


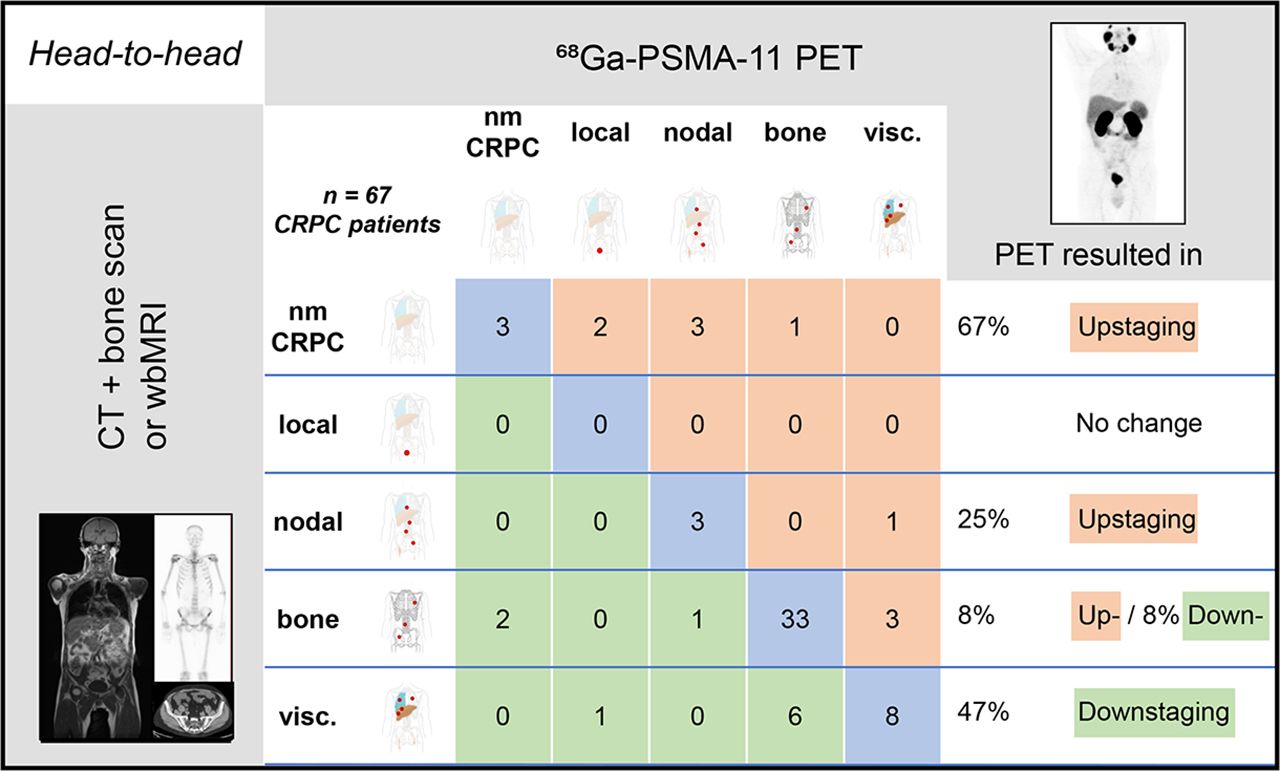
Visual Abstract
Abstract
Prostate-specific membrane antigen (PSMA)–ligand PET is potentially useful for screening of castration-resistant prostate cancer (CRPC) clinical trial target populations. We investigated the impact of PSMA PET on Prostate Cancer Clinical Trials Working Group 3 (PCWG3) clinical subtype classification when compared with conventional imaging (CI). Methods: A multicenter retrospective study enrolled patients who had undergone PSMA PET for CRPC, had prostate-specific antigen values of at least 1 ng/mL, and had undergone CI—that is, CT plus bone scanning or whole-body MRI. The clinical PCWG3 subtype was determined for PET versus CI by 3 masked readers. Results: Sixty-seven patients were included, and PSMA PET led to up-staging in 15% (10/67) of patients; of these, 6 of 10 (60%) had nonmetastatic CRPC on CI. PSMA PET resulted in down-staging in 15% (10/67) of patients. Agreement for PET versus CI PCWG3 clinical subtypes was 0.81 versus 0.51, 0.74 versus 0.47, 0.95 versus 0.72, or 0.59 versus 0.66 for local, nodal, bone, or visceral disease, respectively. Conclusion: Despite 70% concordance with CI, PSMA PET demonstrated superior reproducibility and accuracy especially for non-metastatic CRPC and should be implemented in future clinical trial entry procedures.
Prostate cancer is the second leading cause of cancer mortality in men worldwide (1). Patients initially respond to hormonal therapy but eventually develop potentially fatal castration-resistant prostate cancer (CRPC) (2). In 2016, the Prostate Cancer Clinical Trials Working Group 3 (PCWG3) summarized CRPC clinical trial recommendations, defining 5 clinical CRPC target populations based on pattern of spread, ranging from nonmetastatic to visceral metastatic CRPC. PCWG3 recommends conventional imaging (CI), that is, bone scanning (BS), CT, or whole-body MRI, as standard imaging modalities (3). Since PCWG3, PET with small-molecule ligands that bind to cell-surface prostate-specific membrane antigen (PSMA PET) have been introduced widely. In patients with biochemical recurrence and a low prostate-specific antigen (PSA) level, PSMA PET proved to have superior accuracy for recurrent prostate cancer staging (4) when compared with the recently approved fluciclovine PET (5). PSMA PET further localized metastases in more than half of patients with nonmetastatic CRPC by CI (6) and detected a higher tumor load in CRPC patients with bone metastases on previous BS (7). We therefore hypothesized that PSMA PET offers more accurate and reproducible identification of PCWG3 CRPC clinical trial target populations and will lead to considerable stage migration when compared with CI.
MATERIALS AND METHODS
Study Design and Participants
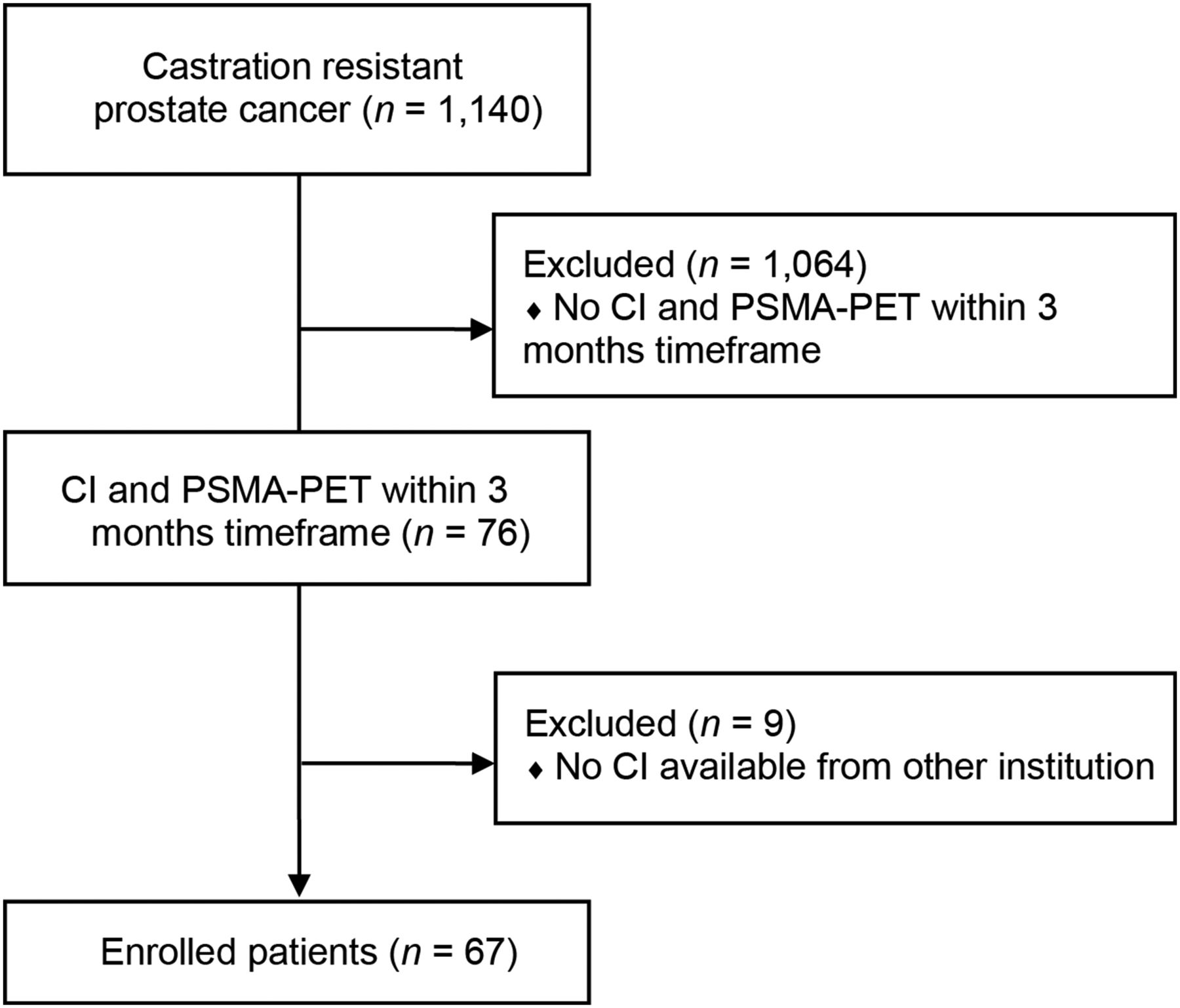
Datasets from 1,140 CRPC patients at 3 participating high-volume PET Centers (University of Bologna, University Hospital Essen, and Technical University Munich) were retrospectively screened for patients with prostate cancer who had undergone PSMA PET between January 2014 and January 2019, had PSA values of at least 1 ng/mL at the time of PET in accordance with PCWG3 (3), and had undergone BS along with CT or whole-body MRI within 3 mo of the PSMA PET without changes in therapy between staging modalities. The patient flow is demonstrated in Figure 1. Approval was obtained by the University of Duisburg–Essen ethics committee (18-8153-BO). All patients gave written consent to undergo PSMA PET. The prerequisite to obtain informed consent for inclusion in this retrospective analysis was waived by the ethics committee.
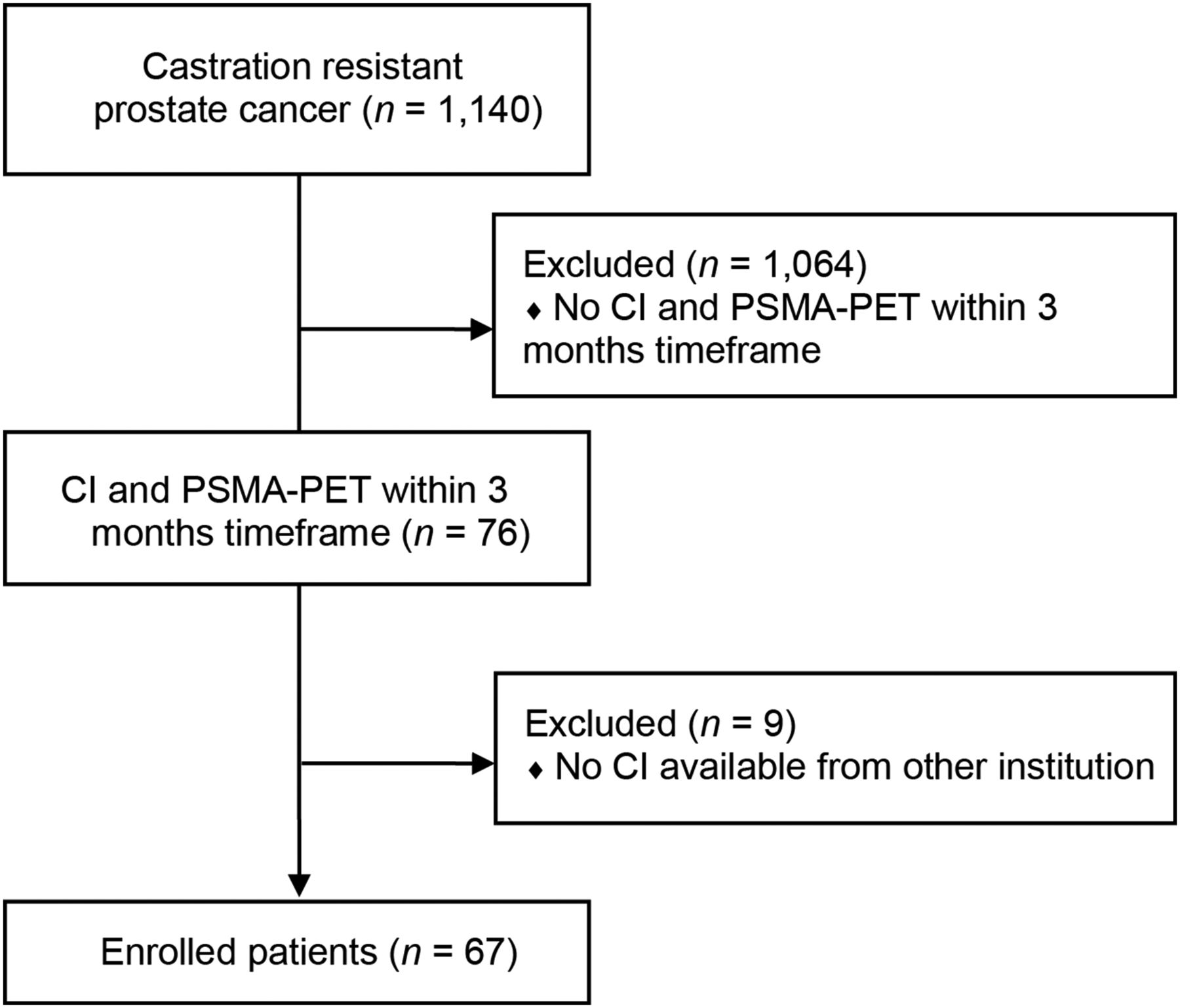
Consort diagram for patient selection.
CRPC Subtypes and Stage Migration
PCWG3 clinical subtypes were, by ascending stage, nonmetastatic CRPC, locally recurrent disease only, nodal spread (with or without local relapse), bone disease (with or without local or nodal disease), and visceral disease (with or without local or nodal or bone disease). Up-staging was defined as any shift to a higher stage; down-staging was defined as any shift to a lower stage.
Imaging Procedures
68Ga-PSMA-11 PET was acquired in accordance with the international guideline as part of a PET/CT (n = 52) or PET/MRI (n = 15) examination (8). Of 67 examinations, 58 (87%) were performed with radiographic contrast enhancement. Attenuation correction was based on the diagnostic CT (PET/CT) or a separate Dixon-based sequence (PET/MRI).
PET
Patients received, on average, 137 MBq (range, 111–159 MBq) of 68Ga-PSMA-11. Image acquisition was started at an average of 64 min (range, 51–68 min) after injection. The PET was reconstructed by ordered-subset expectation maximization–based algorithms. Data from the CT or MRI were used for attenuation correction.
CT
A full-dose CT scan was acquired from the skull base to the mid thigh. Automatic dose modulation was applied with a tube voltage of 120 kV (200–240 mAs). Iodinated intravenous contrast was given 70 s before image acquisition.
MRI
Whole-body MRI was performed on an integrated 3-T PET/MRI scanner using high-channel surface coils. The field of view was from the skull base to the mid thigh, and the protocol consisted of, first, a simultaneous PET and 3-dimensional Dixon volumetric interpolated breath-hold examination for scatter correction; second, a diffusion-weighted sequence with b-values of 50, 500, and 1,000; and third, a standardized whole-body MRI protocol including an axial T1-weighted volumetric interpolated breath-hold examination after administration of gadolinium.
BS
An average of 683 MBq (range, 606–947 MBq) of 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid or 99mTc-hydroxydiphosphonate was given intravenously. Delayed whole-body imaging was performed 2–4 h after tracer injection (matrix size, 128 × 128 or 256 × 256). SPECT imaging was obtained depending on the recruiting center’s protocol.
Image Interpretation
Clinical PCWG3 subtype was determined for PET versus CI by 3 masked readers using published criteria after dedicated reader training (9–11). PET datasets included PSMA PET with CT or MRI; CI datasets included CT and BS (n = 52) or whole-body MRI (n = 15). Datasets were read separately and independently after anonymization and randomization with more than 2 wk between PET and CI reading sessions. Readers were familiar with the patients’ most recent PSA value and prior treatments but were masked to other imaging findings and clinical data. OsiriX MD (Pixmeo SARL) was used for the central readings. Consensus (positive vs. negative) was determined by majority vote.
Statistical Analysis
For continuous data, mean ± SD, median, and interquartile range were reported, whereas categoric variables were described using absolute and relative (%) frequencies. The PSMA PET and CI positivity rate for localization of disease was determined on a patient basis stratified by PSA at the time of the scan. The Pearson χ2 test or Fischer exact test was used to evaluate associations between categoric variables, including International Society of Urologic Pathologists grade group, T stage, N stage, D’Amico risk group, chemotherapy naive, and first and second lines of therapy. Because of an asymmetric distribution of PSA, its association with PSMA or CI positivity was assessed with the nonparametric Mann–Whitney test. When the effect of categoric variables was assessed against a symmetric continuous variable (SUVmax), a linear model with ANOVA was used. Interobserver agreement was determined by the Fleiss κ and interpreted by the criteria of Landis and Koch (12). Statistical analysis was conducted with Stata statistical software, version 13 (StataCorp), and a P value of less than 0.05 was considered significant.
RESULTS
Patient Characteristics
Sixty-seven patients were included (Technical University of Munich, 35 [52%]; University Hospital Essen, 24 [36%]; and University of Bologna, 8 [12%]). The patient characteristics are given in Table 1. The median PSA level at the time of PSMA PET was 53.2 ng/mL (interquartile range, 5.8–334.6 ng/mL). Within 3 mo before or after PSMA PET or as part of the PSMA PET assessment, 52 of 67 (78%) patients had CT and BS, and 15 of 67 (22%) had whole-body MRI. The median time between PSMA PET and CI was 1 mo (interquartile range, 0–2 mo). The median PSA level at the time of CI was 28.7 ng/mL (interquartile range, 3.0–7.5) in the whole-body MRI group and 122.3 ng/mL (interquartile range, 28.3–388.8) in the CT/BS group. Regarding previous therapies, 41 of 67 (61%) patients were abiraterone/enzalutamide/apalutamide-naïve and 41 of 67 (61%) were chemotherapy-naïve; 12 of 67 (18%) were previously treated with 223Ra.
Patient Characteristics (n = 67)
Lesion Detection
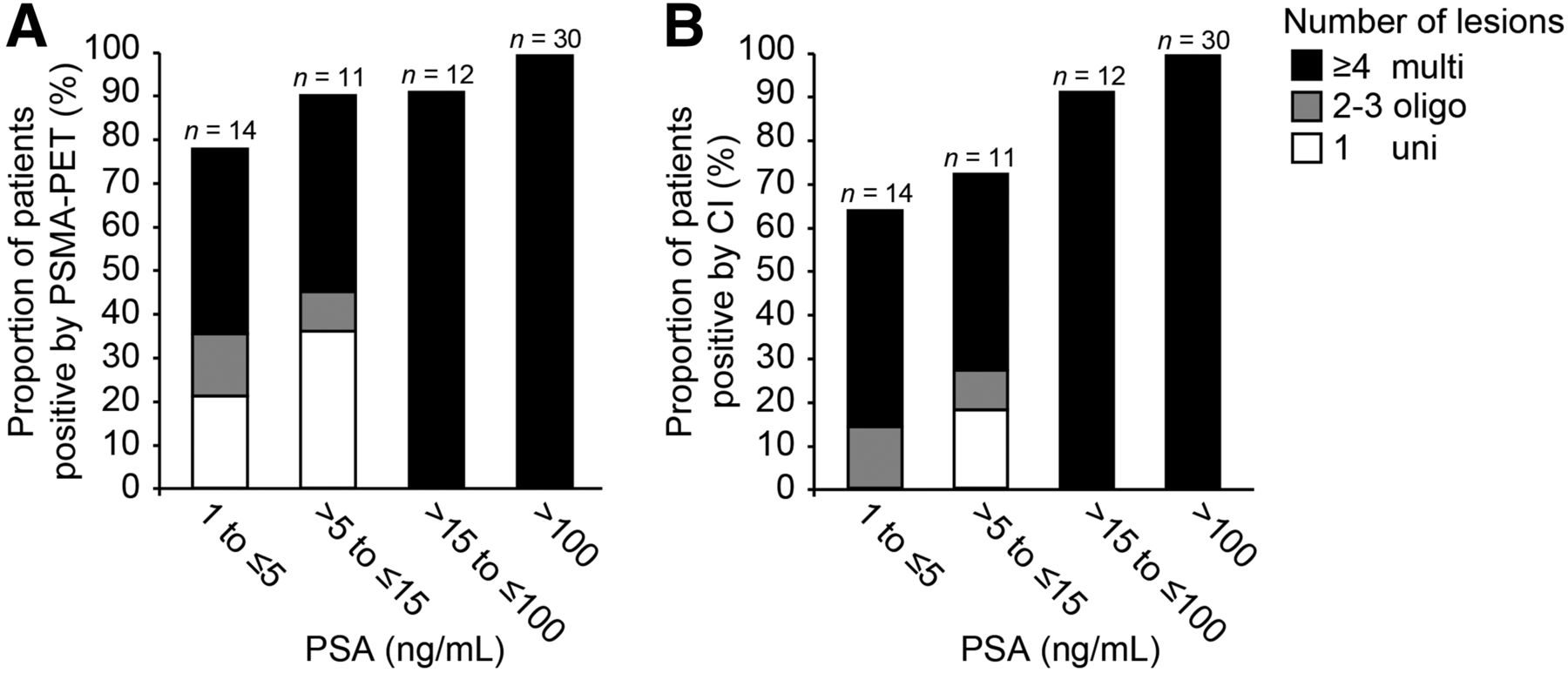
Overall, CI was positive in 87% (58/67) of patients, and PSMA PET was positive in 92% (62/67). The positivity rates of CT, BS, and whole-body MRI were 96% (50/52), 90% (47/52), and 47% (7/15), respectively. The probability of detecting any lesion was associated with the PSA level at the time of the scan (P = 0.032 for PSMA PET and P = 0.002 for CI). PSMA PET versus CI disease burden is shown in Figure 2. Details on lesion size and SUV are given in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org).

PSMA PET (A) and CI (B) positivity rate on patient basis stratified by PSA and number of lesions. multi = multifocal; oligo = oligometastatic; uni = unifocal according to PROMISE criteria.
PCWG3 Subtype
CI PCWG3 clinical subtype was nonmetastatic, local, nodal, bone, or visceral disease for 13% (9/67), 0% (0/67), 6% (4/67), 58% (39/67), or 22% (15/67), respectively (Supplemental Tables 2 and 3).
Up- or down-staging by PSMA PET is given in Supplemental Table 4. Overall, PSMA PET and CI subtype were discordant in 20 of 67 (30%) patients. PSMA PET led to up-staging in 10 of 67 (15%) patients, 4 of these with migration from nodal or bone to visceral disease and 6 with a shift from nonmetastatic to locally recurrent (n = 2), nodal (n = 3), or bone (n = 1) disease. PET led to down-staging in 10 of 67 (15%) patients; 7 of these had CI visceral disease in the lungs (n = 5), liver (n = 2), or adrenal (n = 1), and 3 had bone involvement ruled out by PSMA PET. Lesion validation in 7 patients demonstrated both true-negative (n = 2, 25%) and false-negative (n = 3, 38%) PSMA PET interpretation (Supplemental Table 5).
There was a statistically significant association between higher D’Amico risk group and PSMA PET down-staging compared with CI (P = 0.003); PSA at the time of PET or number of systemic therapies was not significantly associated with stage migration.
Interobserver Agreement
Agreement for PET versus CI PCWG3 clinical subtype was 0.81 versus 0.51, 0.74 versus 0.47, 0.95 versus 0.72, or 0.59 versus 0.66 for local, nodal, bone, or visceral disease, respectively. Agreement for nonmetastatic CRPC was 0.46 for PET and not measurable for CI (n = 0) (Supplemental Tables 6 and 7).
DISCUSSION
PSMA PET previously demonstrated unprecedented accuracy for tumor localization in patients with prostate cancer biochemical recurrence and nonmetastatic castration-resistant disease (4,6). Diagnostic value was validated by histopathology, management changes, and survival in several trials (4,6,13–15). Imaging is essential for identification of CRPC clinical trial target populations. However, the impact of PSMA PET on CRPC PCWG3 staging remains unknown. Here, we assessed in a retrospective multicenter study the potential shift in PCWG3 clinical subtype by PSMA PET when compared with CT plus BS or whole-body MRI. Most patients had advanced disease (80% with CI bone or visceral metastases) with previous CRPC systemic therapy. PSMA PET demonstrated higher reproducibility, except for visceral disease, and detected additional lesions, especially in patients with a PSA level of no more than 15 ng/mL leading to up-staging of CI nonmetastatic CRPC. On the other hand, PET demonstrated somewhat lower reproducibility and did not detect organ lesions, leading to down-staging in patients with CI visceral disease (16–19). Lesion validation indicated false downstaging by PSMA PET in some patients. False-negative interpretations for dedifferentiated organ metastases are a known limitation of PSMA PET. Although the previously reported high accuracy in biochemical recurrence and nonmetastatic CRPC cohorts suggests true findings by PSMA PET, a systematic lesion validation has not been performed in the presented patients.
Overall, PSMA PET was concordant with CI CRPC subgroups in more than two thirds of patients, especially in patients with bone metastatic disease. Both PET and CI detected multifocal disease in almost all patients with more advanced disease (PSA > 15 ng/mL). Here, we demonstrated that PSMA PET is a highly reproducible staging tool for advanced CRPC, with high concordance with CI. Our findings encourage a shift in the current CRPC imaging choice: PSMA PET should be included in future CRPC clinical trial entry and potentially also endpoint assessments. Implementation with careful assessment of visceral lesions is expected to improve patient selection, thereby increasing the probability of trial success and the reproducibility of findings. Follow-up PSMA PET will generate exploratory analyses, such as for CRPC outcome prediction.
Limitations of our study include its retrospective single-center design, small sample size, lack of systematic follow-up, heterogeneous imaging modalities, use of the CT and whole-body MRI as part of a PSMA PET examination, and use of PSMA PET versus CI readings by the same reader group.
CONCLUSION
PSMA PET was highly reproducible and resulted in PCWG3 subtype migration in 30% of patients, especially in patients with CI nonmetastatic disease. Subtypes were concordant in 70% of patients, especially in patients with a PSA level of more than 15 ng/mL or bone metastatic disease. PSMA PET should be implemented in future CRPC clinical trial entry procedures.
DISCLOSURE
Wolfgang P. Fendler is a consultant for Ipsen, Endocyte, and BTG; received personal fees from RadioMedix outside the submitted work; and received financial support from the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG, grant FE1573/3-1/659216), Mercator Research Center Ruhr (MERCUR, An-2019-0001), IFORES (D/107-81260, D/107-30240), Doktor Robert Pfleger-Stiftung, and Wiedenfeld-Stiftung/Stiftung Krebsforschung Duisburg. Ken Herrmann reports personal fees from Bayer, Sofie Biosciences, SIRTEX, ABX, Adacap, Curium, and Endocyte; grants and personal fees from BTG; personal fees from IPSEN; personal fees and nonfinancial support from Siemens Healthineers; and nonfinancial support from GE Healthcare, outside the submitted work. Boris Hadaschik reports grants from German Cancer Aid, the German Research Foundation, and Profound Medical; grants, personal fees, and nonfinancial support from Janssen; personal fees and nonfinancial support from Astellas, Bayer, BMS, Lightpoint Medical, Astra Zeneca, and Sanofi; and grants and personal fees from Uromed, all outside the submitted work. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is PSMA-ligand PET accurate and reproducible in identifying CRPC clinical trial target populations as compared with CI and according to PCWG3 clinical subtypes?
PERTINENT FINDINGS: In this retrospective multicenter study, PSMA-ligand PET was highly reproducible and resulted in PCWG3 subtype migration in 30% of patients, especially in patients with nonmetastatic disease at CI. Subtypes were concordant in 70% of patients, especially in patients with a PSA level of more than 15 ng/mL or bone metastatic disease.
IMPLICATIONS FOR PATIENT CARE: PSMA-ligand PET should be implemented in future clinical trial entry procedures for patients with castration-resistant prostate cancer.
Footnotes
Published online Sep. 11, 2020.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication April 5, 2020.
- Accepted for publication August 6, 2020.





{kind=link}
{kind=link}
{kind=link}