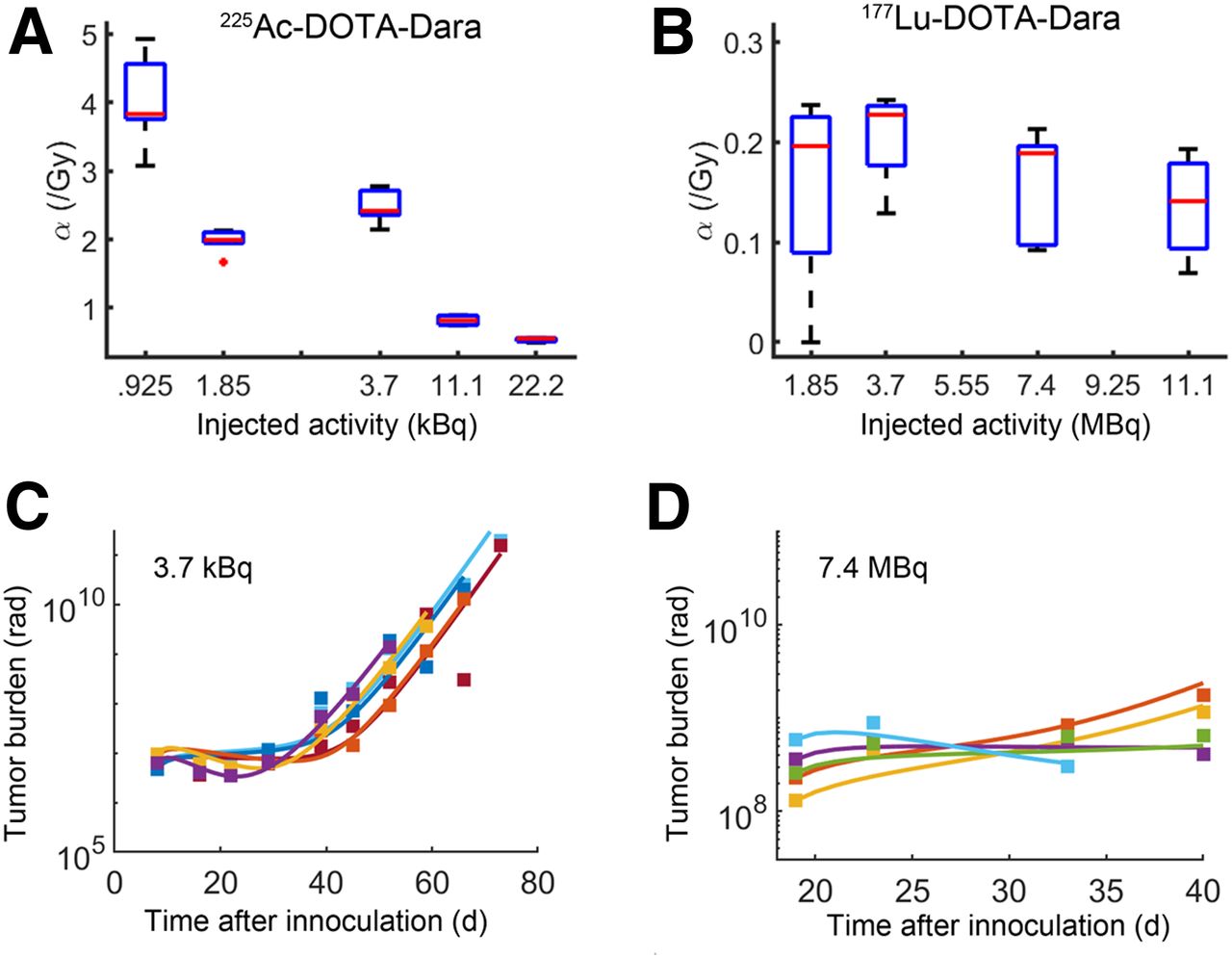
The major differences in the results with α- versus β-emitter radioimmunotherapy in disseminated MM was modeled in terms of differences between α- and β-particle interactions with tissues that result in different cell survival characteristics. One would predict that, since the high-LET radiation of α-emitters deposits more energy per unit distance than do β-emitters, they would effect more damage to the targeted cells. We quantified the radiobiologic effects of the 177Lu and 225Ac with the linear quadratic model parameter α(Gy−1), which is associated with radiosensitivity. By fitting a mathematic model that accounts for MM proliferation and the action of the radioimmunotherapy to the tumor burden data, we observed the MM tumors to have a 10-fold increase in radiation sensitivity to 225Ac-radioimmunotherapy, compared with 177Lu-radioimmunotherapy, for all tested doses, consistent with the relative biological effectiveness of high-LET α-radiation compared with low-LET β-radiation (Fig. 5). Importantly, we observed a nonlinear relationship between radiosensitivity and injected dose activity for 225Ac, with a predicted peak of therapeutic radiosensitivity at a dose of 3.7 kBq (Fig. 5A). In contrast, much less variation in radiosensitivity was observed across dose levels for 177Lu (Fig. 5B). A table of model parameters and model parameter sensitivity analysis is provided in the supplemental materials (Supplemental Figs. 5 and 6; Supplemental Table 1).

Radiobiologic analysis of 225Ac-DOTA-daratumumab and 177Lu-DOTA-daratumumab therapy. Radiosensitivity parameter α (Gy−1) is calculated for all dose levels of 225Ac and 177Lu DOTA-daratumumab treatments. (A) We observed nonlinear relationship between radiosensitivity and dose for 225Ac. Although 0.925 kBq results in largest value of α, this dose level did not confer survival advantage. Model predicts 3.7 kBq of 225Ac-DOTA-daratumumab to provide largest radiosensitivity and therapeutic benefit relative to 1.85-, 11.1-, and 22.2-kBq doses. (B) Low-LET 177Lu results in 10-fold lower α than does high-LET 225Ac and less pronounced correlation with injected activity. (C and D) Tumor burden measured by bioluminescence over time and mathematic model fits for 3.7 kBq of 225Ac and 7.4 MBq of 177Lu, respectively. Difference in duration of response can be seen between 225Ac and 177Lu, 60–80 d vs. 30–40 d. Dara = daratumumab.
DISCUSSION
Theranostics is a treatment strategy that combines diagnostics with therapy. Daratumumab is a promising theranostic agent, since the antibody alone is Food and Drug Administration–approved for MM therapy (30) and is being investigated as a carrier for the targeted delivery of cytotoxic agents (31). Caserta et al. showed that 64Cu-DOTA-daratumumab retained full immunoreactivity to CD38 and gave more specific and sensitive PET/CT tumor images than did 18F-FDG in a disseminated MM model (29). On the basis of the preclinical results, 64Cu-DOTA-daratumumab was approved for a clinical trial at the City of Hope—a trial in which 64Cu-DOTA-daratumumab also preliminarily showed higher sensitivity than the Food and Drug Administration–approved 18F-FDG imaging agent in the imaging of MM patients (32).
A recent study by Dawicki et al. used a similar 225Ac-DOTA-daratumumab construct for targeted α-therapy in both lymphoma and MM mouse models (18). However, that study used a subcutaneous xenograft model with therapy given via an intraperitoneal injection, versus our study’s disseminated MM model with the targeted α-therapy given intravenously. Whereas Dawicki et al. showed an antitumor effect with high doses of unlabeled daratumumab antibody alone, this result was not seen in our experiments, perhaps because of differences in immune status between the 2 mouse models. In the subcutaneous MM model, the researchers saw a decrease in tumor growth rate at a targeted α-therapy dose of 14.8 kBq, and in our disseminated model, targeted α-therapy doses of 22.2 and 11.1 kBq prevented tumor progression for up to 35 and 25 d after treatment, respectively. We believe that the disseminated MM model is more similar to the spread of MM in humans and that intravenous versus intraperitoneal injections allow for more rapid systemic diffusion of the agent. Similarly to our study, Dawicki et al. observed no unacceptable toxicity in terms of weight loss. They also reported no significant difference in hematologic, liver, or kidney toxicity between the targeted α-therapy and control groups. Both studies indicate that the use of α-therapy targeted to CD38 shows great promise in the treatment of MM, with little off-target toxicity.
Compared with targeted β-therapy, targeted α-therapy caused a more pronounced regression of MM growth while displaying lower whole-body toxicity. As the total-body absorbed dose increased, the median survival of 177Lu-radioimmunotherapy–treated mice did not increase in a parallel fashion (Table 1), likely because of bone marrow toxicity, a consequence of the long path-length of the 177Lu β-emitter. In contrast, 225Ac-based targeted α-therapy had less whole-body toxicity and displayed a dose-dependent therapeutic effect. As the total absorbed dose increased, the median survival also increased, a consequence of its lower path length and higher LET (Table 2). This effect is specific for targeted α-therapy, since the untargeted α-therapy led to no improvement in median survival with increasing doses. This effect was consistent with mathematic modeling, an approach that quantified the radiobiologic effects of the radionuclides and predicted a maximal therapeutic radiosensitivity at 3.7 kBq of administered 225Ac-DOTA-daratumumab. Going forward, the 3.7-kBq dose of 225Ac-DOTA-daratumumab–targeted α-therapy shows the most promise, especially for combinatorial therapy, as its therapeutic efficacy is similar to the higher 11.1- and 22.2-kBq dose groups in causing initial regression of the MM and more than double the median survival time while not showing the significant toxicity seen with the higher-dose 225Ac groups. On the basis of our experience with targeted α-therapy, it is likely that proper scaling of these doses to humans warrants evaluation in a clinical trial. Furthermore, in MM patients undergoing daratumumab therapy who experience tumor progression, daratumumab therapy is often discontinued, yet analysis of their cancer cells reveals continued CD38 expression (9,33). Thus, even previously treated daratumumab patients may be candidates for CD38 targeted α-therapy.
CONCLUSION
We conclude, and mathematic modeling confirms, that maximal biologic doses were achieved by targeted α-therapy and demonstrated 225Ac to be superior to 177Lu in delaying tumor growth and decreasing whole-body toxicity.
DISCLOSURE
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under grants R01CA238429 (Russell Rockne, John Shively, and Flavia Pichiorri) and P30CA03357 (City of Hope Comprehensive Cancer Center support). No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can 225Ac-DOTA-daratumumab lead to a better tumor response and less whole-body toxicity than 177Lu-DOTA-daratumumab in a disseminated model of MM?
PERTINENT FINDINGS: Targeted α-therapy with 225Ac-DOTA-daratumumab at 3.7 kBq demonstrated optimal tumor response with no whole-body toxicity, whereas 177Lu-DOTA-daratumumab showed no dose-dependent tumor response and was toxic at all doses. Mathematic modeling of radiobiologic effects demonstrated the superiority of targeted α-therapy in a disseminated model of MM.
IMPLICATIONS FOR PATIENT CARE: Targeted α-therapy for disseminated MM with proper scaling of 225Ac-DOTA-daratumumab doses to humans warrants evaluation in a clinical trial.
Footnotes
Published online Oct. 30, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 19, 2020.
- Accepted for publication October 7, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}