


Abstract
1395
Objectives: The evaluability of 18F-FDG PET/CT studies for treatment response to cancer therapy is dependent on a multitude of factors that affect its quantitative measurement, the Standard Uptake Value (SUV). In efforts to provide standards and guidelines to reduce variability of PET imaging, the QIBA FDG-PET Biomarker Committee, as part of the Quantitative Imaging Biomarkers Alliance (QIBA)) has developed an imaging profile for acceptable guidelines to acquire quantitative PET/CT imaging. Our objective is to provide real-world key parameter data from a multitude of 18F-FDG imaging studies and to compare how well these parameters match the QIBA profile.
Methods: 338 18F-FDG PET/CT studies were compiled across 4 NCI NCTN multi-center clinical trials utilizing PET/CT as the primary imaging modality for treatment monitoring. Utilizing DICOM tag metadata and adjunctive data form information, the 18F-FDG uptake times (in minutes), the consistency of these times from follow-up to baseline exams, glucose measurements (in mg/dL), fasting times (in hours), and radiopharmaceutical dose (in MBq), were analyzed and compared to the acceptable parameters as outlined in the “FDG-PETCT as an Imaging Biomarker Measuring Response to Cancer Therapy” QIBA profile (version 1.13).
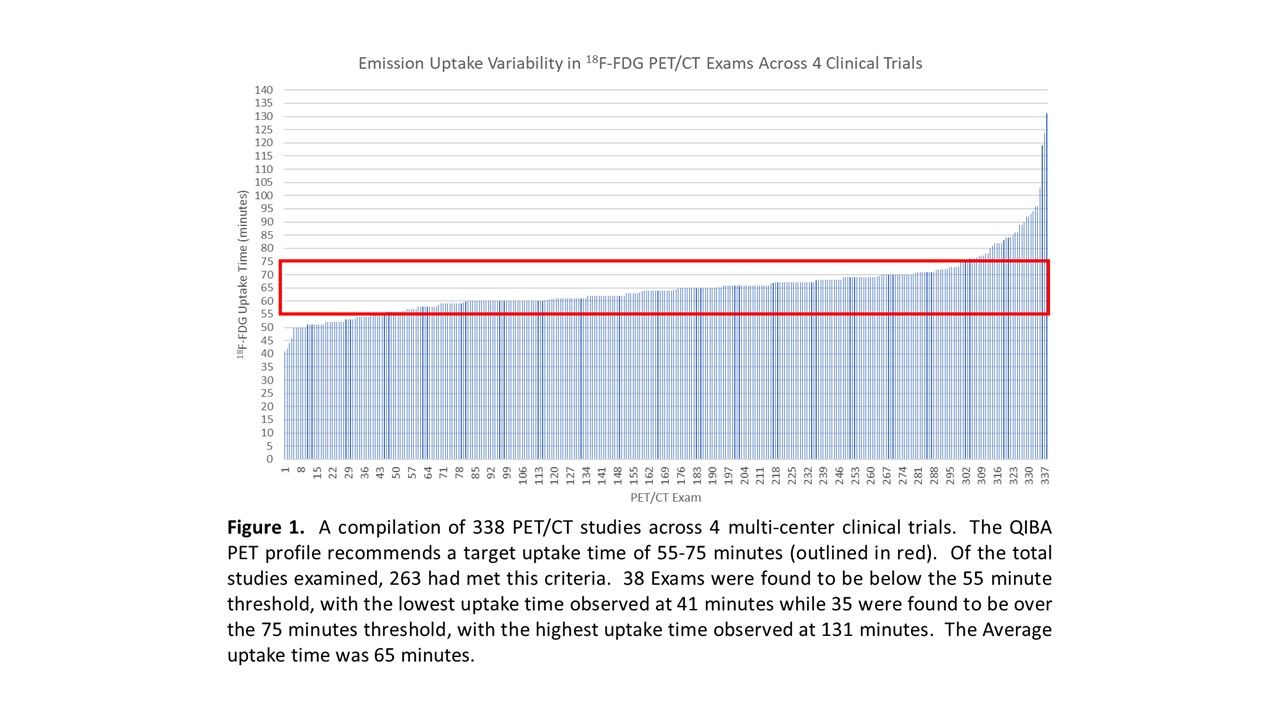
Results: The emission uptake times fell in line with the QIBA profile acceptable ranges at a rate of 78% out of 338 observed exams, with an average uptake time of 65 minutes. The percentage of QIBA compliant uptake time consistency was 77% out of an evaluable sample of 197 exams; with an average consistency of 8 minutes (absolute value). 18F-FDG dosing was found to be QIBA compliant in of 99% out of 338 observed exams; none of the exams evaluated had an 18F-FDG dose below the acceptable QIBA range of 185 to 740 MBq. Fasting was found to be QIBA compliant in 88% out of an evaluable sample of 294 exams (based on available fasting information), with 36 studies found below the acceptable QIBA parameter of 6 hours. For glucose, while the QIBA recommendation was to measure blood glucose levels prior to imaging and report abnormalities, 99% of glucose measurements from 314 studies with this information available were found to be within the diabetic cut-off of 200mg/dL. Conclusion: While there are several parameters involved in 18F-FDG PET imaging studies, key parameters of radiopharmaceutical uptake, uptake consistency, radiopharmaceutical dose, fasting, and blood glucose measurements demonstrates a variable, though reasonably high rate of compliancy with the QIBA guidelines; with the minimum rate at 77%. However, since the protocols from which these data were compiled had built-in PET/CT acquisition guidelines, as opposed to standard of care, it is possible that these percentages may be lower in trials that only require standard-of-care imaging for PET/CT, and can be made higher with consistent quality-control feedback. Research Support: ODSA TECH 13-060 (IPP), NCI 5U24CA180803 (IROC)

In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.