


Abstract
We aimed to evaluate the diagnostic performance of 18F-FDG PET/CT for the detection of posttransplantation lymphoproliferative disorder (PTLD) in a pediatric population and explore its feasibility during response assessment. Methods: This retrospective study included 28 pediatric transplant recipients who underwent a total of 32 18F-FDG PET/CT scans due to clinical suspicion of PTLD within an 8-y period. Pathology reports and 2 y of follow-up were used as the reference standard. Twenty-one response assessment 18F-FDG PET/CT scans were reevaluated according to the Lugano criteria. Results: The diagnosis of PTLD was established in 14 patients (49%). Sensitivity, specificity, positive predictive value, and negative predictive value of 18F-FDG PET/CT for the detection of PTLD in children with a clinical suspicion of this disease were 50% (7/14), 100% (18/18), 100% (7/7), and 72% (18/25), respectively. False-negative results occurred in patients with PTLD in the Waldeyer’s ring, cervical lymph nodes, or small bowel with either nondestructive or polymorphic PTLD. Two of 5 interim 18F-FDG PET/CT scans and 3 of 9 end-of-treatment 18F-FDG PET/CT scans were false-positive. Conclusion: 18F-FDG PET/CT had good specificity and positive predictive value but low to moderate sensitivity and negative predictive value for the detection of PTLD in a 28-pediatric-patient cohort with a clinical suspicion of this disease. False-negative results were confirmed in the Waldeyer’s ring, cervical lymph nodes, and small bowel with either nondestructive or polymorphic PTLD subtypes. 18F-FDG PET/CT appears to have a limited role in the response assessment setting of pediatric PTLD, given the observed high proportions of false-positives both at interim and at end-of-treatment evaluations.
- posttransplant lymphoproliferative disorder
- 18F-fluoro-d-deoxyglucose PET
- 18F-FDG PET/CT
- diagnosis
- pediatric
Posttransplantation lymphoproliferative disorder (PTLD) is a major complication of continued immunosuppressive therapy after solid-organ or hematopoietic stem cell transplantation. Morphologically, PTLD ranges from Epstein-Barr virus–driven polyclonal lesions to aggressive monoclonal lymphoid proliferations, classified by the World Health Organization as nondestructive, polymorphic, monomorphic, or classic Hodgkin lymphoma PTLD (1).
Compared with adults, pediatric PTLD patients have distinct characteristics regarding incidence and presentation. PTLD is the most common posttransplant malignancy in children, with a higher reported incidence than in adults (2–4). An important risk factor associated with PTLD development is an Epstein-Barr virus status mismatch between seropositive donors and seronegative recipients. The Epstein-Barr virus has a recognized role in the pathogenesis and development of PTLD, particularly related to nondestructive and polymorphic lesions. Because only 20%–25% of the pediatric population is an Epstein-Barr virus carrier by the age of 5 y (unlike 80%–90% in the adult population), children are at an increased risk of developing this disorder after transplantation (5,6). The presentation may be asymptomatic or have a variation of symptoms, including B symptoms, lymphadenopathy, or graft dysfunction. Although it may be localized in any organ system, pediatric PTLD has been reported to occur more frequently in the Waldeyer’s ring and gastrointestinal tract (7,8). This location is in contrast to that in the adult PTLD population, for whom lesions have been reported to occur proportionally more often in the transplant allograft and lymph nodes (6,9).
Timely diagnosis of PTLD remains challenging but is crucial for treatment initiation, management, and prognostication. Because reduction of immunosuppression is the first-line intervention in many PTLD cases, prompt therapy, particularly in nondestructive lesions, may be adequate to achieve remission. Nevertheless, this therapy may also jeopardize the transplanted organ (10–12). Biopsy remains necessary for diagnostic confirmation, but imaging may be used to confirm or refute clinical suspicion of PTLD and identify suggestive lesions accessible for biopsy. For treatment evaluation, imaging-based response assessment may be used to monitor lesions in the entire body, circumventing the need for invasive biopsies and their associated complications. 18F-FDG PET/CT combines metabolic and anatomic information and may be of value in the diagnosis and treatment evaluation of pediatric PTLD. Preliminary literature suggests that 18F-FDG PET/CT may be helpful in detecting occult lesions and clarifying findings on other imaging modalities (13–19). However, as these previous studies suffered from small sample sizes and frequently mixed pediatric and adult populations, the value of 18F-FDG PET/CT in pediatric PTLD remains unclear. If 18F-FDG PET/CT proves accurate in detecting PTLD and feasible for treatment evaluation, it may be implemented in future guidelines. In this study, we aimed to determine the diagnostic performance of 18F-FDG PET/CT for the detection of PTLD in the pediatric population and to explore its feasibility in the therapy response assessment setting.
MATERIALS AND METHODS
Study Design and Patients
This retrospective single-center study was conducted at the University Medical Center Groningen. All consecutive patients 18 y old or younger for whom a 18F-FDG PET/CT scan was requested on clinical suspicion of PTLD between January 2010 until January 2019 were included. The first 18F-FDG PET/CT scan and in some children a second or third 18F-FDG PET/CT scan (provided the 18F-FDG PET/CT scan was requested because of a clinical suspicion of PTLD and there was a minimum interval of 2 y without any evidence of PTLD between these scans) were included for the diagnostic performance analysis. In patients with pathologically proven PTLD, all 18F-FDG PET/CT scans for treatment evaluation were analyzed to explore the feasibility of 18F-FDG PET/CT in the response assessment setting. Demographic, relevant clinical data and PTLD morphology or histology were retrieved from the electronic patient charts. Patients who had a complete tumor resection before 18F-FDG PET/CT, and patients for whom the established reference standard criteria were not fulfilled, were excluded. A waiver was obtained from the local medical ethics committee on September 7, 2017 (study 201700855).
18F-FDG PET/CT Acquisition
All 18F-FDG PET/CT scans were performed on a Biograph 40- or 64-slice mCT (Siemens Healthineers) according to the guidelines for 18F-FDG PET and PET/CT imaging in pediatric oncology from the European Association of Nuclear Medicine (20). The imaging protocol included a minimum fasting time of 6 h. The 18F-FDG dose was adjusted according to body weight following European Association of Nuclear Medicine guidelines, and 18F-FDG PET/CT scans were performed from the mid thigh to the skull base, 60 min after intravenous administration. 18F-FDG PET/CT images were corrected for scatter and attenuation on the basis of low-dose CT information.
18F-FDG PET/CT for PTLD Detection
18F-FDG PET/CT scans performed for PTLD detection were retrospectively reviewed by 3 readers (2 experienced nuclear medicine physicians and 1 research fellow) using syngo.via software (Siemens Healthineers). The readers reviewed the scans independently from each other and were masked to other imaging findings, pathology results, and clinical findings. Any metabolic active focus that could not be related to physiologic distribution, or any focus with an 18F-FDG uptake higher than the surrounding tissues and not suggestive of other pathology, was regarded as PTLD-positive. If a metabolic active focus was visualized but could not with certainty be attributed to PTLD or other diseases (such as infectious, inflammatory, or other malignant lesions), the 18F-FDG PET/CT scan result was considered ambiguous. A differential diagnosis was noted when deemed relevant by the reader. Discordant results between readers were reevaluated in a consensus meeting and conclusively classified as PTLD-positive or PTLD-negative. False-positive and false-negative scans were reevaluated to determine potential patterns. Histopathologic examinations were used as a reference standard for PTLD diagnosis. Two experienced hematopathologists were consulted to clarify morphology for 12 patients whose original pathology report was not sufficiently clear. In the case of a PTLD-negative biopsy or lack of tissue for pathologic examination, a 2-y follow-up period without preemptive PTLD therapy was accepted as the reference standard. In adults, absence of lymphoma during this period has been shown to be an accurate marker for lack of disease in other lymphomas (21,22). True-positive scans were those interpreted as PTLD-positive on 18F-FDG PET/CT and confirmed by histopathologic examination to be PTLD within 2 y. True-negative scans were those interpreted as PTLD-negative on 18F-FDG PET/CT and with no signs of PTLD being identified within a 2-y follow-up. False-positive scans were those interpreted as PTLD-positive on 18F-FDG PET/CT and with no signs of PTLD being identified within a 2-y follow-up. False-negative scans were those interpreted as PTLD-negative on 18F-FDG PET/CT but confirmed by histopathologic examination to be PTLD within 2 y.
18F-FDG PET/CT for Response Assessment
All 18F-FDG PET/CT scans performed for response assessment were reevaluated according to the Lugano criteria with masking to other imaging findings, pathology results, and clinical findings (23). Scans with a score of 1–3 were considered indicative of complete remission, whereas scores of 4–5 were considered to represent partial response, stable disease, or progressive disease. 18F-FDG PET/CT response assessment scans for which a reference standard was available were classified as true-positive, true-negative, false-positive, or false-negative for the presence of PTLD. For interim scans, histopathologic examination was accepted as the reference standard for PTLD confirmation. For end-of-treatment scans, the accepted reference standard for PTLD confirmation was a confirmatory biopsy or high suspicion of death due to PTLD, whereas a negative 2-y follow-up period was accepted as confirmation of absence of disease.
Statistical Analysis
Baseline patient characteristics were summarized using median ± SD with interquartile range. The sensitivity, specificity, positive predictive value, and negative predictive value of 18F-FDG PET/CT for the detection of PTLD on a patient-based analysis were calculated, along with the 95% confidence interval. Interobserver variability among the 3 observers was calculated using the Fleiss κ. The κ-value was interpreted according to the method of Landis and Koch: poor (0–0.20), fair (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80), and perfect agreement (0.81–1) (24). Because of the relatively small and heterogeneous population, and the inconsistent availability of a reference standard, the diagnostic yield of 18F-FDG PET/CT in the response assessment setting for PTLD was only descriptively analyzed. Statistical analyses were performed using SPSS, version 23.0 (IBM Corp.).
RESULTS
Patients
Thirty-three potentially eligible patients were identified. Four patients were excluded because they did not fulfill the reference standard criteria (3 patients did not have a 2-y follow-up and 1 patient received preemptive treatment with rituximab after a negative biopsy). One patient was excluded because the suspected tumor had been fully resected before 18F-FDG PET/CT. Because of PTLD suspicion on multiple occasions with an interval of more than 2 y between different 18F-FDG PET/CT scans, 2 patients had 2 eligible scans and 1 patient had 3 eligible scans. Thus, in total, 32 18F-FDG PET/CT scans in 28 patients were included. Common indications for requesting an 18F-FDG PET/CT scan are described in Table 1. There were 13 (46%) boys and 15 (54%) girls (Table 2). Patient age ranged from 1 to 18 y, with a median age of 4 y. Liver was the most frequently transplanted organ (n = 20, 71.4%), followed by lung (n = 3, 10.7%), multiple organs (n = 2, 7.1%), heart (n = 1, 3.6%), kidney (n = 1, 3.6%), and small bowel (n = 1, 3.6%). According to the reference standard, 14 patients (50%) were diagnosed with PTLD, of which 5 cases (35.7%) were nondestructive, 3 (21.5%) polymorphic, 5 (35.7%) monomorphic, and 1 (7.1%) classic Hodgkin lymphoma.
Indications for 18F-FDG PET/CT
Patient Characteristics (n = 28)
Diagnostic Performance of 18F-FDG PET/CT for PTLD Detection
After a consensus meeting by the 3 readers, 7 scans were considered as PTLD-positive and 25 as PTLD-negative. A PTLD-positive biopsy, a PTLD-negative biopsy with 2 y of follow-up without preemptive therapy, and a 2-y follow-up without preemptive therapy or biopsy were used as the reference standard for 14 (43.8%), 10 (31.2%), and 8 (25%) of the 18F-FDG PET/CT scans, respectively. According to the reference standard, 18 (56.2%) 18F-FDG PET/CT scans were true-negative, 7 (21.9%) true-positive, 0 false-positive, and 7 (21.9%) false-negative (Table 3). On a patient-based analysis, the sensitivity of 18F-FDG PET/CT for the detection of PTLD was 50%, specificity was 100%, positive predictive value was 100%, and negative predictive value was 72% (Table 4).
Classification of 18F-FDG PET/CT Scans (n = 32)
Diagnostic Performance of 18F-FDG PET/CT in PTLD Detection
Causes of False-Negative 18F-FDG PET/CT Scans for PTLD Detection
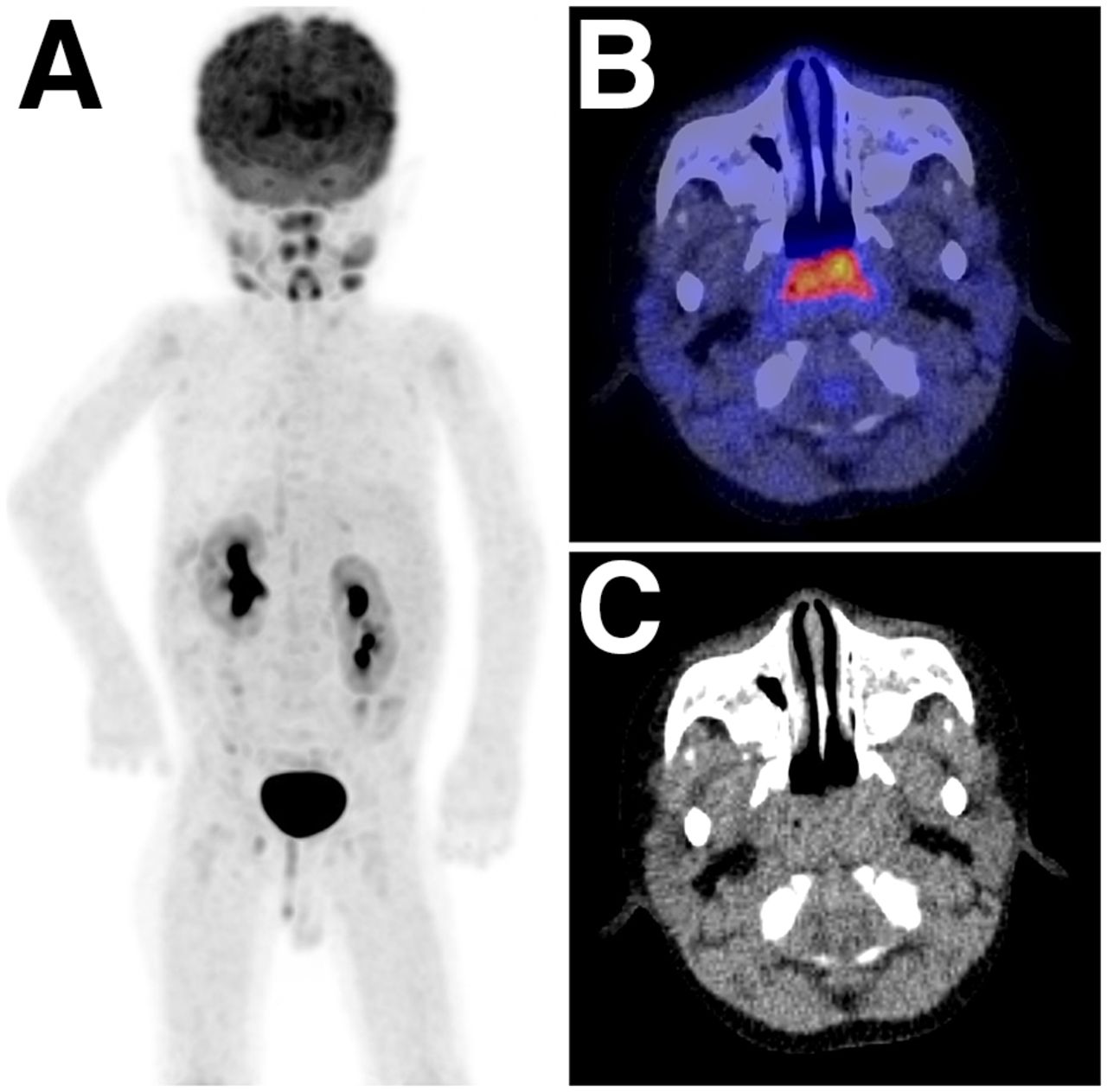
Seven of 32 (21.9%) 18F-FDG PET/CT scans performed because of clinical suspicion of PTLD were false-negative (Table 5). Five of the 7 false-negative cases had biopsy-confirmed nondestructive PTLD. On 18F-FDG PET/CT, 3 patients had symmetric 18F-FDG uptake (higher than liver 18F-FDG uptake) in and limited to the Waldeyer’s ring, whereas 2 had symmetric 18F-FDG uptake (higher than liver 18F-FDG uptake) in the Waldeyer’s ring along with 18F-FDG–avid (higher than liver 18F-FDG uptake) cervical lymph nodes (Fig. 1). The remaining 2 false-negative patients had biopsy-confirmed polymorphic PTLD in the small intestines, which was interpreted as physiologic intestinal 18F-FDG uptake in both cases. In these 2 patients, no focal 18F-FDG–avid lesions were observed; rather, diffuse 18F-FDG uptake (higher than liver 18F-FDG uptake) was observed in the gastrointestinal tract. One patient initially had a false-negative scan with polymorphic PTLD in the ileum. After adjustment of immunosuppression and watchful waiting, the patient developed a monomorphic PTLD, which was visualized by subsequent 18F-FDG PET/CT (Fig. 2). Abdominal diagnostic CT was performed in 1 of these 2 patients, but the clinical radiology report mentioned no signs of PTLD.
Description of False-Negative 18F-FDG PET/CT Scans (n = 7)
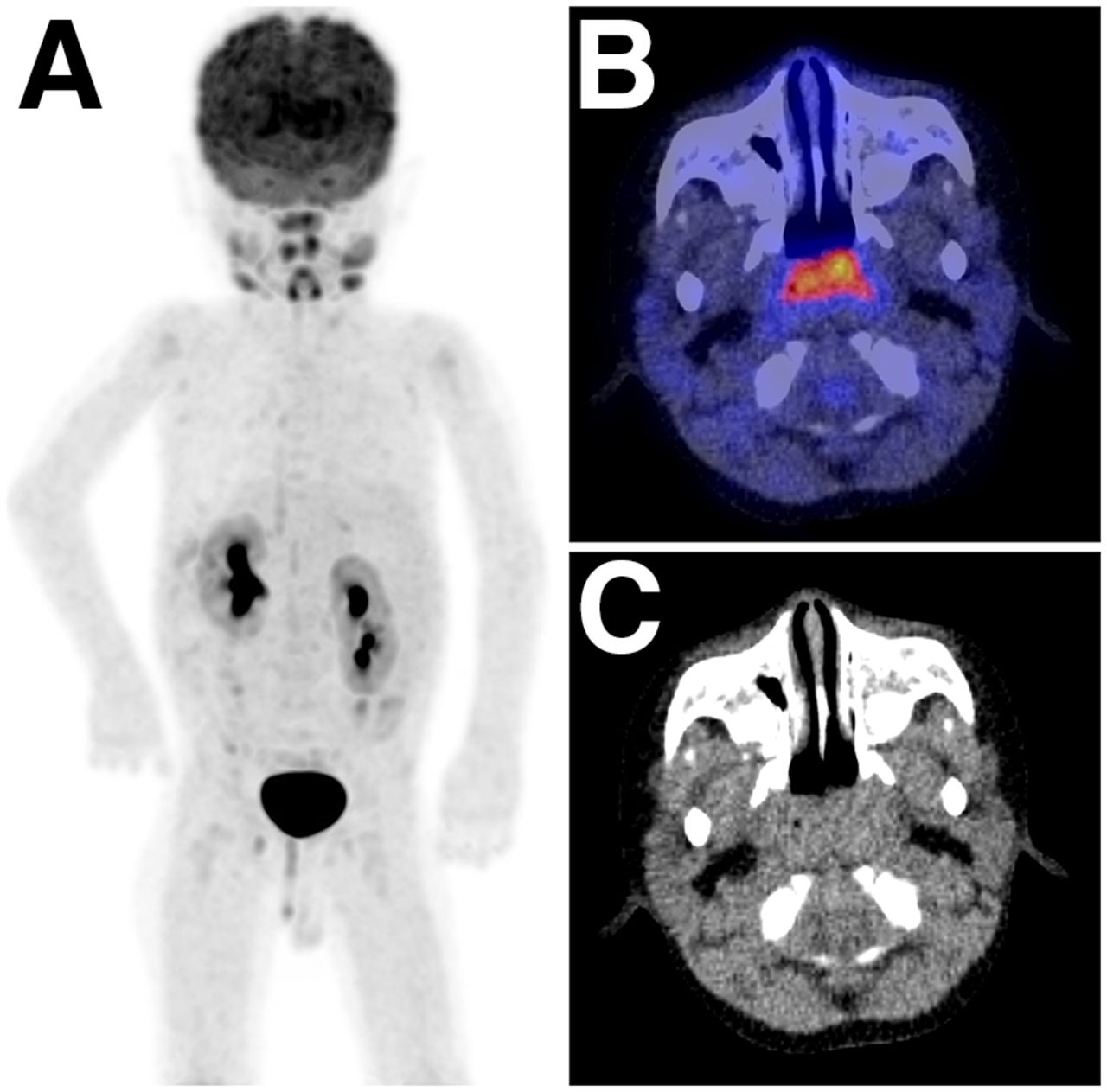
Two-year-old boy 1 y after receiving liver transplant because of biliary atresia. 18F-FDG PET/CT was requested after prolonged fever. False-negative 18F-FDG PET/CT scan with biopsy confirmed nondestructive PTLD in adenoid or tonsils. (A) Maximum-intensity-projection 18F-FDG PET shows almost symmetric uptake in Waldeyer’s ring and salivary glands. (B) Axial fused 18F-FDG PET/CT shows almost symmetric uptake in adenoids. This pattern of 18F-FDG uptake was interpreted as physiologic. (C) Low-dose CT does not show any suggestive lesions.
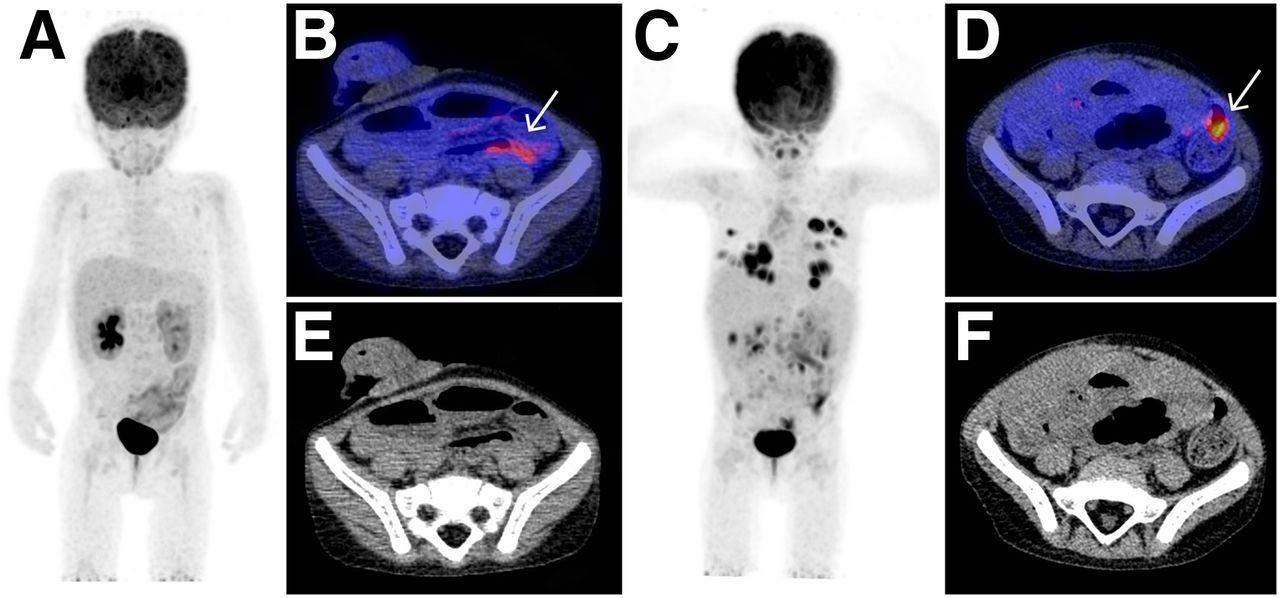
Three-year-old girl 2 mo after small-bowel transplantation because of unexplained absorption disorder. 18F-FDG PET/CT was requested during clinical admission due to fever and leukopenia. (A, B, and E) False-negative 18F-FDG PET/CT scan with biopsy-confirmed polymorphic PTLD in ileum. Maximum-intensity-projection 18F-FDG PET (A) and axial fused 18F-FDG PET/CT (B) show diffuse uptake in small bowel (white arrow), interpreted as physiologic uptake; on low-dose CT (E), distended gas-filled bowels and postoperative ileostomy are shown. (C, D, and F) Same patient 6 mo after reduction in immunosuppression and watchful waiting: true-positive 18F-FDG PET/CT scan with biopsy-confirmed monomorphic intestinal PTLD. Maximum-intensity-projection 18F-FDG PET (C) shows multiple intrapulmonary, mesenteric, and intestinal 18F-FDG–active lesions; axial fused 18F-FDG PET/CT (D) shows focal 18F-FDG uptake in small bowel suggestive of PTLD without evident abnormalities on low-dose CT (F).
Interobserver Variability of 18F-FDG PET/CT for PTLD Detection
From a total of 32 18F-FDG PET/CT scans evaluated before the consensus meeting, discordant results were reported for 5. One 18F-FDG PET/CT scan with symmetric 18F-FDG uptake in the Waldeyer’s ring and cervical lymph nodes was considered ambiguous for PTLD by 2 readers, who thought the findings could be interpreted as either reactive lymph nodes or PTLD. One case of 18F-FDG uptake in the Waldeyer’s ring and retroperitoneal lymph nodes was considered to be due to either inflammatory changes or PTLD by 2 readers. In 1 scan with focal 18F-FDG uptake in the lung, 2 of 3 readers reported difficulties in distinguishing between PTLD and an infectious cause (i.e., fungal). Finally, in 1 scan with localized 18F-FDG uptake in the cecum and in another scan with 18F-FDG uptake throughout the whole duodenum and colon, the readers reported difficulty in differentiating whether the 18F-FDG uptake was physiologic, due to PTLD, or due to other intestinal disease such as colitis. Of the 5 discordant 18F-FDG PET/CT scans, 2 were true-positive, 2 true-negative, and 1 false-negative. The remaining 6 false-negatives scans were reported as PTLD-negative by all readers. The interobserver variability was found to be good, at a κ-value of 0.74 (95% confidence interval, 0.58–0.86).
18F-FDG PET/CT for Response Assessment
In all 14 patients who were diagnosed with PTLD, reduction of immunosuppression was the cornerstone therapy. First-line treatment was performed with rituximab in 8 patients; rituximab, cyclophosphamide, vincristine, and prednisone in 2 patients; watchful waiting in 2 patients; rituximab, vincristine, etoposide, prednisone, and doxorubicin in 1 patient; and tumor resection in 1 patient. Two patients were lost to follow-up after diagnosis. 18F-FDG PET/CT was used for interim response assessment in 6 patients on 12 occasions; of these, biopsy correlation was possible for 5 scans. According to the pathology results, there were 3 true-positive and 2 false-positive interim 18F-FDG PET/CT scans. False-positive scan results were due to therapy-induced reactive changes (Fig. 3). End-of-treatment 18F-FDG PET/CT was used in 8 patients on 9 occasions, and a reference standard was available on all occasions. There were 1 true-positive, 4 true-negative, 3 false-positive, and 1 false-negative end-of-treatment 18F-FDG PET/CT scans. In 2 false-positive cases, a negative 2-y follow-up period did not reveal any PTLD, and in 1 case, biopsy revealed follicular hyperplasia without evidence of PTLD. For the false-negative end-of-treatment 18F-FDG PET/CT, a biopsy obtained 2 mo after a PTLD-negative scan revealed monomorphic PTLD.

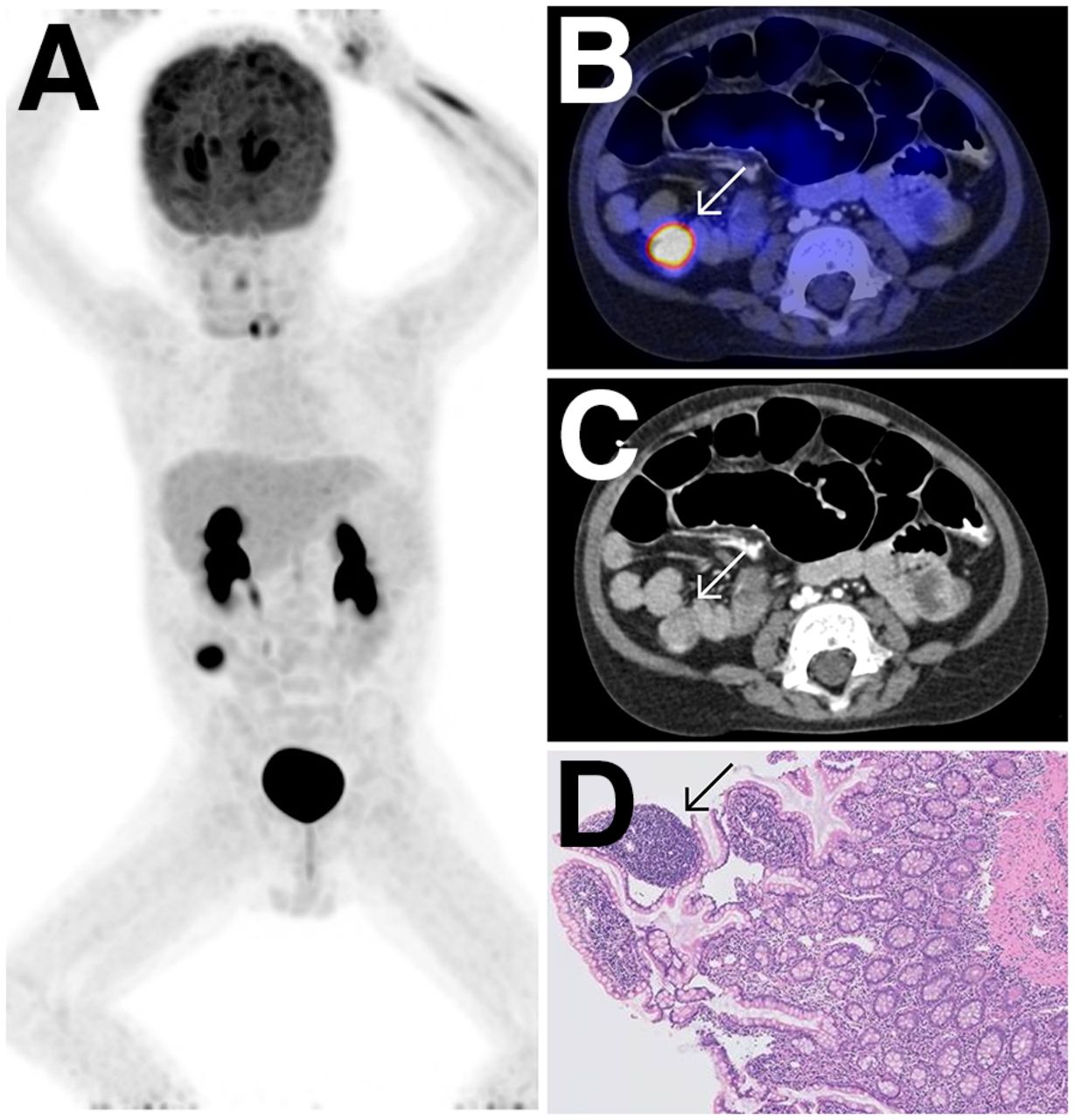
Three-year-old boy 2 y after liver transplantation because of biliary atresia. 18F-FDG PET/CT was requested after 3 cycles of rituximab, cyclophosphamide, vincristine, and prednisone therapy. False-positive interim 18F-FDG PET/CT scan confirmed after biopsy via colonoscopy revealed therapy-induced reactive changes in the cecum. (A and B) Maximum-intensity-projection 18F-FDG PET (A) and axial fused 18F-FDG PET/CT (B) show 18F-FDG–avid lesion in cecum (arrow). (C) On diagnostic CT, spheric mass is seen in cecum (arrow). (D) ×100 magnification with hematoxylin and eosin staining shows lymphoid infiltration without abnormal cells (arrow).
DISCUSSION
This study aimed to evaluate the diagnostic performance of 18F-FDG PET/CT for the detection of PTLD in the pediatric population and to explore its feasibility in the response assessment setting. The results suggest that 18F-FDG PET/CT has a good specificity and positive predictive value but low to moderate sensitivity and negative predictive value for the detection of PTLD in children, especially when disease is localized in the Waldeyer’s ring, cervical lymph nodes or gastrointestinal tract. A positive 18F-FDG PET/CT scan may therefore confirm PTLD suspicion, but a negative 18F-FDG PET/CT does not rule out PTLD.
Studies on the clinical utility of 18F-FDG PET/CT in pediatric PTLD are limited and often combined with adult PTLD cohorts (13,16,17,19). However, considering the essential differences in pathology and presentation of this disease in the 2 population groups, diagnostic performance analyses should be performed separately for children. To date, studies on pediatric PTLD patients have been descriptive in nature, comparing 18F-FDG PET or PET/CT with other imaging modalities (such as CT and MRI) on a lesion by lesion basis and evaluating how additional detected lesions on 18F-FDG PET or PET/CT affected staging and treatment (14,15,18,25). Study populations were often small (range, 7–34 patients), and in 2 of the 4 previous studies on this topic, stand-alone 18F-FDG PET was used instead of the hybrid 18F-FDG PET/CT (14,18). Furthermore, a diagnostic performance analysis (in terms of sensitivity, specificity, positive predictive value, and negative predictive value) for the detection of PTLD was not performed in any of these previous studies.
Although results from mixed and adult cohorts suggest 18F-FDG PET/CT as a viable imaging modality for PTLD detection at diagnosis (sensitivity, 89%–85%; specificity, 91%–89%; positive predictive value, 91%–83%; and negative predictive value, 92%–87%), the high number of false-negative cases in our pediatric patient population impacted the sensitivity and negative predictive value of 18F-FDG PET/CT for PTLD detection (16,26–28). False-negative results in our current study were confirmed in the Waldeyer’s ring (n = 4), cervical lymph nodes (n = 1), and small bowel (n = 2), which were interpreted as physiologic uptake but proved to be either nondestructive or polymorphic PTLD. In pediatric patients particularly, attention should also be paid to the head and neck region. Concerns about false-negative results in the tonsils have been previously reported by Vali et al. (18). Nondestructive PTLD tends to occur at a younger age and is also often limited to the Waldeyer’s ring (1,7). However, uptake in the Waldeyer’s ring is commonly reported in children and not necessarily indicative of pathology, leading to potential misinterpretation of uptake in this area as physiologic (29). Additionally, although reactive 18F-FDG–avid lymph nodes in the cervical region are also often reported in children, cervical malignant lymphadenopathy seems to occur more frequently in PTLD patients than in immunocompetent lymphoma patients (30). The gastrointestinal tract is also a commonly reported PTLD location in pediatric patients (7,31). Physiologic uptake in the gastrointestinal tract may obscure or mimic pathology and give rise to false-negative results (32).
Despite a low to moderate sensitivity and negative predictive value for the detection of PTLD at diagnosis, 18F-FDG PET/CT retains clinical utility in the management of pediatric PTLD patients. Because of the high number of false-negative scans in the tonsils or adenoids, physicians must remain alert for signs that might indicate the presence of disease, such as a high Epstein-Barr virus DNA load and tonsillar hypertrophy (4,33). Nevertheless, if a biopsy is positive for nondestructive PTLD in the tonsils or adenoids but the 18F-FDG PET/CT findings are interpreted as PTLD-negative, the disease might be focal and therapy limited to reduction of immunosuppression (or potentially rituximab) and clinical follow-up. With regard to uptake in the gastrointestinal tract, 1 study has demonstrated that patient preparation with N-butylscopolamine (Buscopan; Boehringer Ingelheim) reduces artifacts in the bowel and improves accuracy (34). Furthermore, CT has also been suggested as a more sensitive modality for PTLD lesion detection in bowel and stomach (18). Patient-specific preparation and an abdominal diagnostic CT scan may be necessary in a selected group of patients if lower-gastrointestinal-tract PTLD is suspected. The high specificity and positive predictive value of 18F-FDG PET/CT in the disease detection setting are clinically relevant, because concerns about false-positive 18F-FDG PET/CT scans, predominately due to inflammation or other malignancies, are often encountered in the literature (26,35). However, compared with adults, the risk of a malignancy (other than PTLD) is decreased in pediatric transplant patients—a fact that may explain the lack of false-positive scans in the disease detection setting in this study (36).
Regarding the potential contribution of 18F-FDG PET/CT during treatment evaluation in pediatric PTLD, there were 40% (2/5) false-positive interim 18F-FDG PET/CT scans. For end-of-treatment 18F-FDG PET/CT, there were 33% (3/9) false-positive and 11% (1/9) false-negative scans. Interim false-positive results were predominantly due to therapy-induced reactive changes. This finding is in line with a systematic review of immunocompetent lymphoma patients by Adams et al. (37), who raised concerns about high proportions of false-positives, with false-positive results reported in 55.7% of all 18F-FDG–avid lesions that were biopsied during and at the end of treatment (most being due to inflammatory changes).
The retrospective nature of this study constitutes a significant limitation. Important variables such as patient selection and the timing of 18F-FDG PET/CT could not be controlled. Because there are currently no guidelines on the use of 18F-FDG PET/CT for the diagnosis of PTLD in pediatric patients, each medical department defined its own criteria for requesting a scan. Previous examinations performed before 18F-FDG PET/CT in the included patients may have influenced the a priori incidence of PTLD and, therefore, diagnostic performance. In addition to potentially inducing a selection bias, the lack of control on patient management variables may also have affected 18F-FDG PET/CT diagnostic performance during treatment evaluation. Taking into consideration the lack of literature and the limitations of retrospective studies, future research on this topic should focus on prospective and multicenter studies.
CONCLUSION
18F-FDG PET/CT showed a good specificity and positive predictive value but a low to moderate sensitivity and negative predictive value for the detection of PTLD in a 28-pediatric-patient cohort with clinical suspicion of this disease. False-negative results were confirmed in the Waldeyer’s ring, cervical lymph nodes, or small bowel with either nondestructive or polymorphic PTLD subtypes. 18F-FDG PET/CT appears to have a limited role in the setting of response assessment for pediatric PTLD, given the observed high proportions of false-positives both at interim and end-of-treatment evaluations.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Is 18F-FDG PET/CT an accurate imaging modality for PTLD detection in pediatric patients with suspicion of the disorder?
PERTINENT FINDINGS: In this single-center retrospective study including 28 patients and 32 scans, the sensitivity, specificity, positive predictive value, and negative predictive value of 18F-FDG PET/CT for the detection of PTLD in children with a clinical suspicion of this disease were 50% (7/14), 100% (18/18), 100% (7/7), and 72% (18/25), respectively. False-negative results were confirmed in the Waldeyer’s ring, cervical lymph nodes, and small bowel with either nondestructive or polymorphic PTLD subtypes.
IMPLICATIONS FOR PATIENT CARE: Clinicians should be aware of the inherent limitations of 18F-FDG PET/CT, paying particular attention to the potential for a focus of disease in the Waldeyer’s ring, cervical lymph nodes, and gastrointestinal tract of pediatric patients.
Footnotes
Published online Jan. 31, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 14, 2019.
- Accepted for publication January 3, 2020.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.