


Abstract
ABT-806 is a tumor-specific antibody targeting the epidermal growth factor receptor (EGFR). This study assessed safety, biodistribution, and pharmacokinetics of 111In-radiolabeled ABT-806 (ABT-806i) and effects of repeated doses of ABT-806 on receptor occupancy. Methods: Eligible patients had advanced tumors likely to express EGFR/EGFRvIII; adequate performance status and organ function; and measurable disease by RECIST 1.1. In cohort 1, 6 patients received a bolus administration of ABT-806i and underwent SPECT followed by whole-body planar scans. In cohort 2, 12 patients were imaged similarly as in 1 initially; thereafter, they received 3 doses of unlabeled ABT-806, before another dose of ABT-806i with associated SPECT and whole-body planar scans. At the end of both cohorts, patients who had stable or responding disease were able to enroll into an extension study (M12-326) in which they received unlabeled ABT-806 every 2 wk until disease progression, withdrawal of consent, or intolerable toxicity. Results: No toxicity related to ABT-806i infusion was observed. ABT-806i showed minimal uptake in normal tissues and cleared gradually from blood with a half-life of 6.0 ± 1.5 d. The mean effective dose of ABT-806i was 0.137 mSv/MBq for males and 0.183 mSv/MBq for females. ABT-806i tumor uptake varied and did not correlate with archived tumor EGFR expression. No change in ABT-806i uptake was observed after interval ABT-806 treatment, indicating stable EGFR expression in tumor. The patient with highest tumor uptake of ABT-806i had advanced head and neck cancer and experienced a partial response. Conclusion: ABT-806i allows for real-time imaging of EGFR conformational expression in tumors, has an acceptable radiation dosimetry, and provides important additional information about antigen expression compared with standard approaches using archival tissue. Its role to assist in patient selection for EGFR-based therapeutics and investigate treatment resistance should be further investigated.
The epidermal growth factor receptor (EGFR) gene is a validated target in oncology. Monoclonal antibodies against EGFR are used to treat cancers of the head and neck, colon, and lung (1,2). Tyrosine kinase inhibitors of EGFR are used in the treatment of lung cancer with activating kinase mutations (1,2). The most common toxicity of these agents is a well-characterized skin rash (3). Other toxicities include diarrhea, stomatitis, fatigue, and electrolyte disturbances.
ABT-806 is a humanized recombinant IgG1κ antibody that is specific for a unique, conformationally exposed epitope of EGFR. This epitope is available for binding only under conditions where there is dysregulated EGFR activation due to conditions such as EGFR amplification, presence of specific mutations such as EGFRde2–7 (EGFRvIII), or presence of autocrine loops (1,4–6). The epitope is inaccessible when EGFR is expressed at normal physiologic levels; thus, ABT-806 has limited binding to normal tissues (1,4–6). ABT-806 reproducibly inhibits the growth of multiple EGFR amplified/EGFRvIII mutated tumors preclinically through downregulation of EGFR signaling with resulting antitumor changes in proliferation, angiogenesis, and apoptosis (1,7–9). When compared with other EGFR-directed therapies, preclinical studies show ABT-806 has a favorable toxicity profile and equivalent/improved efficacy to other anti-EGFR antibodies (1,8,10,11). In a phase 1 human study of ABT-806 (study M11-847, NCT01255657), the recommended phase 2 dose was 24 mg/kg (12). Importantly, ABT-806 was shown to have negligible skin or other organ toxicity (12,13).
ABT-806i, an 111In-radiolabeled conjugate of ABT-806, is a novel radiopharmaceutical that was developed for real-time scintigraphic imaging of EGFR. It uses the tumor-specific binding affinity of ABT-806 for the imaging of EGFR-positive tumors to determine whether EGFR amplification, overexpression, or mutation is present. We report herein the results of a first-in-humans trial of ABT-806i, exploring the ability to image the conformational epitope of EGFR bound by ABT-806, the impact of ABT-806 therapy on ABT-806i uptake, and the relationship of ABT-806i uptake to tumor EGFR by immunohistochemistry.
MATERIALS AND METHODS
Trial Objectives
This first-in-humans trial (M11-849, NCT01472003) was a 2-cohort, open label, multicenter study to determine the biodistribution and dosimetry of ABT-806i. Secondary objectives included characterization of ABT-806i pharmacokinetics; examination of ABT-806i SPECT imaging in tumors of different histologies, EGFR expression, and size; and determination of the effect of unlabeled ABT-806 on ABT-806i receptor occupancy. The study was approved by the Austin Health Human Research Ethics Committee, and all subjects signed an informed consent form.
Patient Eligibility for M11-849 Bioimaging Study
Eligible patients were aged 18 y or older; had tumors of a type likely to overexpress wild-type EGFR/EGFRvIII; were Eastern Cooperative Oncology Group Performance Status of 0–2; had measurable disease by RECIST version 1.1, with at least 1 extrahepatic 2-cm lesion; had adequate organ function, defined as absolute neutrophil count ≥ 1,500/mm3; platelets ≥ 100,000/mm3; hemoglobin ≥ 9.0 g/dL; creatinine ≤ 1.5 times the upper limit of the institution’s reference range (×ULN); and bilirubin, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) ≤ 1.5 × ULN (those with liver metastases were eligible if their AST and ALT was ≤ 5.0 × ULN). Exclusion criteria included anticancer therapy within 14 d of the first ABT-806i dose; prior use of EGFR-directed monoclonal antibody within 4 wk of the first ABT-806i dose; presence of unresolved Common Terminology Criteria for Adverse Events grade 2 or higher toxicity from prior therapy; major surgery within 21 d before the first ABT-806i dose; significant comorbidities that posed an unacceptable risk of toxicities; history of major immunologic reaction to any IgG containing agent; and pregnancy or lactating patients.
Radiolabeling of ABT-806i
ABT-806i was formed by mixing a formulated precursor, DTPA-ABT-806, with commercially available 111In trichloride. DTPA-ABT-806 was produced from the conjugation of ABT-806 with the isothiocyanate of the phenylisothiocyanate derivative of dientylenetriaminepentacetic acid (CHX-A″-DTPA). An average of 2–3 CHX-A″-DTPA moieties were conjugated per antibody. For radiolabeling, 0.5 M sodium acetate (pH 7.2, 1.0 mL) was added to 111In trichloride (185–277 MBq [5–7.5 mCi]), and then placed in a sterile reaction vial. DTPA-ABT-806 (5 mg/2 mL) was added to the reaction vial at room temperature and after mixing was withdrawn into a 5-mL syringe. The total reaction time was 30 min. Preclinical studies confirmed retention of binding affinity after radiolabeling (immunoreactive fraction > 65%), radiochemical purity > 90%, and serum stability studies showed retention of immunoreactivity (data not shown).
Trial Design of M11-849 Study
Patients were treated as in Figure 1. Patients in cohort 1 received a single intravenous administration of ABT-806i to determine baseline drug distribution. Predose scintigraphic scanning with 57Co transmission (including whole-body planar and SPECT) were performed on day 1 before bolus administration of ABT-806i (a protein tracer dose of 3–5 mg labeled with 148–259 MBq [4–7 mCi] of indium) preceded approximately 30 min prior by 500–1,000 mg of acetaminophen and 25–50 mg of intravenous promethazine. We and others have previously demonstrated that this dose of 111In (148–259 MBq [4–7 mCi]) is optimal for diagnostic and dosimetric analysis of intact antibodies (13–15). After ABT-806i administration, patients underwent whole-body planar and SPECT scans on days 1, 2; days 3 or 4; days 5 or 6; then on day 7. Thereafter, all patients were eligible to enroll on the extension study (study M12-326, NCT01406119), which is described below.

Patient flow within M11-849 study and subsequently for eligible patient, from the M11-849 study into the M12-356 extension study. *Comprised SPECT scan on day on ABT-806i infusion and then on days 2, 3/4, 5/6, and 7 after infusion based on patient convenience. Note that in Cohort 2, SPECT on day 2 was omitted. **All patients in cohort 1 in M11-849 were clinically stable at the end of week 1 and were immediately enrolled in the M12-356 extension study. ♣7 patients had progressive disease at the time of radiologic restaging at the end of cohort 2 in M11-849, and as such were not eligible for enrolment in M12-356 extension study for patients with clinical stability/benefit on ABT-806 therapy. Pts = patients.
In cohort 2, patients underwent an initial week of imaging for the purposes of determining the biodistribution of ABT-806i, in a manner similar to patients treated on cohort 1. In this first week, they received ABT-806i (148–259 MBq [4–7 mCi])/3–5 mg) on day 1 of week 1; this was then followed by whole-body planar and SPECT scans on day 1; days 3 or 4; days 5 or 6; then on day 7. Beginning on day 1 of week 2, they were treated with either 18 mg/kg or 24 mg/kg of unlabeled ABT-806 every fortnight (weeks 2, 4, and 6); in week 6, they also underwent repeated imaging with another dose of ABT-806i after the unlabeled ABT-806 to determine the effects of unlabeled antibody on receptor occupancy. Imaging after this dose of ABT-806i was on days 2 or 3, 4 or 5, and then day 7 of week 6. At the end of the 6 wk, all patients with disease response or control were eligible to enroll on the extension study (study M12-326, NCT01406119).
The extension study (M12-326, NCT01406119) allowed patients on the bioimaging study (M11-849) who had completed the required imaging and had not progressed to continue treatment with unlabeled ABT-806 until withdrawal of consent, disease progression, need for other cancer therapy, or intolerable toxicity.
Pharmacokinetics During M11-849 Study
Pharmacokinetic samples for ABT-806i and ABT-806 were collected before dosing and up to 168 h after dosing on day 1 of week 1 (cohorts 1 and 2) and up to 336 h after dosing on day 1 of week 6 (cohort 2 only). These were measured using the same validated electrochemiluminescence immunoassay and analyzed using noncompartmental methods (16). Serum samples for antibody drug antibody were collected before dosing on week 1, day 1 and at the end of the study.
Biodistribution and Dosimetry During M11-849 Study
From whole-body planar and SPECT images, the distribution of ABT-806i in the body and tumor uptake was assessed. Tumor uptake in defined target lesions was evaluated on a 4-point scale, with comparison of tumor uptake between initial trace infusion of ABT-806i, and after the second infusion of ABT-806i, to evaluate alteration in EGFR expression after ABT-806 treatment, as well as to define possible receptor occupancy with ABT-806 treatment. The quantitative analysis of ABT-806i in normal tissues was determined in the patients in cohort 1 after injection of ABT-806i by a region-of-interest technique. Radioactivity as percentage injected dose per organ was measured in various organs of the patients at 5 time points over 7 d (∼168 h) after injection. For each patient the %ID values of each organ were plotted against time to generate organ biokinetics to obtain organ radiation exposure (17).
Tumor uptake of ABT-806i was measured based on SPECT imaging before and after ABT-806 treatment and plotted against time. Target lesions were selected based on tumor size, with a minimum size of approximately 2 cm in the longest transverse diameter on CT, and sufficient tumor-to-background ratio, ideally greater than approximately 1.5. A major vessel or the heart, selected based on the anatomy in the field of view, was chosen as the blood-pool region of interest to estimate radioactivity in the whole blood at the time of imaging (14).
Adverse Events During M11-849 Study
Analyses of toxicity included only treatment-emergent adverse events in the first 30 d after the first dose of ABT-806i. Treatment-emergent adverse events were summarized by system organ class and preferred term according to the Medical Dictionary for Regulatory Activities. The severity of toxicity was assessed using the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0 toxicity.
Sample Size of M11-849 Study
A pragmatic sample size of 26–30 patients was chosen, with 6 patients in cohort 1 and the rest in cohort 2. The study was terminated after 18 patients as sufficient data had been gathered with tolerability of highest available dose. Summary statistics for demographics are provided in Table 1.
Patient Demographics
RESULTS
Patients
Patient demographics are shown in Table 1. The first 6 patients were imaged in cohort 1 and then proceeded immediately to treatment with the ABT-806 on the M12-326 extension study (Fig. 1; Table 2). In cohort 2, 6 patients were treated at the 18 mg/kg dose level and 6 patients at the 24 mg/kg dose level. At the end of cohort 2, 5 of 12 patients had stable disease with formal MRI restaging at the end of the imaging study and proceeded to the M12-326 extension study (Fig. 1; Table 2). Of these, 1 patient in cohort 2 with squamous cell carcinoma of the head and neck experienced partial response (patient 8, Table 2). In total, 11 of the 18 patients on the M11-849 biodistribution study had stable or better disease at the end of the study and were screened for enrolment in the M12-326 extension study (Table 2).
Individual Patient Data
Biodistribution of ABT-806i in M11-849 Biodistribution Study
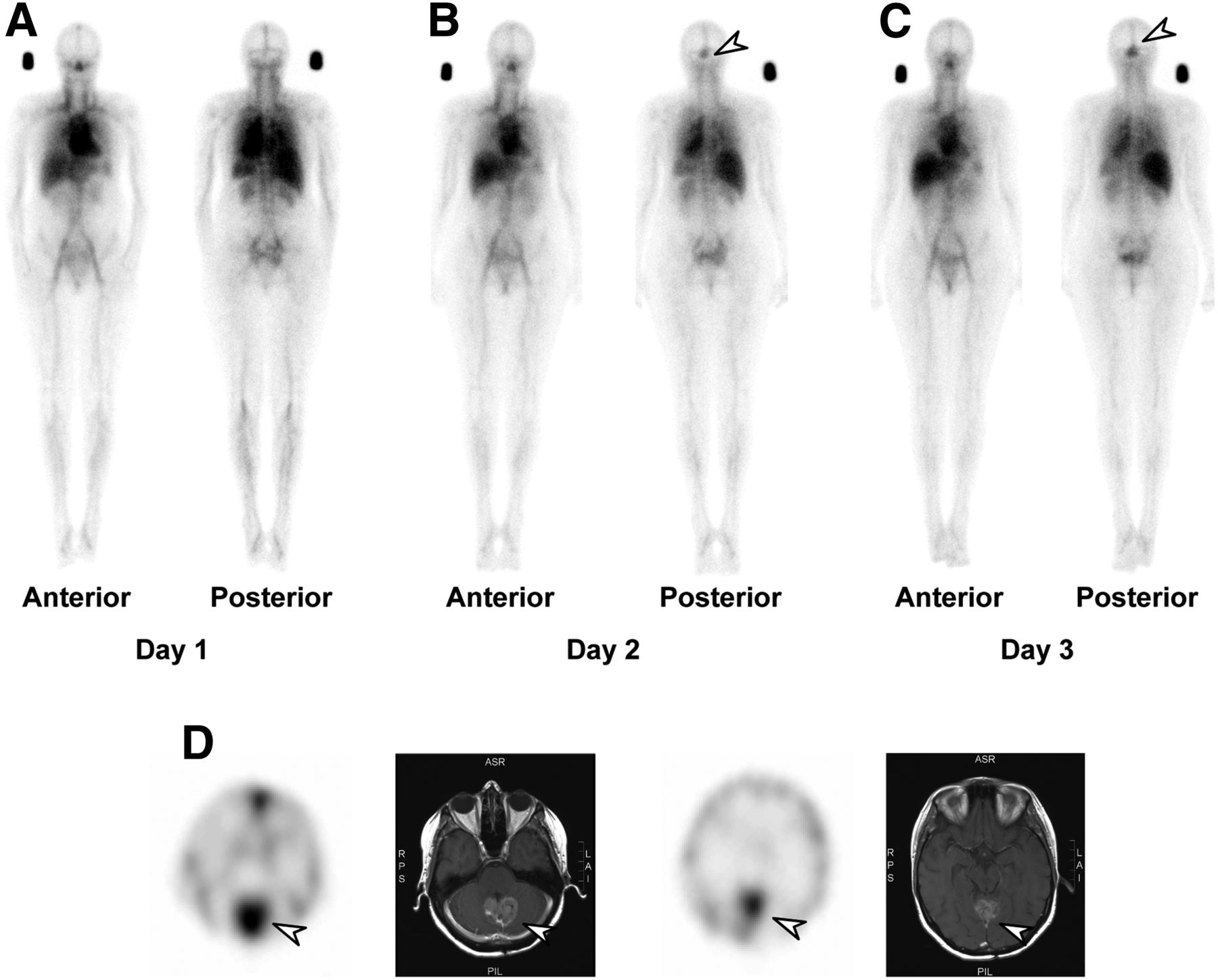
Evaluation of imaging datasets showed initial pooling of ABT-806i in the cardiac blood pool and within large vessels, liver, spleen, and kidneys, followed by gradual blood clearance and washout of ABT-806i from normal tissues over the 8 d of imaging in all patients (Fig. 2). In the patients with uptake of ABT-806i in tumor, this was best seen after day 3, with increasing intensity up to day 8 (Fig. 2). High, specific uptake of ABT-806i in tumor was visualized in the target lesions for 5 of 6 patients in cohort 1, with the other patients having no uptake. High specific uptake was seen in all 12 patients in cohort 2. The uptake of ABT-806i was observed to peak at the seventh or eighth day after injection. Interestingly, both patients with primary brain tumors showed excellent ABT-806i uptake (Fig. 2). Furthermore, the increasing accumulation of ABT-806i over time in tumor (maximal uptake around 4 d), despite decline in serum concentration of ABT-806i during this time frame, would support specific uptake in the glioblastoma tumors imaged in the study. The peak uptake of ABT-806i in target tumor volumes in cohorts 1 and 2 are shown in Tables 3 and 4, respectively.
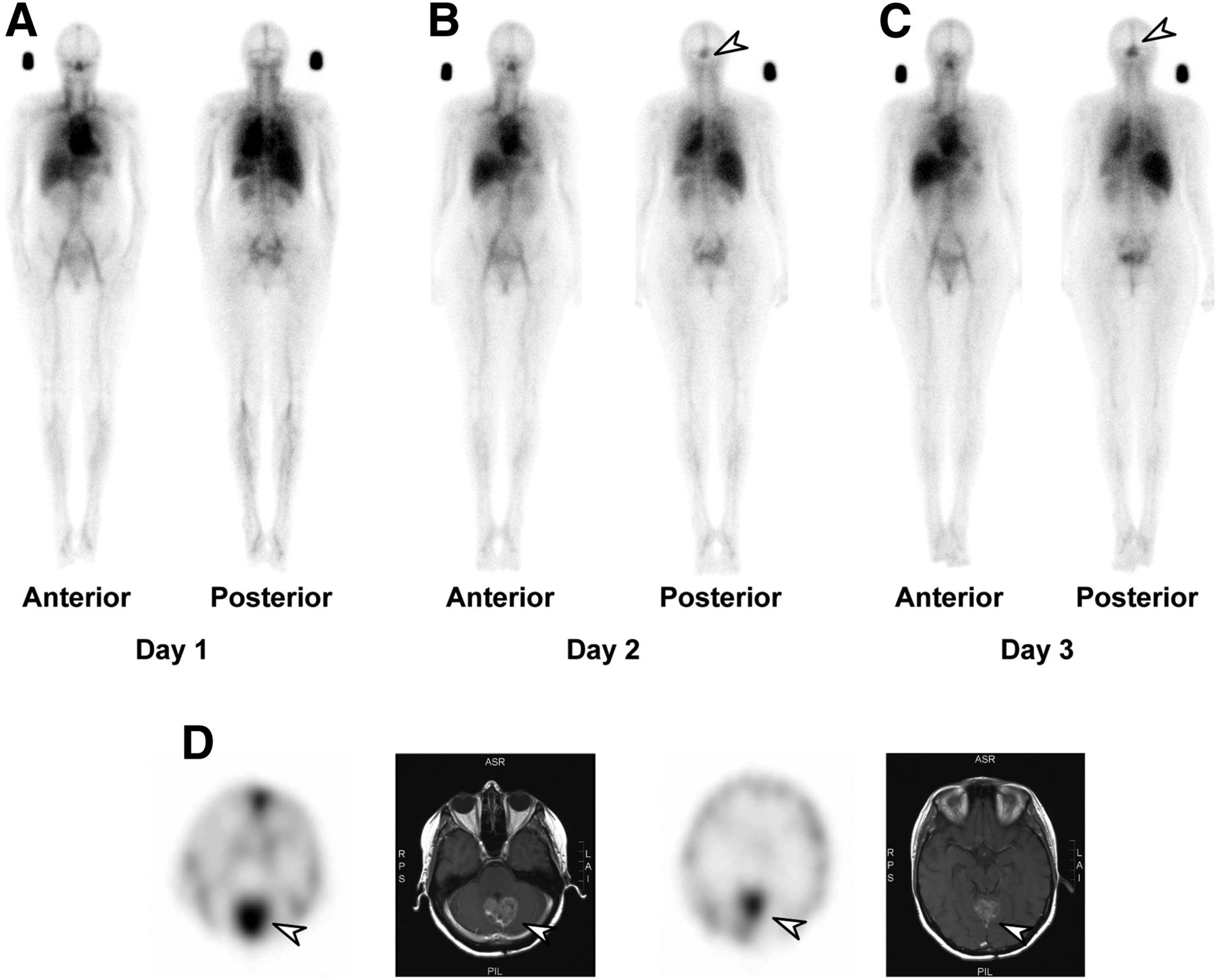
ABT-806i biodistribution and SPECT/CT images of patient with high-grade glioma. (A) Anterior and posterior whole-body planar images at day 1 (standard located above right shoulder for dosimetry). (B) Whole-body planar images at day 2. (C) Whole-body planar images at day 3 in patient 3. Rapid uptake of 111In-ABT-806i in known glioblastoma (arrow) is identified by day 2 and increases by day 3. (D) SPECT/MR images at 2 planes showing high uptake of 111In-ABT-806i in glioblastoma (arrow) in posterior fossa. A focus of 111In-ABT-806i uptake in anterior venous sinus is due to blood-pool activity.
Peak Uptake of 111In-ABT-806i in Target Tumor Lesion in Cohort 1 Patients, Calculated from SPECT Images
Peak Uptake of 111In-ABT-806i in Target Tumor Lesion in Cohort 2 Patients, Calculated from SPECT/CT Images
Pharmacokinetics During M11-849 Biodistribution Study
ABT-806i pharmacokinetics were similar between cohorts 1 and 2 (Table 5; Fig. 3). The apparently shorter observed half-life and higher clearance of ABT-806i compared with ABT-806 (Fig. 3) may be due to a shorter pharmacokinetic sampling period for ABT-806i, although nonlinear pharmacokinetics between the low ABT-806i and high ABT-806 doses cannot be completely excluded. The biodistribution images did not indicate any saturable normal tissue compartment, which would be seen if a nonlinear pharmacokinetics at low protein dose did exist. The ABT-806 pharmacokinetics were consistent with results in the previous phase 1 dose escalation study with ABT-806. No antibody drug antibody was detected after ABT-806 administration in this study.
Pharmacokinetic Parameters of ABT-806i and ABT-806

Serum concentration–time profiles of ABT-806i (week 1, day 1) or ABT-806 (week 6, day 1) after intravenous administration. Mean + SD is shown on a log-linear scale.
Toxicity Within M11-849 Study
No patient in the M11-849 study experienced an adverse event related to ABT-806i. Two patients (33%) in cohort 1 of the M11-849 study each experienced an unrelated adverse event of grade 1 upper respiratory tract infection and grade 2 dyspnoea. Ten patients (83%) in cohort 2 experienced toxicity. One patient in cohort 2 (8%) experienced grade 1 rash that the investigator considered possibly related to ABT-806 but no toxicities related to ABT-806i were reported. Toxicity occurring in ≥ 2 patients in cohort 2 included decreased appetite, fatigue (4 patients each, 33.3%), constipation, nausea, upper respiratory tract infection (3 patients each, 25%), arthralgia, dizziness, and productive cough (2 patients each, 17%) that were unrelated. Two of 10 patients each experienced 2 grade 3 events; the remaining 8 patients experienced grade 1 or 2 events.
Tumor Uptake and Dosimetry of ABT-806i
ABT-806i tumor uptake was quantitatively evaluated for patients in cohorts 1 and 2 (n = 18). Tumor uptake varied greatly between patients and ranged from 0.009 to 5.837 percentage injected dose for a reference lesion. The only nontumor region that showed specific ABT-806i uptake was in patient 1, who had uptake in an area of previous lung radiotherapy, most likely related to enhanced permeability into the area of inflammation. No clear pattern between ABT-806i uptake and EGFR staining in archival tissue was seen (Table 2), although the median interval between tissue acquisition and enrolment on study was 1.5 y (range, 0.3–6.5 y), and archived samples tested were typically from previously removed primary tumors. Repeated treatment with ABT-806 had little effect on ABT-806i tumor accumulation irrespective of ABT-806 dose.
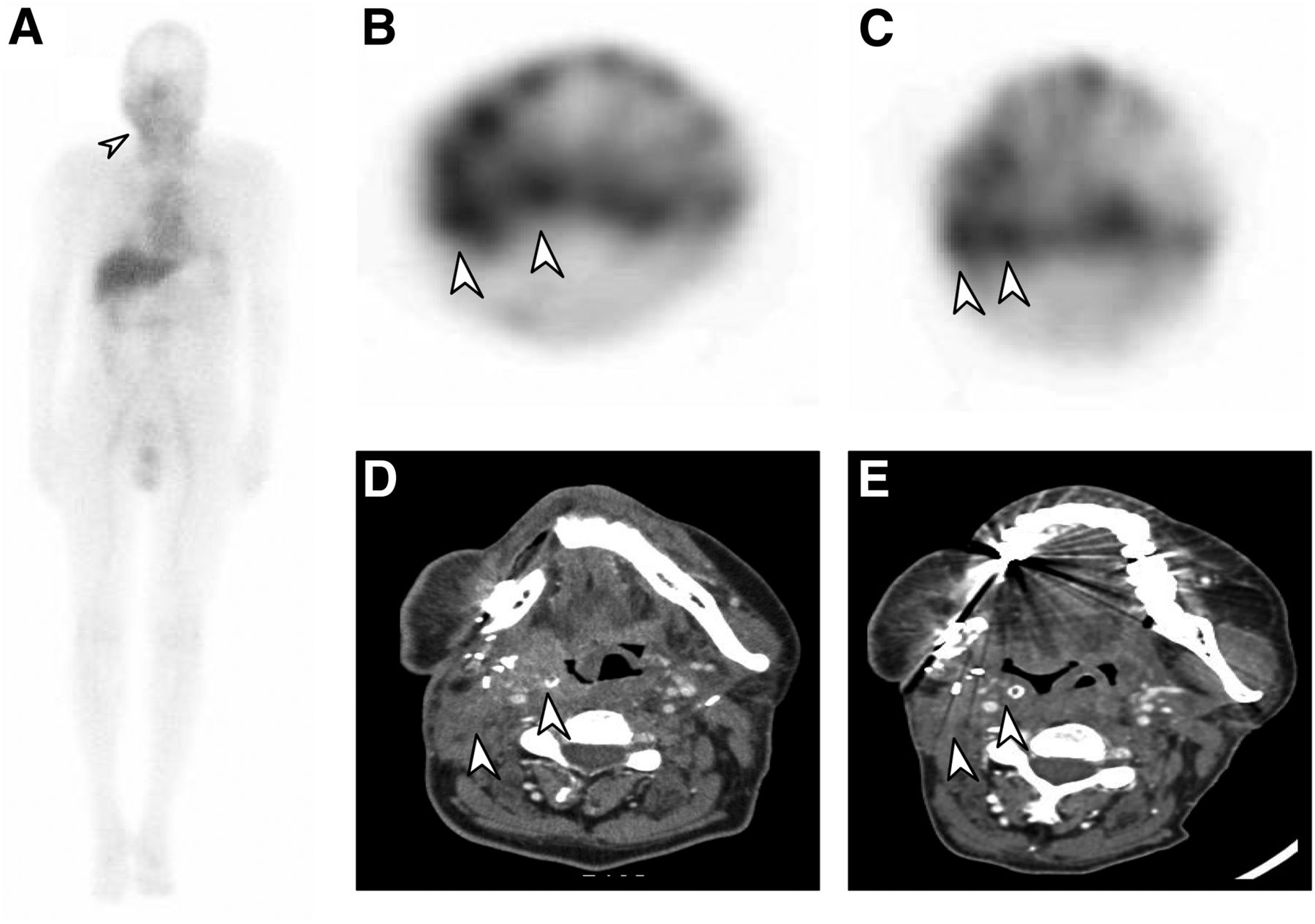
On a per-target lesion basis, there were 12 lesions in cohort 1, of which 7 lesions demonstrated qualitative uptake of ABT-806i, 2 lesions with mild uptake score of 2; 3 lesions with moderate uptake score of 3; and 2 lesions with marked uptake score of 4. There was 1 target lesion with no uptake (score 0), 1 lesion with equivocal uptake, and 1 lesion with nonevaluable uptake. In cohort 2, there were 34 lesions, of which 21 lesions had uptake of ABT-806i, including 14 lesions with moderate uptake score of 3, and 1 lesion with marked uptake score of 4. Importantly, of the 13 patients who had more than one evaluable lesion, 4 patients (31%) showed marked intertumoral variation of uptake of ABT-806i in target lesions. The patient who had a partial response had high (score 3) uptake of ABT-806i (Fig. 4).
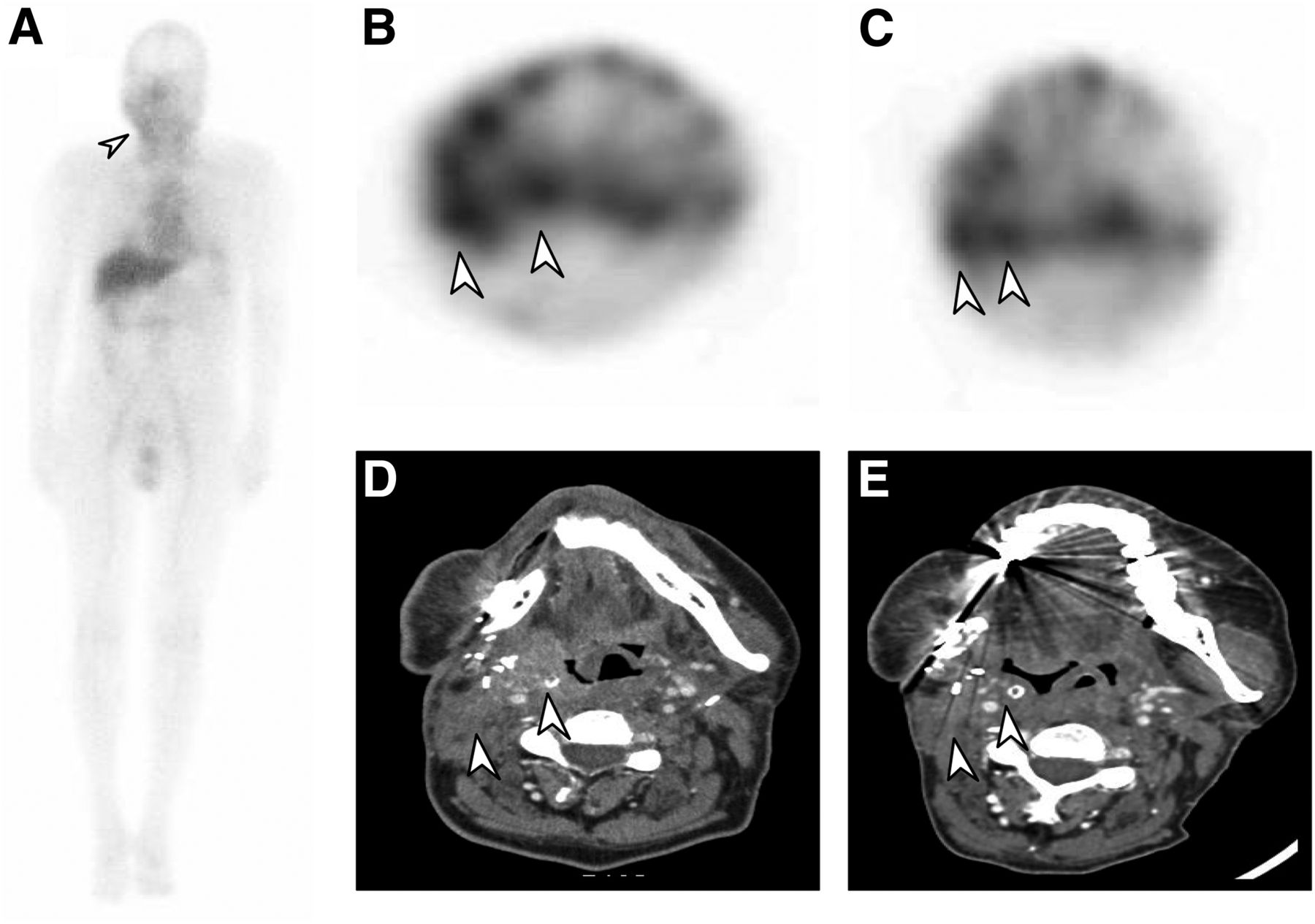
ABT-806i biodistribution and SPECT/CT images of patient with squamous cell carcinoma of head and neck. (A) Whole body planar image of 111In-ABT-806i biodistribution at day 8 in patient 8. Arrow shows localization in tumor area in right neck. (B) Week 1 SPECT image of 111In-ABT-806i uptake in right parapharyngeal lesion and right cervical node (arrows), with uptake increased compared with normal tissue. (C) Week 16 SPECT image of 111In-ABT-806i uptake in right parapharyngeal lesion and right cervical node (arrows), which appear smaller than week 1 images. (D) CT at baseline showing tumor in right parapharyngeal region and right cervical node (arrows), which also showed 111In-ABT-806i uptake. (E) CT at week 16 restaging, showing reduction in size of right parapharyngeal lesion and right cervical node (arrows), assessed as RECIST partial response.
The normal tissue dosimetry of ABT-806i is shown in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). The mean effective dose of ABT-806i was calculated to be 0.137 mSv/MBq for males and 0.183 mSv/MBq for females.
DISCUSSION
The advent of next-generation antibodies such as ABT-806 represents the next wave of EGFR-targeting antibodies with enhanced tumor specificity and minimal cutaneous toxicities (1,7,12,13). ABT-806 has been shown to be well-tolerated and to have little of the cutaneous and other toxicities seen with other anti-EGFR antibodies (12). Our current study confirmed this profile with only 1 patient (6%) experiencing a grade 1 rash that was possibly related to ABT-806. Like other anti-EGFR antibodies that have shown some activity in head and neck cancer (18), there was 1 patient with head and neck cancer who had a prolonged objective response.
Administration of ABT-806i was safe and well tolerated, with no drug-related toxicities. The lung had the highest dosimetry for ABT-806i, although the dose received from a tracer infusion of ABT-806i is well within acceptable levels and consistent with other 111In-labeled antibodies (15,19). In comparison to imaging of wild-type EGFR, using 111In-225 (20) and 89Zr-cetuximab (21), ABT-806i showed less liver uptake on imaging, with dosimetry and linear pharmacokinetics at low protein doses consistent with lack of normal tissue “sink” as well as tumor-specific EGFR imaging. This imaging illustrated several key observations. First, marked intertumoral heterogeneity exists in nearly a third of patients between different metastatic sites. Second, it is not possible to predict this intertumoral heterogeneity with EGFR testing using archival tissue (or likely even with prospective tissue collection from single tumor sites). Last, the observation that the 1 responder in this study also had the higher ABT-806i uptake suggests a possible use to enrich for patients who will respond to anti-EGFR treatment. Clearly, our results require further validation given the relatively small study size and the heterogeneous patient population. However, the possibility that prospective and contemporaneous assessment of antigen target expression using radiolabeled tracers may affect patient selection for antibody-based therapeutics has been shown by other trials, including T-DM1 (22), and may have an important role in drug development (14,23). Arguably, ABT-806i imaging could present a way to enrich for responders for therapy with ABT-414, which comprised ABT-806 conjugated to monomethyl auristatin F (MMAF) (24). When selection on EGFR amplification in archival tissue was used, adding ABT-414 to standard postoperative chemoradiation did not improve survival in newly diagnosed patients (25); however, there was a trend, though not statistically significant, toward survival benefit when combining ABT-414 with temozolomide in patients with recurrent glioblastoma (26). In both studies, the need for better patient selection for highly targeted drugs such as ABT-414 was emphasized (25,26), and imaging with ABT-806i could represent one way to do so.
CONCLUSION
This study has established the safety and feasibility of molecular imaging of intratumoural EGFR expression using ABT-806i scanning and illustrates possible roles in the development of antibody-based therapeutics.
DISCLOSURE
AbbVie provided financial support for this study (M11-849, NCT01472003) and participated in the study design, conduct, analysis, and interpretation of data, as well as the writing, review, and approval of the manuscript. Hui K. Gan received honoraria, travel support, or research funding from AbbVie, BMS, Eisai, EMD Serono, and MSD. Matthew Burge served on advisory boards and received honoraria from Roche, Amgen, and Sirtex. Benjamin Solomon served on advisory boards and received honoraria from Pfizer, Merck, Roche-Genetech, AstraZeneca, Bristol-Myers Squibb, and Novartis. Kyle D. Holen, Wijith Munasinghe, JuDee Fischer, Peter Ansell, Gerard Fox, Hao Xiong, Edward B. Reilly, and Rod Humerickhouse are employees of AbbVie and may own stock. Yumin Zhang is a previous AbbVie employee and may own stock. Marika Ciprotti is an employee of Bristol-Myers Squibb and may own stock. Andrew M. Scott received research funding and travel support from AbbVie; received research funding from Daiichi-Sankyo, Merck, Telix, Avid, Celgene, ITM; and is a consultant for and has stock in Life Science Pharmaceuticals. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is ABT-806i safe and does it have acceptable radiation dosimetry?
PERTINENT FINDINGS: We demonstrate the ability to successfully obtain real-time imaging of EGFR conformational expression in tumors.
IMPLICATIONS FOR PATIENT CARE: Our data provide support for the use of theranostics to guide patient selection for EGFR-targeting therapies.
ACKNOWLEDGMENTS
We thank Mrinal Shah, PhD, for medical writing support, and Thomas Merdan, PhD, for technical support and assistance (both of Abbvie).
Footnotes
Published online Jan. 28, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 8, 2020.
- Accepted for publication September 16, 2020.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.