


Abstract
Prostate-specific membrane antigen (PSMA) is highly expressed on most prostate cancer (PCa) cells, and several PSMA ligands for PET imaging are now available worldwide. 68Ga-PSMA-11 has already received U.S. Food and Drug Administration and European Medicines Agency approval, and use of PSMA PET is currently suggested by several international guidelines for investigating PCa in different clinical settings. In primary PCa, PSMA PET has been shown to be superior to cross-sectional imaging for the detection of pelvic lymph nodes and distant metastases with subsequent clinical management changes. Additionally, it might also have a role in intraprostatic tumor localization, especially when combined with multiparametric MRI. In a setting of PCa recurrence, higher detection rates have been observed than for any other available imaging techniques, especially at low prostate-specific antigen values. Furthermore, PSMA PET consistently led to a shift in clinical management, thus increasing the proportion of radiotherapy, surgery, or other focal therapies at the expense of systemic options or no treatment. In oligometastatic disease after radical surgery, PSMA PET may be relevant in guiding a metastasis-directed therapy approach, as preliminary data seem to suggest a benefit in terms of progression-free survival after treatment of PSMA PET–positive lesions. As a staging and gatekeeping technique, PSMA PET represents a reliable whole-body imaging procedure in combination with second-line therapy of castration-resistant PCa, as well as being pivotal when assessing patients eligible for radioligand therapy such as 177Lu-PSMA. This critical review aims at providing a comprehensive overview of the latest literature on the current or emerging main indications, as well as a general outlook on the recommended interpretation criteria for PSMA PET imaging.
Prostate cancer (PCa) is the most common malignancy in men and is associated with high morbidity and mortality rates (1). MRI and different PET radiotracers have been extensively used to improve the accuracy of conventional imaging, namely CT and bone scintigraphy, at all times during the natural history of PCa. Choline, labeled with either 11C or 18F, and 18F-fluciclovine are still broadly used as metabolic PET tracers in clinical practice, and their role for imaging biochemical recurrence (BCR) and their impact on therapeutic management have been demonstrated in clinical trials (2–5). Other PET tracers, such as gastrin-releasing polypeptide receptor–targeting radiopharmaceuticals, show promising results at various stages of PCa, and data from prospective trials are awaited before translation of these tracers into clinical practice (6). The emerging data suggest that novel prostate-specific membrane antigen (PSMA)–based radioligands carry the highest diagnostic value in the imaging of PCa (7). PSMA is overexpressed in most PCa cells and is associated with higher prostate-specific antigen (PSA) values and a higher International Society of Urologic Pathologists (ISUP) grade at diagnosis, as well as with a worse overall survival. However, PSMA has shown a marked inter- and intrapatient heterogeneity (8). The nuclear medicine community has come a long way since the first in-human applications of 68Ga-PSMA-11, which date back to 2012. Its approval by the European Medicines Agency and the U.S. Food and Drug Administration at production sites only in late 2020 marks an important step toward its wide acceptance, but this approval does not represent an endpoint to its further use in the molecular imaging of PCa (9). Prospective, randomized clinical trials incorporating PSMA imaging will probably soon be published; their results are needed to provide even more robust evidence of its role in improving patient outcome. Several PSMA ligands have been synthesized on the basis of both small urea-based molecules and antibodies bound with 68Ga rather than 18F or other isotopes that are used in PET and SPECT (10–16), and more radiolabeled PSMA ligands are expected in the future (Table 1). However, a detailed analysis of the differences in diagnostic performance for PSMA radiopharmaceuticals goes beyond the scope of this review. The aim of this critical review is to highlight use of the already established or currently emerging diagnostic applications of PSMA compounds during the natural history of PCa.
PSMA Ligands Commonly Used in Clinical Practice for Imaging and Therapy
INTRAPROSTATIC CANCER DETECTION
The detection, characterization, and better definition of intraprostatic foci of PCa are among the most relevant emerging applications of PSMA PET imaging. In association with multiparametric MRI (mpMRI), PSMA PET may be used to detect the need for, and subsequently to guide, a targeted biopsy in patients presenting with clinically suspected PCa. Furthermore, PSMA PET might improve the accuracy of segmentation before radiation therapy or other localized treatments, offer a noninvasive characterization of unclear findings, and provide prognostic information.
Biopsy Guidance
mpMRI should be performed on all subjects presenting with clinically suspected PCa before any biopsy attempt in order to guide the biopsy to significant foci in accordance with the most recent recommendations (17). In this setting, PSMA PET might increase the accuracy of mpMRI, mostly in patients with a high clinical suspicion when mpMRI results are negative (Prostate Imaging–Reporting and Data System 1–2) or inconclusive (Prostate Imaging–Reporting and Data System 3). Bodar et al. mapped foci of increased PSMA uptake within the prostate gland in 30 patients prospectively studied with 18F-DCFPyL PET/CT before radical prostatectomy (RP) (18). The targeting of PSMA PET findings on a later biopsy showed PCa-positive lesions in 28 of 30 patients (93%). However, considering all the intraprostatic cancer lesions, sensitivity and specificity for PSMA PET were 61.4% and 88.3%, respectively. Chen et al. used PSMA PET and mpMRI alone or in a hybrid setting (PET/MRI) to improve the detection of clinically significant PCa in 54 men studied before RP, maintaining the final histopathology results as the standard of reference (19). Sixty-six lesions were retrospectively considered clinically significant. The combination of PET and MRI showed a significantly better accuracy than mpMRI alone: sensitivity was 89% versus 76%, respectively (P < 0.01), and specificity was 96% versus 88% (P > 0.05). This improved accuracy was particularly evident when clinically significant lesions occurred within the context of a Prostate Imaging–Reporting and Data System score of 3.
From the limited literature data available, we can conclude that the use of PSMA PET could add diagnostic accuracy in patients with inconclusive MRI results. However, in consideration of the large number of patients who could benefit from PSMA PET and the still limited availability of this method, an extensive application of PSMA PET for this purpose does not appear to be easily feasible. Studies on highly selected populations could in the future clarify the role and the added value of PSMA PET in this context. The ongoing prospective multicenter PRIMARY clinical trial will measure and compare the sensitivity, specificity, positive predictive value, and negative predictive value of both mpMRI and PSMA PET versus targeted prostrate biopsy (20). The results will be used to determine the proportion of men who could safely avoid biopsy without compromising detection of clinically significant PCa.
Segmentation for Radiation Therapy or Guidance of Other Focal Therapies
Bettermann et al. showed a better accuracy for PSMA PET than for mpMRI for intraprostatic gross tumor volume (GTV) delineation. The authors prospectively performed PSMA PET and mpMRI on 17 patients who were candidates for RP (21). GTV contours for mpMRI and PSMA PET were drawn and compared with final GTVs drawn on histopathology images. Median tumor volumes were 10.4 cm3 for GTVs drawn on histology images, 10.8 cm3 for GTVs drawn on PSMA PET images, and 4.5 cm3 for mpMRI. Sensitivity and specificity were 86% and 87%, respectively, for PSMA PET; 58% and 94%, respectively, for mpMRI; and 91% and 84%, respectively, for the combination of both techniques.
Characterization of Intraprostatic Findings and Prognostic Information
Using a similar study design, Scheltema et al. retrospectively enrolled 56 patients who underwent mpMRI and PSMA PET before RP (22). PSMA PET was accurate in detecting prostate segments containing ISUP grade 2–3, if compared with mpMRI, and it may have a role in diagnosing or monitoring PCa. Roberts et al. retrospectively enrolled 71 patients who had MRI-guided, biopsy-proven PCa and in whom PSMA PET was performed before surgery (23). PSMA uptake in the prostate has been correlated with adverse pathology outcomes and progression-free survival, with a minimum follow-up of 24 mo. PSMA PET provided reliable prognostic information, especially in patients with biopsy-proven Gleason 3 + 4 disease potentially suitable for active surveillance or focal therapy.
On the basis of the available literature, and considering the anticipated widespread use of highly sensitive PET tomographs, we believe it is reasonable to suppose that PSMA PET will soon be a routine part of the diagnostic flowchart in many PCa patients before biopsy or primary therapy.
STAGING
A correct assessment of the tumor extension at onset is crucial to establish the correct therapeutic strategy after primary staging. In this setting, PSMA PET for lymph node and bone spread detection has shown high specificity and positive predictive values but a suboptimal sensitivity, which remains, however, significantly higher than that of conventional imaging (7). In the most recently published metaanalysis, the results of 11 studies, including 904 intermediate- or high-risk patients, were grouped: pooled sensitivity and specificity on a patient basis were 63% (95% CI, 0.46–0.78) and 93% (95% CI, 0.88–0.96), respectively (24). On a lymph-node basis, they were 70% (95% CI, 0.49–0.85) and 99% (95% CI, 0.96–1.00), respectively. The pooled positive predictive value and negative predictive value were above 80% whether in a per-patient or a per-node analysis. The recently published results of the proPSMA study are a game changer in staging high-risk PCa patients (25). The proPSMA study is the first multicentric, 2-arm, randomized study aimed at investigating whether PSMA PET may show an improved accuracy when compared with conventional imaging or if it may end up replacing conventional imaging as the only imaging method to perform in high-risk PCa patients at disease presentation. The study included 302 high-risk patients: 152 were randomly assigned to the conventional imaging diagnostic flowchart and 150 to PSMA PET only. The results were validated by a composite reference standard including histopathology, imaging, and laboratory data. At final diagnosis, 30% of the patients showed local or distant metastatic disease. PSMA PET showed greater accuracy than conventional imaging, 92% versus 65%, respectively; better sensitivity, 85% versus 38%; higher impact on clinical decisions, 28% versus 15%, and a lower number of indeterminate findings, 7% versus 23%. The authors concluded that PSMA PET may replace conventional imaging when staging high-risk patients. Nevertheless, the main drawback is that in men undergoing radiotherapy, histologic confirmation of nodal disease was not performed, and some patients might have had microscopic disease that was missed by either conventional imaging or PSMA PET. Wondergem et al. studied 160 high-risk patients at presentation with a fluorinated PSMA compound (18F-DCFPyL) (26). PSMA PET correctly identified 81 of 90 (90%) patients with local or distant metastatic spread at final diagnosis. PSMA PET detected additional lymph node metastases in almost all patients (41/42) for whom CT was already positive in at least 1 lymph node. PSMA PET determined a significant shift in patient management in 17% of the population. In accordance with the proPSMA study, the authors concluded that PSMA PET might be considered the first-line imaging modality for high-risk PCa at presentation, with no need for further diagnostics (Supplemental Fig. 1; supplemental materials are available at http://jnm.snmjournals.org). In a recent prospective multicenter single-arm, open-label phase 3 trial, the accuracy of PSMA PET in the detection of N1 status was assessed in 277 intermediate- or high-risk patients at presentation (27). At final diagnosis, 27% of the patients were N1 at histopathology. On a region-based analysis, sensitivity and specificity by PSMA PET in N1 detection were 40% and 95%, respectively. Higher PSA values and larger nodes were correlated with increased sensitivity by PSMA PET. According to the available data and the foreseeable increase in PSMA PET use before primary treatment, it stands to reason that future inclusion of PSMA PET within the main international guidelines can be expected, at least in a setting of high-risk PCa at disease presentation. Moreover, a cost-effectiveness analysis developed using data from the proPSMA study demonstrated greater accuracy and lower direct comparative costs for PSMA PET than for conventional imaging, namely CT and bone scanning (28).
BCR
Imaging in PSA persistence or recurrence after radical treatment aims at treatment changes and thus possibly a better clinical outcome. PSMA PET demonstrated higher sensitivity than 11C-choline or 18F-fluciclovine PET in this setting (29,30), and scan positivity increases with higher PSA values (7). A common limitation of PSMA PET for this purpose is the lack of robust validation of PSMA PET–positive findings and lack of accurate evaluation of its impact on outcome, since most of the data are retrospective or with a short median follow-up time. However, numerous data confirm a significant impact of PSMA PET at least on clinical management. A metaanalysis investigating the impact of PSMA PET on management of BCR patients (11 studies, 908 patients) reported changes in 54% of patients, although substantial heterogeneity among the included studies was noted—that is, differences in clinical settings, types of initial definitive treatment, and baseline characteristics (31). Between 5% and 20% of men continue to have detectable PSA after RP (most often defined as PSA ≥ 0.1–0.2 ng/mL within 4–8 wk from surgery). This condition is often associated with poor prognosis. In this patient setting, retrospective studies report a PSMA PET positivity rate ranging from 67% to 70% (32–34). According to the European Association of Urology guidelines, PSMA PET is the most sensitive imaging modality to detect metastasis in this patient setting and should be offered to patients with a PSA higher than 0.2 ng/mL after RP (Table 2) (35). In a large single-arm, multicenter prospective study, 635 patients with BCR after RP (41%), radiation therapy (27%), or both (32%) were enrolled, with the main aim of evaluating the positive predictive value and the detection rate of PSMA PET (36). PSMA PET showed recurrent PCa in 75% of patients. The positive predictive value was 0.84 in the 87 patients validated by histopathology and 0.92 in the 217 patients validated by the composite reference standard. As expected, the PSMA PET detection rate was associated with increased PSA values, ranging from 38% in patients with a PSA lower than 0.5 ng/mL to 97% in those with a PSA higher than 5.0 ng/mL. These data confirm that higher serum PSA levels are associated with PSMA positivity in BCR. Careful patient selection using nomograms has been proposed to maximize the probability of a positive PSMA PET result, implementing clinical parameters such as ISUP grades, current androgen-deprivation therapy (ADT), time to BCR, clinical stage, and PSA kinetics, with areas under the receiver-operating-characteristic curve ranging from 0.69 to 0.76 (37,38). In one study, Rauscher et al. included 272 hormone-sensitive patients with previous RP and PSA values between 0.2 and 1.0 ng/mL at the time of PSMA PET (37). Among those, about 10% were on ADT at the time of the PSMA PET scan. In a multivariable regression model, ADT administration and PSA values were identified as the most relevant predictors of positive PSMA PET results. Similarly, Ceci et al. included 703 patients with PSA failure after RP, stratified according to different clinical settings, that is, first BCR, recurrence after salvage treatment, PSA persistence after radical surgery, and advanced stage of PCa before second-line systemic therapy (38). In a multivariable regression model, ISUP grade, PSA values, PSA doubling time, and clinical setting were independent predictors of a positive PSMA PET result.
2020 Recommendations on Use of PSMA PET or Next-Generation Imaging (NGI; i.e., PET/CT, PET/MRI and Whole-Body MRI)*
We can conclude that besides PSA values at the time of PSMA PET, concurrent ADT and PSA kinetics were the most relevant predictors of a positive scan in BCR patients. Nevertheless, in clinical daily practice, despite the high detection rates and accurate patient selection, a not-negligible number of patients will have a negative PSMA PET result. A prospective multicenter study (▪▪▪) was performed to evaluate the predictive value of PSMA PET in 260 men with BCR (PSA of 0.26 ng/mL; follow-up of 38 mo) who were candidates for salvage radiotherapy (SRT). Overall, freedom from progression after 3 y was statistically significantly increased in patients with negative PSMA PET results or when PSMA PET showed disease confined to the prostatic fossa, in comparison with patients showing extraprostatic disease (P < 0.0001). It is interesting that in the same population, PSA values were not able to stratify patients with the same statistically significant accuracy.
SRT PLANNING
SRT after RP is associated with PSA control in about 50% of patients. International guidelines suggest performing SRT when serum PSA levels are lower than 0.5 or 1.0 ng/mL (35). At these PSA levels, conventional imaging demonstrated very low sensitivity in detecting sites of recurrence. For this reason, GTVs are usually drawn without imaging guidance. PSMA PET in patients eligible for SRT may improve the likelihood of PSA response and is suggested by the main international guidelines (Table 2) (35,39). Calais et al. enrolled 270 patients after prostatectomy and before SRT who underwent PSMA PET at a PSA level of less than 1 ng/mL (median, 0.48 ng/mL) (40). PSMA PET was positive in 49% of patients and showed the presence of at least 1 lesion out of the planned GTV in 19% (52/270 patients), mostly localized in the bones or in perirectal lymph nodes. PSMA PET findings thus led to a major change in management in 19% of the patients (Fig. 1). In a randomized phase 3 trial aimed to evaluate the success rate of SRT with and without radiation therapy planning based on PSMA PET findings, the primary endpoint was the SRT success rate, measured as biochemical progression-free survival, at 5 y among patients who actually received SRT (41,42). Enrollment is complete: 83 patients in the control arm proceeded with standard SRT, and 102 patients in the investigational arm underwent PSMA PET before SRT planning. Patients in the control group were staged heterogeneously using 18F-fluciclovine PET (33%), CT (36%), bone scanning (17%), MRI (27%), or 18F-FDG PET (1%), and 34% had no imaging. In the intervention group, PSMA PET was positive in 37% of patients, with 9% positive outside the pelvis (M1). This large prospective study will provide useful information about the added value of PSMA PET in patients who are candidates for SRT and whether the impact of PSMA PET on SRT planning would translate into better patient outcomes.
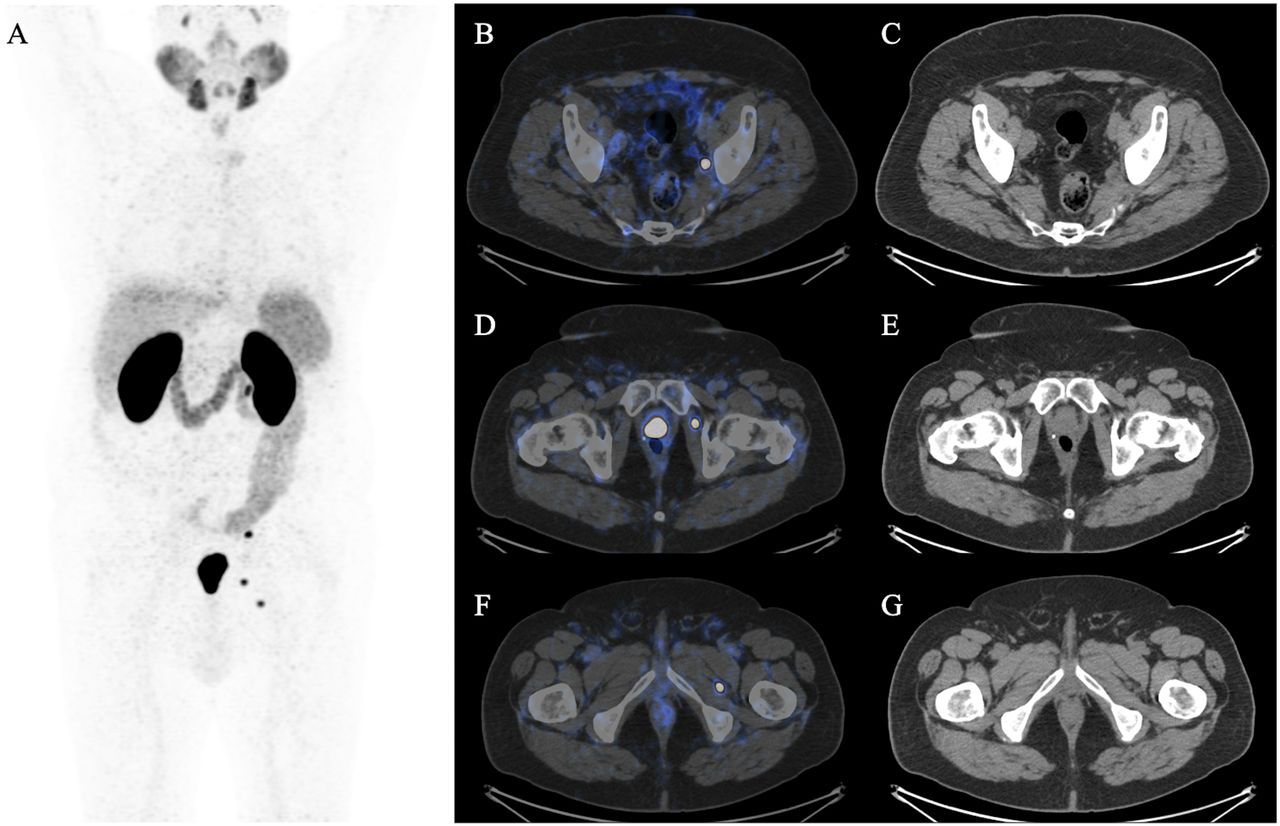
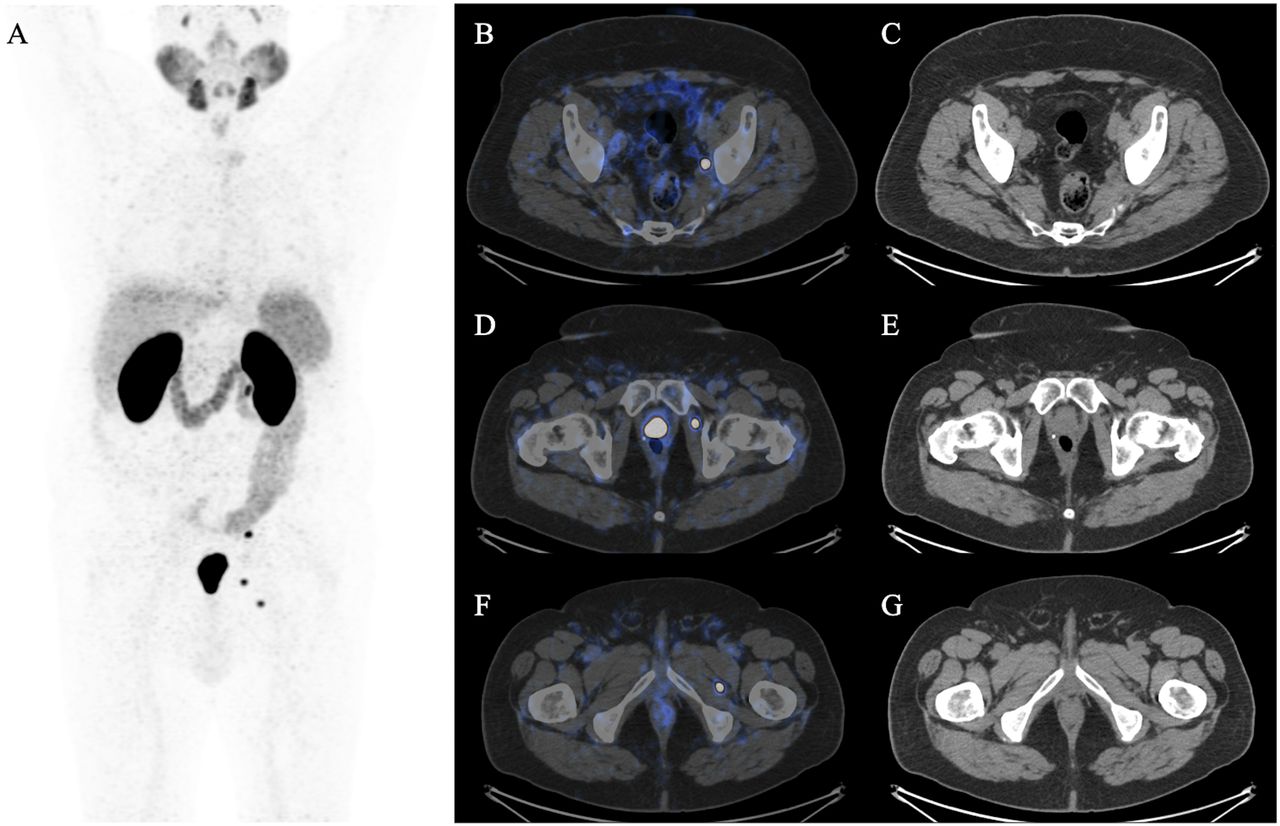
PSMA-guided salvage treatment in 69-y-old man with initial PSA level of 5.1 ng/mL, who underwent robot-assisted laparoscopic prostatectomy and lymph node dissection for adenocarcinoma with neuroendocrine phenotype, ISUP 4, pT3a pN0 (0/11), R0. PSA persistence existed 4 wk after surgery, at 0.73 ng/mL. Patient was referred for PSMA PET before scheduled SRT. PSA level at time of scan was 0.92 ng/mL, with PSA doubling time of 5.2 mo. (A) PSMA PET maximum-intensity projection. (B–G) PSMA PET/CT images and CT images showing 1 right obturator lymph node with PSMA uptake (B and C) and 2 intramuscular lymph nodes with PSMA uptake (D–G). Patient was treated with SRT and simultaneous integrated boosts and showed complete PSA response 9 mo after treatment.
METASTASIS-DIRECTED THERAPIES AFTER RADICAL TREATMENT
The oligometastatic state is proposed as a stage of cancer spread intermediate between localized and systemic disease, enabling a potential opportunity for metastasis-directed therapy to delay the emergence of polymetastatic disease (43). Disease volume and distribution have prognostic implications for patient management, quality of life, and survival, and thus, prompt recognition of oligometastatic PCa is desirable (44). However, the type of imaging that best defines oligometastatic PCa for the purpose of metastasis-directed therapy is debated (45). PSMA-based literature on this topic is mostly retrospective, and the randomized phase 2 ORIOLE (Observation vs. Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer) study is the first clinical trial on PSMA PET–directed salvage therapy (46). Thirty-six patients with hormone-sensitive oligometastatic PCa underwent conventional imaging and were randomized to receive SBRT versus observation alone. Baseline PSMA PET was performed with 18F-DCFPyL, and PSMA PET results were not used for SBRT treatment planning. At baseline PSMA PET, 16 of 36 (44.4%) patients treated with SBRT showed positive findings that were not included in the prescribed treatment fields. Post hoc analysis of progression-free survival based on extent of untreated disease appreciable by PSMA PET found improved progression-free survival and distant metastasis-free survival advantages among men who received consolidation therapy for all PSMA-avid disease (hazard ratio, 0.26; 95% CI, 0.09–0.76; P = 0.006). This means that PSMA PET should be considered for metastasis-directed therapy to maximize patient benefit in oligometastatic PCa and that consolidation therapy in cases of PSMA PET positivity might improve progression-free survival.
CASTRATION-RESISTANT PCA (CRPC)
In CRPC, the number of available treatments is steadily rising over ADT, ranging from novel androgen receptor–targeted therapy (abiraterone, enzalutamide, or apalutamide) to anti–programmed cell death protein 1 and radionuclide therapy. In this setting, conventional imaging is recommended (35) despite the emergence of PSMA PET as an accurate imaging modality for evaluating CRPC patients. A multicenter retrospective study including 200 patients with a PSA level higher than 2.0 ng/mL, negative results on conventional imaging, and a high risk for metastasis (i.e., PSA doubling time ≤ 10 mo or Gleason score ≥ 8) aimed to assess the performance of PSMA PET in nonmetastatic CRPC (47). PSMA PET was positive in 196 of 200 (98%) patients. Overall, PSMA PET showed pelvic disease in 44%, including 24% with local prostate bed recurrence, and distant metastasis in 55% despite negative findings on conventional imaging (Supplemental Fig. 2). The overall accuracy of PSMA PET was 95% for osseous lesions and 60% for soft-tissue lesions. PSMA PET also demonstrated a shift in 30% of patients regarding per-patient Prostate Cancer Clinical Trials Working Group clinical subtype in comparison with conventional imaging, as well as a major concordance with conventional imaging, in a multicenter retrospective analysis of 67 CRPC patients imaged with PSMA PET and CT plus bone scintigraphy or whole-body MRI (48). According to these results, it stands to reason that PSMA PET leads to an earlier detection of metastasis than does conventional imaging and a change in clinical subtype, which may trigger earlier or different treatments. However, whether there could be an impact on overall survival or quality of life has yet to be determined, and further studies are warranted. Additionally, PSMA PET might be useful for selecting patients for the most appropriate treatment. In a retrospective analysis of 80 advanced-CRPC patients treated with 223Ra-dichloride, the final outcome was significantly better in the group of patients studied with PSMA PET before treatment than in those who were staged only with conventional imaging (49). Moreover, assessing PSMA expression is essential for the inclusion criteria in all PSMA-based radioligand therapy trials, since some patients may show low or absent PSMA expression, which is a contraindication for radioligand therapy. Experience derived from 177Lu-PSMA suggests a dual-tracer approach using both PSMA and 18F-FDG for patient selection before treatment (50,51). 18F-FDG–avid disease represents sites of aggressive disease that cannot efficiently be targeted with radioligand therapy. However, an optimal threshold for defining low PSMA expression on PSMA PET has not been defined or validated yet. Further prospective trials are required to elucidate the role of PSMA PET in response assessment and survival prediction. In a retrospective study on PSMA PET before and after 3 cycles of docetaxel, 16 metastatic CRPC patients were evaluated (52). The authors compared PSA decline with the responses on PSMA PET and CT. PSMA PET was better than CT as a predictor of response (56% of the cases for PSMA PET vs. 33% for CT). In another retrospective study, 43 patients with metastatic CRPC underwent PSMA PET before and after systemic therapies (53). PSMA PET parameters, as well as RECIST 1.1 (54), were significantly associated with PSA response. However, neither the investigated PET parameters nor PSA level or RECIST 1.1 were associated with overall survival. This result could be explained by the design of the study and the heterogeneity of treatments and by the lack of standardized criteria to assess response (or progression) at PSMA PET. In this regard, the PSMA PET Progression Criteria were proposed to define disease progression (55), since the criteria of the Prostate Cancer Clinical Trials Working Group include only laboratory parameters and conventional imaging but no molecular imaging (56). The proposed definition of PSMA PET progression in metastatic CRPC is reported in Supplemental Table 1.
ANTIANDROGEN MODULATION OF PSMA
STANDARDIZED REPORTING AND INTERPRETATION
With the increasing diffusion of PSMA PET imaging worldwide, the application of standardized, unique methods to read and interpret images has become mandatory in order to collect reproducible data and increase the accuracy of PSMA PET. Several criteria have been already proposed, and Table 3 summarizes the key features.
PROMISE Criteria
The PROMISE criteria are a suggested standardization for PSMA PET either for reading based on the intensity of PSMA expression (known as miPSMA scores) or for interpretating the images and staging the disease (known as miTNM scores) (64). miPSMA categories were defined in relation to mean PSMA uptake in the blood pool, the liver, and the parotid gland, ranging from 0 to 3. However, the authors of the criteria recommend that image interpretation and the conclusion on disease extent (miTNM scoring) be performed within the clinical context and with consideration of the extent and the location of PET findings. miTNM scores could be used as a guide for a standardized report taking into consideration the presence, location, and extent of local PCa and the pattern of metastases; the PSMA expression level of tumor lesions; and the diagnostic confidence about the reported findings.
PSMA RADS
PSMA RADS is a classification of PSMA PET findings into categories that reflect the likelihood of the presence of PCa (65). Like the other radiologic RADS criteria, the goal of PSMA RADS is to score the level of confidence of the reader on the presence of PCa and the potential need for any additional work-up. The scores for PSMA RADS range from 1 to 5, with higher numbers indicating a greater probability of PCa. In addition, the authors of the classification also recommend that a complete clinical history be collected for each patient, including the current and previous PSA levels, the findings of other imaging modalities, the type and duration of previous therapies, and whether there are other known malignancies.
E-PSMA
The E-PSMA is a comprehensive guideline supported by the European Association of Nuclear Medicine and aims to develop a structured report for PSMA PET images and to harmonize diagnostic interpretation criteria (66). In the suggested structured E-PSMA report, the visual description should relate PSMA uptake to background uptake in the blood pool, liver, and salivary glands on a visual scale of 0–3. For image interpretation, the guideline panelists suggest a 5-point scale of confidence. The document also suggests the use of a standardized terminology in reporting PSMA PET findings and the adoption of a structured report.
CONCLUSION
PSMA ligands for PET imaging have been adopted at an unprecedented rate, resulting in a tremendous increase in published studies and trials. Most importantly, PSMA PET is now part of the diagnostic flowchart of PCa in international guidelines and has received the first regulatory approvals. Several PSMA radiotracers are now available and many more are under investigation, thus increasing the availability of PSMA PET imaging worldwide. Currently, the challenge lies in understanding the mechanisms behind PSMA expression and its influencing factors, either endogenous or exogenous. Furthermore, nuclear medicine physicians will have to familiarize themselves with a standardized reporting system, and a strict collaboration with the clinician remains vital for effective implementation of the PSMA PET imaging results. In short, from now on what we need is the production of reliable data on patient outcome at dedicated endpoints.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENT
We sincerely thank Dr. Alessandro Lambertini for the revision of the manuscript and his friendship.
Footnotes
Published online Mar. 12, 2021
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 19, 2021.
- Accepted for publication March 1, 2021.





{kind=link}