


Visual Abstract

Abstract
Criteria for the behavioral variant of frontotemporal dementia (bvFTD) include decreased frontal metabolism. 18F-FDG PET was used to investigate whether patients with the behavioral variant of neurocognitive disorder (bvNCD) who did not fulfill 3 bvFTD criteria had the characteristic brain metabolic pattern. Methods: Patients were referred from the memory clinic to the nuclear medicine department for differential diagnosis of neurocognitive disorder with dysexecutive syndrome and predominant mild frontal atrophy. When only 2 bvFTD criteria were met, patients were classified into 2 groups before 18F-FDG PET: probable bvFTD (n = 25) or bvNCD (n = 27). Results: Voxel-based and multivariate partial least-squares analyses of 18F-FDG PET did not show significant between-group difference at inclusion. After 4.8 y of follow-up, most patients with probable bvFTD received the same diagnosis, 3 remained stable, and 1 participant was given a psychiatric diagnosis. Five patients with bvNCD fulfilled the criteria for probable bvFTD at a 4.4-y mean follow-up, whereas 2 participants remained stable and 3 received alternative neurologic or psychiatric diagnoses. When initial 18F-FDG PET findings were compared between groups stratified at follow-up (26 bvFTD vs. 17 bvNCD), there was a trend (P < 0.001, uncorrected) for lower prefrontal metabolism with relatively preserved premotor metabolism in bvFTD than in bvNCD. Twelve bvNCD participants had neuropsychologic testing before inclusion. They all presented executive dysfunction and normal visuospatial performance, and most (n = 9) had memory-encoding impairment. Conclusion: Frontal hypometabolism was observed in a dysexecutive presentation of frontal neurodegenerative disorder (bvNCD) that did not fulfill all clinical criteria for bvFTD.
Frontotemporal dementia (FTD) represents about 15% of all neurodegenerative dementias. The onset of the behavioral variant of FTD (bvFTD) is insidious, and early diagnosis is difficult. Revised bvFTD clinical criteria were recently described (1). They state that bvFTD is characterized by progressive deterioration of behavior and cognition. The diagnosis is classified as possible when 3 of the following symptoms are present: early disinhibition, early apathy, loss of empathy, stereotyped or compulsive behavior, hyperorality, and executive deficit with relative preservation of memory and visuospatial functions. The diagnosis becomes probable when frontal or anterior temporal atrophy or hypometabolism can be demonstrated and when significant functional decline is observed at follow-up. bvFTD diagnostic criteria are not achieved when only 2 of these symptoms are observed, irrespective of other factors, including neuroimaging results. This study was performed to determine the outcome of patients with only 2 symptoms suggesting bvFTD. Exclusion criteria correspond to other neuropsychiatric diseases. Effectively, frontal involvement is observed in psychiatric conditions, in parkinsonian disorders, or in a frontal presentation of Alzheimer disease (AD), for example. Among the inclusion criteria, the neuropsychologic profile may be variable, since memory impairment is frequently reported in bvFTD when assessed with specific episodic memory tasks (2). Rascovsky et al. (1) reported 19 patients with pathologically confirmed frontotemporal lobar degeneration who did not meet all bvFTD criteria, and 10 had important memory problems.
The sensitivity and specificity of neuroimaging for the bvFTD diagnosis have been assessed in several studies. One study using volumetric imaging and regions of interest compared bvFTD, semantic dementia, and progressive nonfluent aphasia (3). Each syndrome could be discriminated from each other with high sensitivity (86%–100%) and specificity (89%–100%). Characteristic frontal and temporal metabolic impairment on 18F-FDG PET was shown in bvFTD with different statistical approaches (4,5). In a study of patients with suspected FTD but no characteristic changes on structural imaging, 18F-FDG PET had a relatively low sensitivity of 47% for bvFTD but a high specificity of 92% in a sample with diverse neurologic and psychiatric diagnoses at follow up (6). Yet, 18F-FDG PET was important because it identified bvFTD that could not be diagnosed through structural imaging. Sensitivity and accuracy for detecting FTD are higher with 18F-FDG PET than with MRI (7). Actually, the utility of 18F-FDG PET in distinguishing AD from FTD has long been recognized, and the technique meets many of the ideal characteristics for a biomarker. Notably, it reflects a fundamental FTD pathologic feature, that is, the selective regional pathology in the anterior brain. Accordingly, frontal hypometabolism was already observed in carriers of progranulin mutation predating dementia (8). Interestingly, a phenocopy was described with a slow evolution and no decline in functional activities, in which the initial diagnosis of possible FTD is not accompanied by frontal atrophy or hypometabolism (9). Among the differential diagnoses, frontal hypometabolism can be observed in schizophrenia, depression, or alcohol abuse, for example (10,11). In the latter study (11), a group of patients with initial behavioral changes received, after a 2-y follow-up, a diagnosis of probable or definite bvFTD (24%), other dementia (25%), or psychiatric disorder (40%). The specificity of frontotemporal atrophy on baseline MRI for bvFTD was 95%, reflecting neurodegeneration. The sensitivity of 18F-FDG PET frontal hypometabolism in participants with normal MRI findings was 90%, with a low specificity of 68% because of decreased frontal activity in primary psychiatric cases and other types of dementia (11).
In the present study, we examined successive patients who were referred to the nuclear medicine department for a differential diagnosis of the behavioral variant of neurocognitive disorder (bvNCD) (12), had no major psychiatric disorder, and had variable but predominant frontal atrophy on structural neuroimaging. Our objective was to investigate whether patients with bvNCD who did not fulfill 3 bvFTD criteria had the characteristic brain metabolic pattern. To do so, 2 main subgroups were identified according to clinical symptoms at inclusion and follow-up: patients with probable bvFTD (1) and patients with bvNCD. If there was a specific signature, lower glucose uptake in the medial frontal regions was anticipated in bvFTD patients (4).
MATERIALS AND METHODS
Participants
Patients with neurocognitive disorder as explained in Sachdev et al. (according to the criteria of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders) (12), and with behavioral and cognitive dysexecutive syndrome but no major psychiatric disorders, were referred from the memory clinic to the nuclear medicine department for differential diagnosis. Patients had difficulty with executive functions, frequent memory complaints, minor language or visuospatial disturbance, and a variable number of behavioral symptoms (Table 1). Clinical evaluation of executive difficulties was based on the caregiver’s or patient’s reports of changes in initiative, planning, or organization of activities and on reports and clinical observation of impulsivity, lack of flexibility and deduction, and sometimes poor awareness of difficulties. Most participants had impaired effortful memory recall and improved performance when a choice was given at recognition during medical screening. Neuropsychologic testing was quite variable (from a short screening to a full neuropsychologic battery); behavioral abnormalities reported by the patient and the caregiver were recorded in a standard format according to recent criteria (1), but social cognition was not formally evaluated. We included 52 participants (29 women and 23 men) with predominant frontal (vs. posterior) atrophy at visual inspection of structural 3-dimensional brain images (Table 1). Participants without atrophy were not included to avoid phenocopies of behavioral disorders (9). Patients with probable AD (13) or parkinsonism were not included. At the time of 18F-FDG PET, the population was classified into 2 subgroups, probable bvFTD (n = 25), when 3 or more diagnostic criteria were met, and bvNCD, when only 2 bvFTD clinical criteria were recorded (n = 27). The diagnosis of neurocognitive disorder excluded psychiatric disease and addiction (12). Clinical dementia rating allowed assessment of the severity of dementia (14). Patients were subsequently followed in the memory clinic to record additional diagnostic symptoms, clinical deterioration or stabilization, or alternative neurologic or psychiatric diagnoses.
Demographic and Clinical Characteristics of Frontal Patient Groups
For the sake of comparison with the literature, 18F-FDG PET data from 32 healthy older participants and 52 patients with probable AD (15) were also gathered (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). This study followed the Declaration of Helsinki on medical protocols and ethics and was approved by the Medical Ethical Committee of the University of Liege. All subjects gave informed consent to the use of their data for research purposes.
Neuroimaging
18F-FDG PET and Structural Imaging
18F-FDG PET was performed 30 min after intravenous injection of 150 MBq (±10%) of 18F-FDG, with eyes closed, using a Gemini TF scanner (Philips) with an 18-cm axial field of view and a 4.8-mm resolution in air (axial resolution in the center of the field of view). A low-dose CT scan was acquired for attenuation correction, followed by a 12-min emission scan. Images were reconstructed using a list-mode time-of-flight algorithm including correction for attenuation, dead time, scatter, and random events. Since some of the early healthy participants moved between CT and PET acquisitions, a row-action maximum-likelihood algorithm reconstruction assuming uniform attenuation was performed. Those images were used for all analyses. Reconstructed images had a 2-mm isotropic pixel size and a 128 × 128 × 90 matrix.
As per the protocol, all patients had variable frontal atrophy on structural neuroimaging (brain CT or brain MRI) performed as part of the clinical routine. The global cortical atrophy–frontal subscale scores were visually rated on transverse sections of structural cerebral images (16).
18F-FDG PET Processing and Statistical Analyses
PET data were subjected to an affine and nonlinear spatial normalization onto the Montreal Neurologic Institute space using the SPM12 standard PET brain template (Wellcome Department of Cognitive Neurology) and smoothed using an isotropic gaussian kernel of 8 mm in full width at half maximum. A mean image was generated that served as a study-specific brain template. Each PET image was then spatially normalized onto this brain template and smoothed with an isotropic gaussian kernel of 12 mm in full width at half maximum. Partial-volume effect could not be considered because MRI was not obtained for all participants. The normalized 18F-FDG PET images were entered in a general linear model with a factorial design including the frontal groups, controls, and AD patients, using proportional scaling by cerebral global mean values to take into account the individual variation in global 18F-FDG uptake. Reference tissue was not used because none is recommended in bvFTD. The analyses consisted of comparisons: frontal groups versus control volunteers, frontal groups versus AD patients, and bvFTD versus bvNCD, using age and sex as confounding variables. Significant group differences in regional metabolism were tested with a statistical threshold of P < 0.05, familywise-error–corrected for multiple comparisons at the voxel level, and trends were also searched for (P < 0.001, uncorrected, k > 10). We performed a second analysis on groups defined at follow-up (bvFTD vs. bvNCD), entering patients with other diagnoses as variables of no interest.
We also provided a multivariate approach—using spatiotemporal partial least-square analysis (17)—that operates on voxel metabolic covariance to identify 1 component (latent variable, LV) that optimally distinguishes between 2 groups. We used nonrotated task partial least-squares in which a design matrix comparing 2 conditions (bvFTD vs. controls, bvNCD vs. controls, bvFTD vs. bvNCD) and the image data matrix (1 mean-centered PET image per subject) were submitted to singular value decomposition. The resulting LV has a singular value that represents the amount of covariance between the design matrix and the image matrix. Each brain voxel has a weight (a salience) on the LV that indicates how that voxel is related to the LV. The salience is positive for one group and negative for the other. The significance for the LV was determined by a permutation test. The singular value of each newly permuted LV was compared with the singular value of the original LV, yielding a probability of the number of times the permuted values exceed the original value. Six hundred permutations were conducted, and the statistical significance level was set at a P value of less than 0.05. Finally, the reliability of the saliences for the brain voxels characterizing LV was assessed by a bootstrap analysis of the standard errors using 150 bootstrap samples (18). A reliable contribution for a given voxel was defined as a ratio of salience to SE superior or equal to 3 (cluster size > 5, P < 0.005).
Demographic and clinical data at inclusion were compared between frontal groups using 2-sample t tests or χ2 tests (P < 0.05) in Statistica (StatSoft, Inc.). Additionally, the frequency of clinical bvFTD symptoms was compared between the 2 groups by means of Mann–Whitney tests, with an α-level of 0.05.
RESULTS
Clinical Data
We compared clinical manifestations in the cohort of 52 patients, contrasting the bvFTD group versus the bvNCD group (Table 1).
Patients with bvFTD were younger than patients with bvNCD (t50 = 2.9, P < 0.01). There was a majority of men in the bvFTD group and a majority of women in the bvNCD group (χ2 = 4.85, P < 0.05). The symptom duration did not differ between groups (P = 0.21). Dementia severity was more important in the bvFTD group than in the bvNCD group according to clinical dementia rating (t50 = −3.89, P < 0.001). However, there was no difference in mini mental state exam score at the time of 18F-FDG PET between the 2 groups. A familial history of dementia was reported in 10 bvFTD patients and 6 bvNCD patients. Vascular risk factors were less frequent in the bvFTD group.
Table 1 also presents the frequency of behavioral symptoms in the frontal groups. Comparison revealed that bvFTD patients exhibited more symptoms of disinhibition, apathy, loss of empathy, stereotypes, and hyperorality than did bvNCD patients. BvFTD patients more frequently showed anosognosia than did bvNCD patients (all significant, P values < 0.05). There was no between-group difference for initial complaints regarding executive functioning, memory and visuospatial impairment. bvNCD participants appeared to have more cognitive than behavioral symptoms (Table 1).
Frontal atrophy was mild to moderate in most patients and severe in only few of them. The global cortical atrophy–frontal subscale scores did not differ between groups (t49 = 0.12, P = 0.89). Genetic testing (comprising C9orf72) was obtained in 7 bvFTD and 5 bvNCD participants, and no mutation was observed.
The mean clinical follow-up duration was 4.8 ± 3.1 y for bvFTD patients and 4.4 ± 2.4 y for bvNCD patients. This duration did not differ between groups (t50 = −0.50, P = 0.61). Follow-up did not much modify the group attribution for bvFTD, with 1 psychiatric diagnosis (depression) and 3 participants with no or very slow progression (stable cases). The behavioral symptoms and dependence tended to worsen in the remaining 21 bvFTD patients who met the diagnosis criteria for probable bvFTD at follow-up. Follow-up provided little additional information for a differential diagnosis in the bvNCD group, with 5 participants reaching 3 diagnostic criteria for bvFTD, 2 cases being stable, 1 having vascular dementia, 1 a psychiatric disorder (depression), and 1 alcohol addiction. The other bvNCD cases (n = 17) could not be more precisely defined following bvFTD criteria. All participants with unexpected evolution are identified in the graphical representation of frontal 18F-FDG uptake in the “Brain Metabolism” section. Twelve patients with a bvNCD diagnosis at follow-up (70%) had a full neuropsychologic examination during their diagnostic assessment. The forward and backward digit span results were normal in 11 patients. Long-term memory impairment concerned effortful (executive) retrieval in 11 patients and encoding in 9 patients, whereas intrusions were observed in 4 patients (19). Slowness was recorded in 6 patients when assessing simple conditions in the Stroop experiment (20). Dysexecutive function corresponded to impaired verbal inhibition (20) or planning difficulties for remembering Rey’s figure (21) or perseverations in graphical or motor sequences or impaired verbal fluency. Visuospatial performance was normal, whereas naming was impaired in 3 patients. In summary, the main results of the neuropsychologic evaluation in this sample were dysexecutive functioning in all patients and memory encoding impairment in 9 patients.
Brain Metabolism
Visual reading reported frontal hypometabolism in each patient (Supplemental Fig. 1).
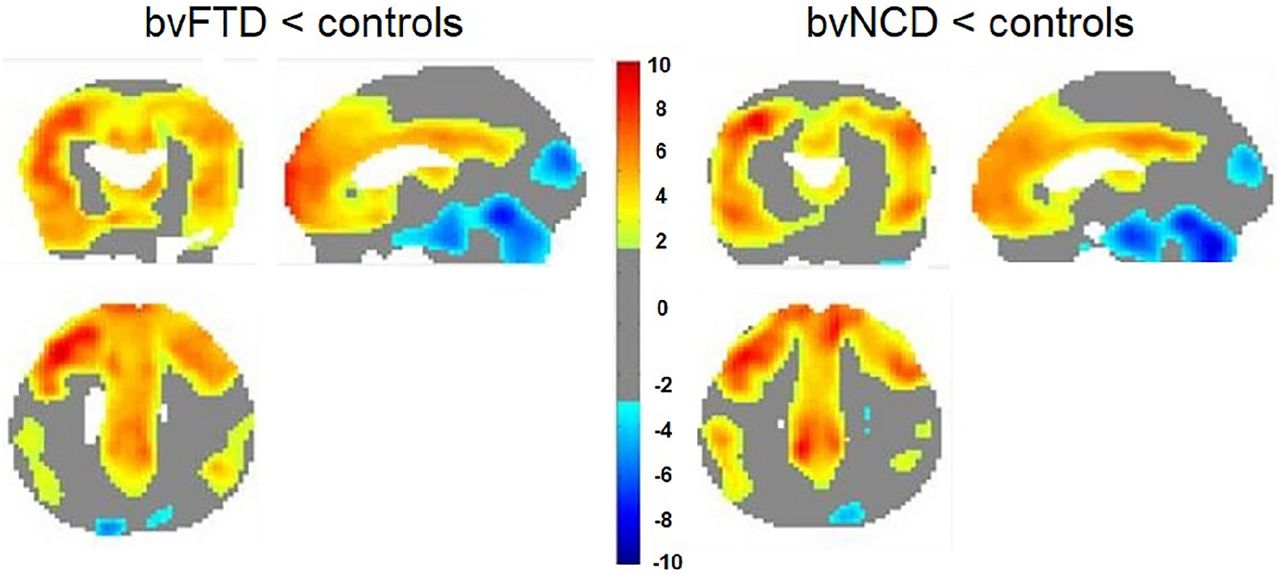
SPM12 statistical analyses contrasting 18F-FDG PET in each frontal group with healthy controls at inclusion revealed a significant reduction of frontal metabolism in both patient groups (Fig. 1; Table 2). Compared with the control group, the bvFTD group seemed to have a more extended decrease of cerebral activity bilaterally in the frontal areas than did the bvNCD group, but the direct group comparison did not reveal any significant difference. There was only a trend (P < 0.001, uncorrected for multiple comparisons) for the bvFTD patients to have a greater hypometabolism than the bvNCD patients in the dorsal anterior cingulate cortex (Montreal Neurologic Institute coordinates: x = 15, y = 41, z = 19, Z = 3.72, k = 56), a region belonging to the salience network (22), and in the inferior temporal pole (x = 33, y = 5, z = −44, k = 49). There was a trend (P < 0.001, uncorrected) for the bvNCD group to have a lower metabolism than did the bvFTD group in the left intraparietal sulcus (x = −33, y = −37, z = 46, k = 41). Adding frontal atrophy measure as a confounding covariate in the contrast did not modify the result.

SPM12 analysis of 18F-FDG PET for frontal patients overlaid on MRI template (P < 0.05, familywise-error–corrected for multiple comparisons).
18F-FDG PET SPM12 Analysis: Regions Showing Metabolic Differences Between Groups
We also confirmed that the 2 frontal groups demonstrated reduced frontal activity compared with AD (Table 2).
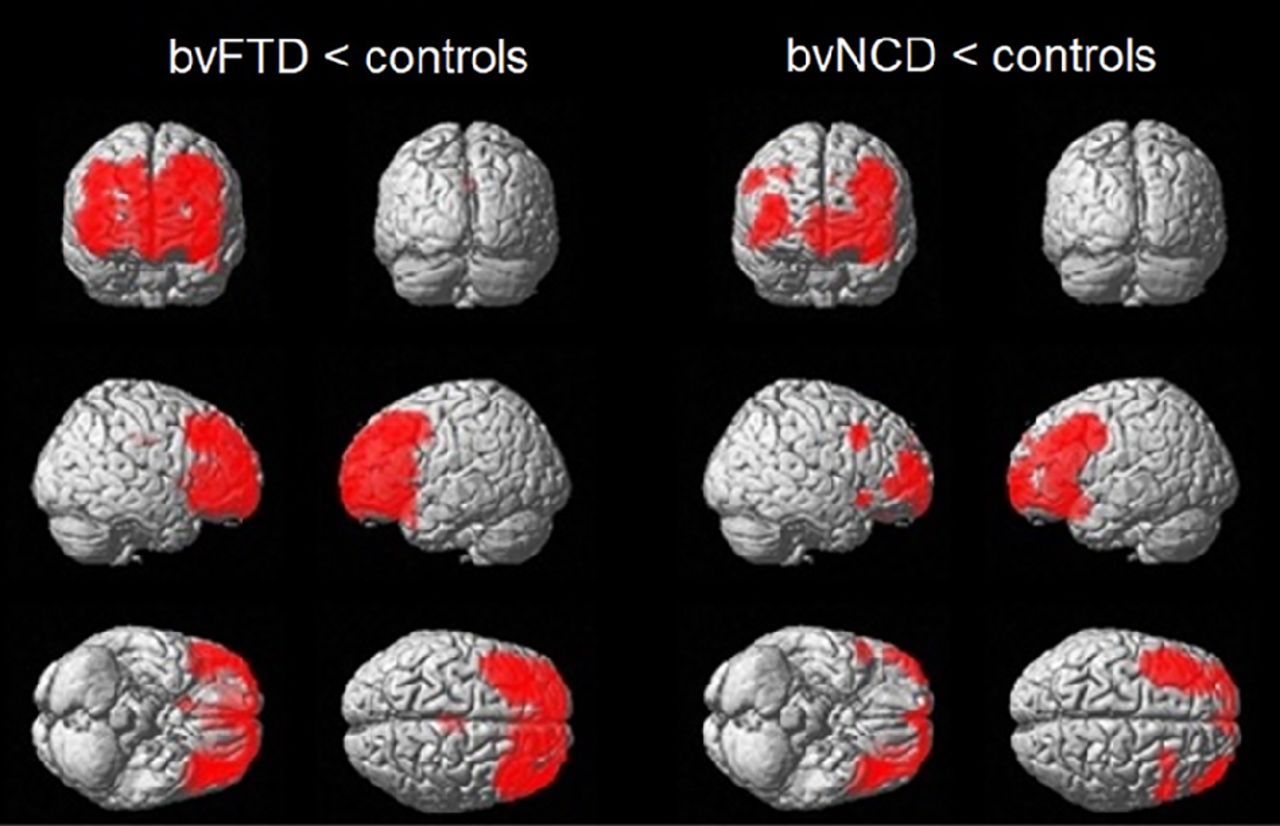
Multivariate partial least-squares analysis showed that 1 LV represented a significant group difference (P < 0.001) for both bvFTD versus controls and bvNCD versus controls. The brain metabolic involvement was similar in both groups (Fig. 2). There was no significant LV between the bvFTD and bvNCD groups, confirming the univariate results.
Multivariate partial least-squares results: topography of cerebral hypometabolism in bvFTD patients and frontal bvNCD patients when compared with controls. Color scale represents bootstrap ratio (hot colors for areas with decreased metabolism in patients compared with controls; cold color for reverse contrast).
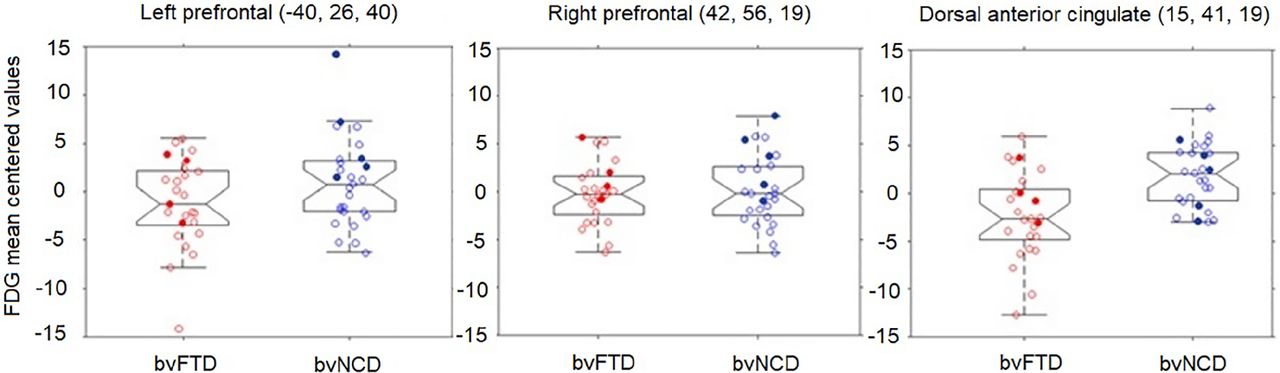
Since few patients had unexpected follow-up results, plots of 18F-FDG PET uptake for the bvFTD and bvNCD groups were generated for regions with the maximum SPM12 voxel significance in order to identify potential outliers (Fig. 3). A single patient had higher left prefrontal 18F-FDG PET uptake than did the others in the bvNCD group, and the diagnosis for this patient was a slowly progressive form of bvNCD. Of note, other patients whose follow-up diagnosis changed to an alternative diagnosis (e.g., stable, vascular, or psychiatric cases) had frontal metabolic values within the ranges of patients whose diagnosis was confirmed at follow-up.
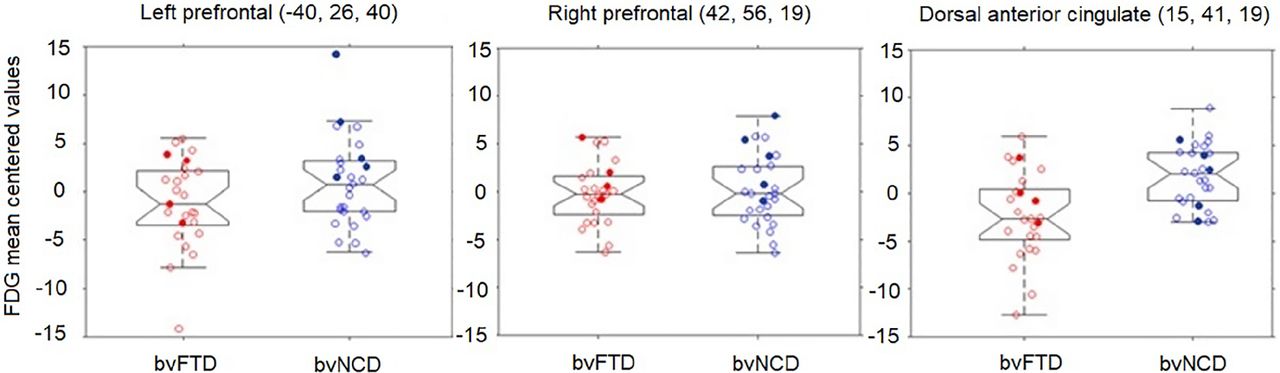
Plots of 18F-FDG PET uptake values in frontal patients. Solid circles show patients with alternative diagnosis at follow-up.
We compared participants with a diagnosis of bvFTD (n = 21 + 5) and bvNCD (n = 17) at follow-up. There was no significant difference in 18F-FDG PET distribution. We observed a trend (P < 0.001, uncorrected) for lower metabolism in the medial frontal cortex (x = 13, y = 32, z = 28, k = 12) and relatively higher metabolism in the premotor cortex (x = −24, y = −16, z = 61, k = 68, and x = 29, y = −20, z = 61, k = 18) for bvFTD compared with bvNCD.
DISCUSSION
A frontotemporal decrease in metabolism is considered an important criterion for a diagnosis of probable bvFTD (1). Accordingly, we studied a group of patients who were referred for a differential diagnosis of neurocognitive and behavioral dysexecutive disorder and had some degree of frontal atrophy on structural brain images. Patients either fulfilled the criteria for probable bvFTD or presented with bvNCD and did not fulfill the 3 required clinical diagnostic criteria (1). Statistical analysis of the 18F-FDG PET results revealed that both bvFTD and bvNCD patients presented with a pattern of frontal hypometabolism, compared with controls and AD patients. When groups of bvFTD and bvNCD patients were compared at inclusion and at follow-up, there was only a trend for lower dorsomedial prefrontal metabolism in bvFTD. bvNCD participants had more cognitive than behavioral symptoms, and all had memory impairment. Although we do not have neuropathologic or genetic confirmation, such participants may correspond to a subgroup of bvFTD patients already described by Rascovsky et al. (1).
Patients first came to the memory clinic with memory and executive complaints. At follow-up, only 2 bvNCD and 1 bvFTD patients were diagnosed with psychiatric disease or addiction. None received a diagnosis of parkinsonism, but 1 bvNCD patient had vascular dementia, which corresponded to an alternative diagnosis (23). A differential diagnosis for the bvNCD patients would have been AD, as the proportion of patients with FTD syndrome and AD neuropathology is not negligible (24). However, our bvNCD patients did not have a typical AD-related hypometabolic pattern in the posterior associative cortices. Effectively, the dysexecutive variant of AD was reported to be characterized by greater temporoparietal atrophy than frontal atrophy (25), even if medial and orbital frontal hypometabolism was greater in frontal cases than in more typical AD cases (26). Early cognitive disorder has already been reported in bvFTD (27–29). Our patients with bvNCD were older than the bvFTD patients, and they were slightly less demented, according to the clinical dementia rating scale. This finding might be consistent with the fact that early-onset FTD is more affected than late-onset FTD (30). Mild frontal, insular, or temporal atrophy was recently reported in a few patients with bvFTD phenocopy (31), but frontal hypometabolism in our stable bvNCD cases is not consistent with this diagnosis. Of note, some patients with C9ORF72 mutations can present with a slow-progression phenotype of bvFTD (32). Only a few participants in our sample had genetic testing, and the results were negative for the main FTD mutations. More interestingly, in the report of Rascovsky et al. (1), patients with frontotemporal lobar degeneration neuropathology who did not meet bvFTD criteria were older and presented with memory impairment, as in our bvNCD group. The main limitation of our study is that there was no biomarker of AD amyloid or tau pathology in our sample and no pathologic diagnosis.
The main finding of the current clinical study was that frontal hypometabolism was as important in bvNCD as in bvFTD. More precisely, there was no significant metabolic difference between the groups, using univariate and multivariate analyses or displaying plots of 18F-FDG PET frontal uptake. Even if that was our expectation, based on the literature, there was only a trend for a greater dorsomedial prefrontal glucose hypometabolism in the bvFTD group. This finding might indicate that bvNCD is an early stage of frontotemporal lobar degeneration with mild dysexecutive syndrome at onset. The last limitation of our study is that a longer follow-up (with postmortem brain analyses) would be required to better characterize patients with bvNCD.
CONCLUSION
Frontal hypometabolism was observed in a dysexecutive presentation of frontal neurodegenerative disorder (bvNCD) that did not fulfill all clinical criteria for bvFTD.
DISCLOSURE
Financial support was received from the University of Liege (R.CFRA.2395), the FRS-FNRS (grant T.0193–16), and the Belgian InterUniversity Attraction Pole (IUAP 7/11). Christine Bastin is a research associate at FRS-FNRS. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Do brain metabolic pattern and clinical evolution characterize patients with bvNCD who do not fulfill 3 bvFTD criteria?
PERTINENT FINDINGS: In this cohort study, we could not demonstrate a significant difference in 18F-FDG-PET distribution between bvNCD and bvFTD patients. bvNCD patients were slightly older, and all complained of memory impairment.
IMPLICATIONS FOR PATIENT CARE: Frontal hypometabolism may characterize a subgroup of bvFTD patients with memory impairment but not all bvFTD criteria.
ACKNOWLEDGMENTS
We thank all the participants and their relatives.
Footnotes
Published online March 31, 2021.
- © 2021 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 17, 2020.
- Revision received March 18, 2021.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.