


Abstract
13
Introduction: Effect of dual-input function and dispersion on lung FDG-PET kinetic quantification using the EXPLORER total-body PET/CT scanner
Objectives: Dynamic 18F-FDG PET with tracer kinetic modeling has been found promising for detection and characterization of lung diseases including lung cancer and pulmonary fibrosis. Existing kinetic modeling approaches commonly use a single-blood input function, e.g., from the right ventricle. However, the lungs are supplied by both the right ventricle (RV) via the pulmonary arteries and the left ventricle (LV) via the bronchial arteries. The effect of dual-blood supply and associated time delay and dispersion has been rarely investigated, in part due to the insufficient temporal resolution of conventional dynamic PET imaging and due to the previous attention focusing on quantification of the steady-state kinetics such as the glucose metabolic rate. In this work, we demonstrate the effect of these factors on quantification of fast kinetics using high-temporal resolution dynamic imaging on the total-body EXPLORER PET/CT scanner.
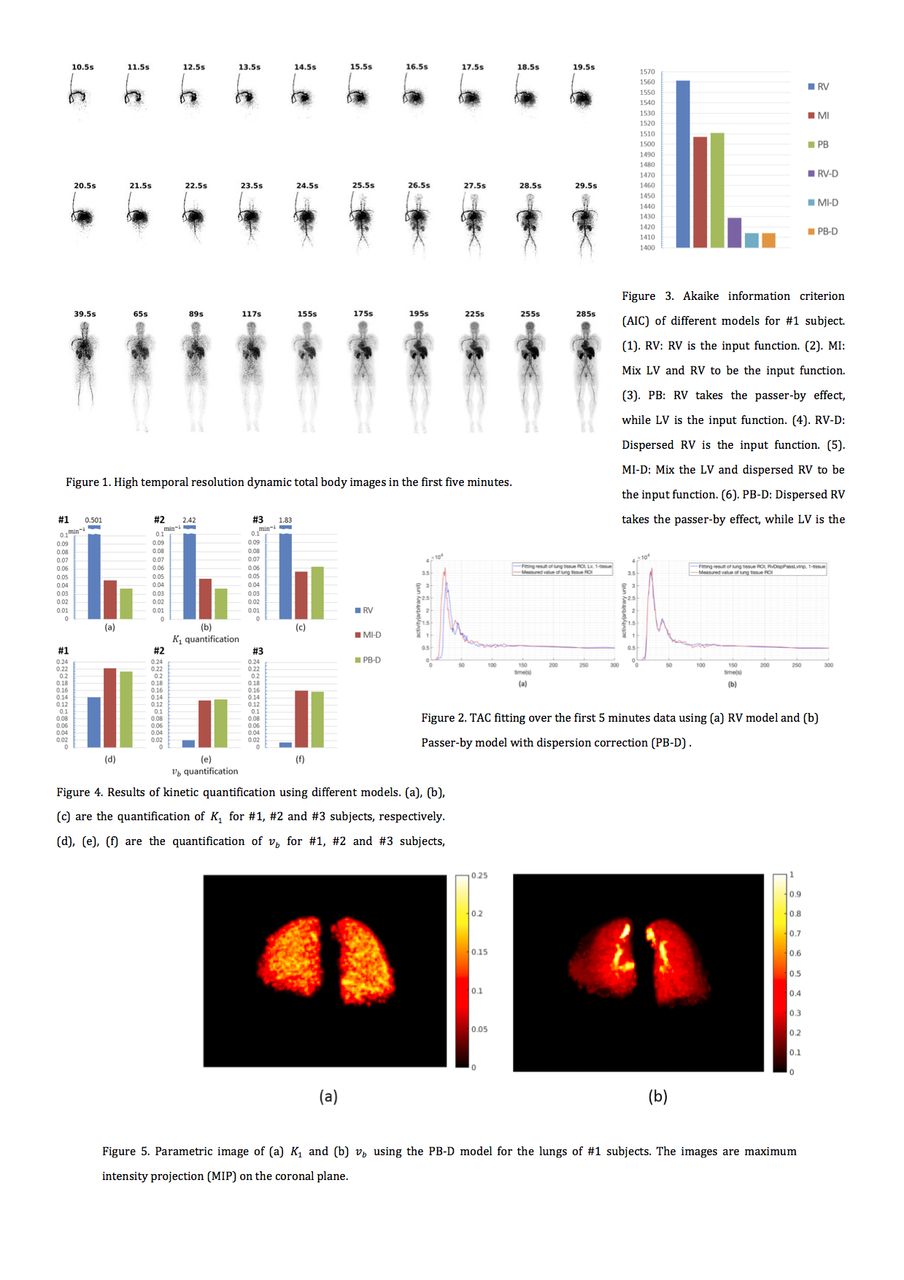
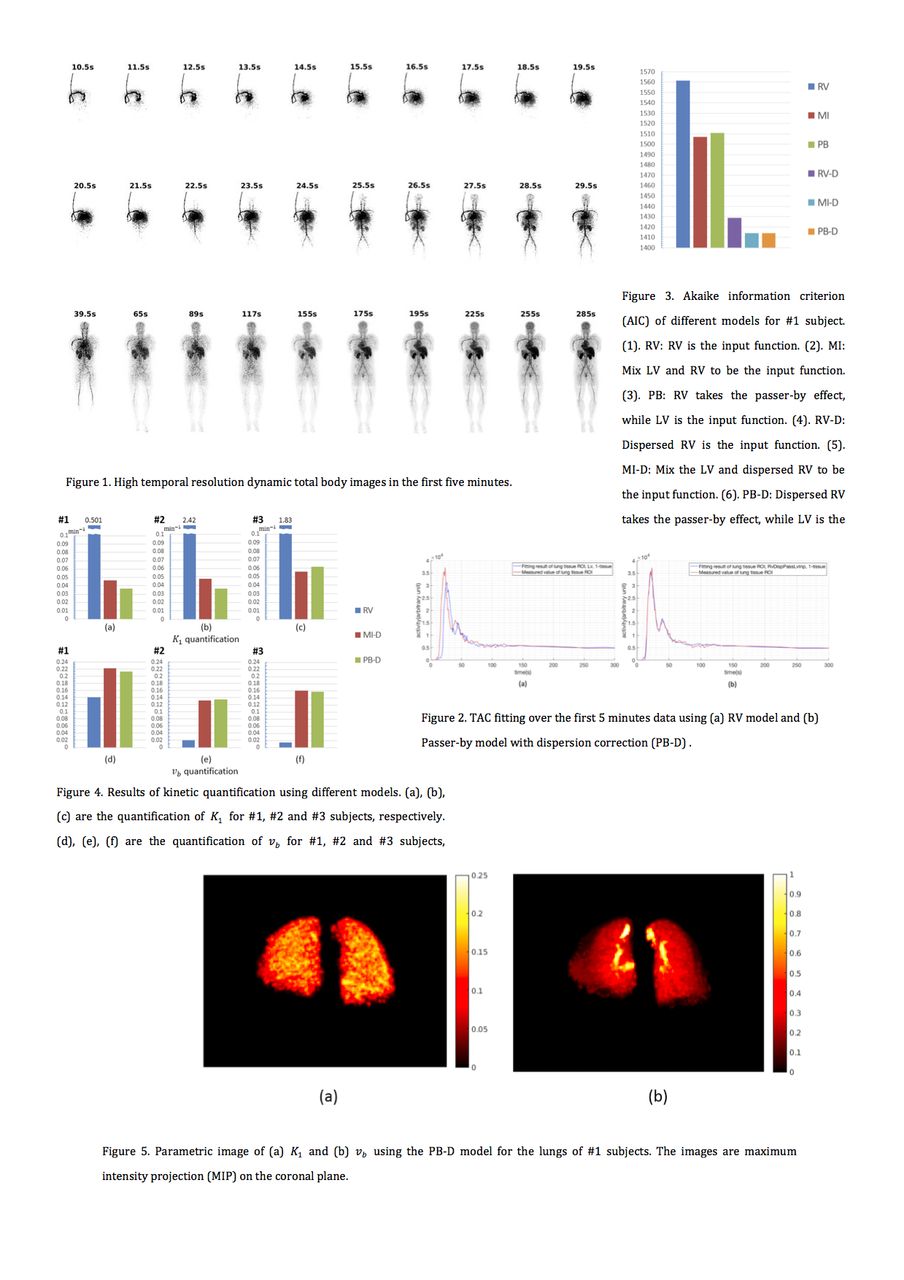
Methods: Three healthy subjects were injected with 9.5-10.6 mCi of 18F-FDG and scanned on the uEXPLORER total-body PET/CT scanner. The list-mode data for the first five minutes post injection were reconstructed into 100 high-temporal resolution (HTR) dynamic frames: 60x1s, 30x2s, 6x10s, 4x30s. Time activity curves (TACs) were extracted from regions of interest (ROI) placed in the left ventricle (LV), right ventricle (RV) and a total of five different lobes in the left and right lungs. The TACs were fitted using the one-tissue compartment model. We compared three different models of the blood input function: (1) the popular RV input function Cp(t) = CRV(t), (2) the mixed-input (MI) model Cp(t) = fCLV(t)+(1-f)CRV(t) that includes both LV and RV as the inputs with f denoting the fraction of contribution from the LV, (3) the passer-by (PB) model that uses the LV as the input but uses RV as a passer-by. The three models (RV, MI, PB) were used with and without dispersion correction, resulting in a total of six different input models (RV, MI, PB, RV-D, MI-D, PB-D) in our comparison. In all the models, the time delay of the input function and fractional blood volume were included for joint estimation. The statistical fit quality of different models for fitting lung tissue TACs was compared using the Akaike information criterion (AIC). The impact on quantification of fractional blood volume (vb) and FDG delivery rate (K1) was evaluated. We also generated parametric images of K1 and vb over the lung region of subject #1.
Results: High-temporal resolution dynamic images were successfully obtained (Figure 1). As compared to the standard RV model, the input models taking into account the dual-blood supply and dispersion effects greatly improve the TAC fitting, as shown in Figure 2. Among different models, either dual-blood supply (MI vs RV, PB vs RV) or dispersion correction (RV-D vs RV) improved TAC fitting according to the AIC evaluation (Figure 3). When both dual-blood supply and dispersion were combined into one model (MI-D and PB-D), the AIC value was further improved. The improved TAC fitting led to a dramatic impact on quantification of K1 and vb (Figure 4). The quantification results using the dual-input and dispersion correction also appeared more stable across the three healthy subjects than the RV input model. Parametric images of K1 and vb using the PB-D model is consistent with the ROI-based study and further demonstrates voxel-based spatial distribution (Figure 5).
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.