


Abstract
A first analysis of simultaneous 68Ga-prostate-specific membrane antigen (PSMA)-11 PET/MRI showed some improvement in the detection of recurrent disease at low serum prostate specific antigen (PSA) values below 0.5 ng/mL compared with the already high detection rate of 68Ga-PSMA-11 PET/CT. We therefore focused on all patients with biochemical recurrence and PSA values no higher than 0.5 ng/mL to assess the detection rate for 68Ga-PSMA-11 PET/MRI. Methods: We retrospectively analyzed a cohort of 66 consecutive patients who underwent 68Ga-PSMA-11 PET/MRI for biochemical recurrence with a PSA value no higher than 0.5 ng/mL at our institution. Median PSA level was 0.23 ng/mL (range, 0.03–0.5 ng/mL). Detection of PSMA-positive lesions within the prostate fossa, local and distant lymph nodes, bones, or visceral organs was recorded. In addition, all scans with 68Ga-PSMA-11 PET/MRI–positive lesions were retrospectively assessed to analyze if lesions were detected inside or outside a standard salvage radiotherapy volume. Results: Overall, in 36 of 66 patients (54.5%) PSMA-positive lesions were detected; in 26 of 40 (65%) patients with a PSA level between 0.2 and 0.5 ng/mL and in 10 of 26 (38.5%) patients with a PSA level less than 0.2 ng/mL. Even at those low PSA values, only 8 of 66 (12.1%) patients had exclusive local recurrence. Lymph nodes were detected in 23 patients and bone metastases in 5 on 68Ga-PSMA-11 PET/MRI. In 26 of 66 patients (39.4%), PSMA-positive lesions were located outside a standard salvage radiotherapy volume. Conclusion: Our data confirm that 68Ga-PSMA-11 PET/MRI has a high detection rate for recurrent prostate cancer, even at low PSA levels no higher than 0.5 ng/mL. In addition, we show that 68Ga-PSMA-11 PET/MRI detected PSMA-positive lesions outside a standard salvage radiotherapy volume in 39.4% of all patients.
Salvage radiotherapy (sRT) to the prostatic bed is still the only localized treatment option for patients with biochemical recurrence (BR) after radical prostatectomy. Early sRT, before prostate-specific antigen (PSA) levels rise to more than 0.5 ng/mL, will achieve undetectable PSA levels in more than 60% of the patients while providing an 80% change in 5-y progression-free survival (1). Yet, for those 30% of patients for whom there is no effect on PSA levels because of extrapelvic localization of the recurrence, sRT to the prostatic bed is of limited value (2).
Detection rates of choline PET/CT range between only 5% and 24% in patients with BR and PSA levels lower than 1 ng/mL after radical prostatectomy (3). In contrast, a recent metaanalysis demonstrated a detection rate of 45% (95% confidence interval [CI], 39%–52%) using the new 68Ga-labeled PET tracer targeting the prostate-specific membrane antigen (PSMA) in patients with BR and PSA values of 0.2–0.49 ng/mL (4). PSMA-based targeted radiotherapy (RT) might therefore become an option in patients with BR (5,6). However, data about the oncologic outcome of PSMA-based targeted RT is still limited, and ongoing clinical trials have to be completed before definitive conclusions on the effect of targeted salvage treatments can be drawn (7). The superior soft-tissue contrast of PET/MRI might further improve the detection of pelvic lesions, and indeed, first preliminary results for 68Ga-PSMA-11 PET/MRI showed that, especially in patients with very low PSA values, the detection rate was higher than the published results for PET/CT (8). However, this finding was based on a small patient number. Hence, robust results for the performance of PET/MRI in patients with very low PSA values are still missing.
Furthermore, several studies showed that even at low PSA values, the detected lesions are not localized exclusively in the prostatic bed. In these cases, an adaption of the target volume of sRT can be discussed. However, there has not yet been an analysis of the number of cases in which 68Ga-PSMA-11 PET/MRI would possibly lead to a change or modification (e.g., with additional boost) of the target volume compared with classic sRT to the prostate bed, as performed when macroscopic tumor is not detectable in patients with low PSA values. We aimed to analyze the detection rate of 68Ga-PSMA-11 PET/MRI in patients with BR after radical prostatectomy and low PSA values no higher than 0.5 ng/mL. In addition, we aimed to retrospectively assess whether lesions detected by 68Ga-PSMA-11 PET/MRI were detected outside a standard sRT volume.
MATERIALS AND METHODS
Patients
We retrospectively analyzed all patients who underwent 68Ga-PSMA-11 PET/MRI between April 2016 and December 2017 at our department for BR after radical prostatectomy at low PSA values no higher than 0.5 ng/mL. BR was confirmed in all patients by at least 2 consecutive PSA values. Patients with very low PSA values less than 0.2 ng/mL were also included in the present analysis. The local ethics committee approved the study protocol (BASEC; protocol 2016-02230), and all patients gave written informed consent. Twenty patients from the previously published cohort investigating the detection rate of 68Ga-PSMA-11 PET/MRI for all PSA values were included in the present dataset (8). Clinical parameters including PSA, primary tumor stage, Gleason score, and surgical margin status were assessed. The detection rate of PSMA-positive lesions was analyzed overall and for 2 subgroups: very low PSA (0–<0.2 ng/mL) and low PSA (0.2–0.5 ng/mL). Further, the region of detection was assessed (prostatic fossa [including bed of seminal vesicles]; pelvic, paraaortic, mediastinal/supraclavicular, and axillary lymph nodes; bone lesions; and visceral lesions). Detection of PSMA-positive lesions was separately analyzed for patients with prior or ongoing androgen-deprivation therapy (ADT). Patients with castration-resistant prostate cancer were excluded from the present analysis. In addition, SUVmax and lesion size were assessed.
68Ga-PSMA-11 PET/MRI
All patients received a single injection of 68Ga-PSMA-11 (130 ± 16 MBq; range, 90–162 MBq). A clinical routine whole-body PET/MRI exam was performed 60 min after injection on a hybrid scanner (Signa PET/MR; GE Healthcare) used in previous studies at our department (8). In brief, the scanner comprises a 3-T MR system with a time-of-flight PET detector ring installed between the body and gradient coils. A 3-dimensional dual-echo, spoiled gradient-recalled echo sequence (LAVA-flex) for attenuation correction and a PET emission scan were recorded in list mode. The whole-body protocol included 6 bed positions with a 2-min acquisition time for each. Specific sequences covering the pelvis, including a high-resolution T1-weighted LAVA-flex sequence, a T2-weighted fast recovery fast spin-echo sequence in 2 planes, and diffusion-weighted images (b values: 0, 300, and 1,000) were acquired with a 15-min PET frame. Furosemide was injected intravenously 30 min before the 68Ga-PSMA-11 injection (0.13 mg/kg) to reduce halo artifacts (9). For attenuation correction, an atlas-based MR method was used for the head; for the remaining body, segmentation of air, lung, and soft tissue was performed using the Dixon LAVA-flex sequences, generating a fat- and water-based attenuation correction map. The protocol scan time was 30 min.
A dual board-certified radiologist and nuclear medicine physician analyzed all images, incorporating both the MRI and the PET information as well as all clinical information. Furthermore, to investigate interreader variability, 2 additional readouts were conducted. For the second readout, the following clinical information was given: PSA level at scan, stage and grade of primary tumor, surgical margins, and Gleason score. In analogy to our previous publication, only lesions highly suspected of being recurrence were considered positive: focal 68Ga-PSMA-11 uptake in the soft tissue of the prostate bed, lymph nodes with an SUVmax of at least 3 or pathologically increased size (≥5 mm for perirectal nodes, ≥8 mm for iliac/retroperitoneal nodes, and ≥1 cm for inguinal nodes), focal bone uptake with correlating bone marrow replacement, or focal uptake with a correlating soft-tissue lesion (8). Most published series suggested an SUVmax of 2–3 as an appropriate cutoff, especially for lymph nodes (10,11). To minimize false-positive interpretation of slightly PSMA-positive findings, a cutoff of 3 was selected.
Retrospective Evaluation of RT Volume
All scans with 68Ga-PSMA-11 PET/MRI–positive lesions were reviewed according to the guidelines of the European Organization for Research and Treatment of Cancer and the Radiation Therapy Oncology Group (12,13). Based on initial tumor stage, nodal status, and surgical margins, as well as PSA value, the appropriate target volume for sRT was retrospectively defined on the basis of both guidelines. If the 68Ga-PSMA-11 PET/MRI–positive lesions were located outside a standard sRT volume, a change in RT target volume was given.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics, version 25 (IBM). Prism, version 7 (GraphPad Software, Inc.), was used to generate all images. Intraclass correlation coefficients were used to assess interreader agreement. Ninety-five percent CIs are reported for κ-values. Interpretation of κ-values and intraclass correlation coefficients was based on a classification established by Landis and Koch: poor reproducibility, 0.0; slight reproducibility, 0.0–0.20; fair reproducibility, 0.21–0.40; moderate reproducibility, 0.41–0.60; good reproducibility, 0.61–0.80; and almost-perfect reproducibility, 0.81–1.00 (14).
RESULTS
Patient Characteristics and 68Ga-PSMA-11 PET/MRI Detection Rate
This study included 66 patients. Their characteristics are summarized in Table 1.
Clinical Patient Characteristics (n = 66)
The 68Ga-PSMA-11 PET/MRI detection patterns for all patients are given in Tables 2 and 3. The overall detection rate was 54.5%, including patients with prior or ongoing ADT. Subgroup analysis showed a detection rate of 38.5% in patients with a very low PSA level (0–<0.2 ng/mL) and of 65.0% in patients with a low PSA level (0.2–0.5 ng/mL). Exclusion of patients with prior or ongoing ADT slightly reduced the overall detection rate to 51.6%, as well as the detection rate in the subgroups with very low PSA (33.3%) and low PSA (63.2%) (Fig. 1).
Overall Detection Rate in Patients with PSA Values ≤ 0.2 ng/mL (Patients 1–26)
Overall Detection Rate in Patients with PSA Values 0.2–0.5 ng/mL (Patients 27–66)

68Ga-PSMA-11 PET/MRI detection rate stratified by different PSA levels at time of scan. Separate analysis was performed including patients with ongoing or prior ADT. Data are percentage of events.
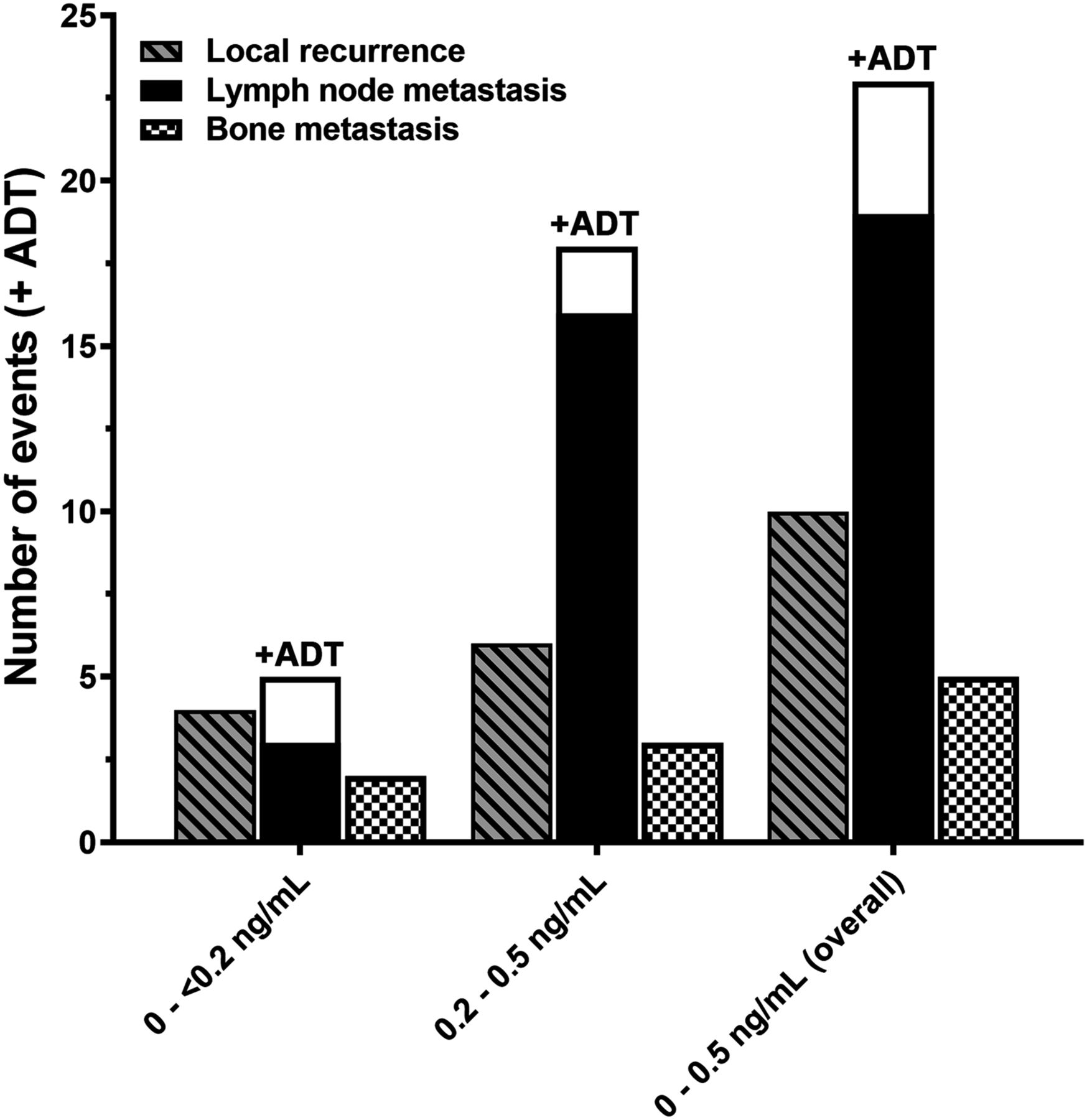
Localization of suggestive lesions is shown in Figure 2. Overall, suggestive lesions were found in the prostatic bed (local recurrence) of 15.1% (n = 10), in the lymph nodes of 34.8% (n = 23), and in the bones of 7.6% (n = 5). In 20 of 23 positive lymph nodes, the maximum short axis was less than 8 mm, in 2 cases it was 8 mm, and in 1 case it was 1 cm. In the subgroup with very low PSA, suspected local recurrence was found in 15.3% (n = 4) of the total cohort (n = 26), lymph node metastasis in 19.2% (n = 5), and bone metastasis in 7.6% (n = 2). In the low-PSA subgroup, local recurrence was detected in 15% (n = 6), lymph node metastasis in 45% (n = 18), and bone metastasis in 7.5% (n = 3). A second analysis was performed with exclusion of all previously reported patients (n = 20) (8). In the second analysis, the overall detection rate was 51.1%, and the detection rate in the subgroups with very low PSA and low PSA was 35.3% and 60%, respectively. In addition, we summarized the published literature regarding the detection rate of PSMA-positive lesions in patients with low PSA values no higher than 1.0 ng/mL (Table 4).
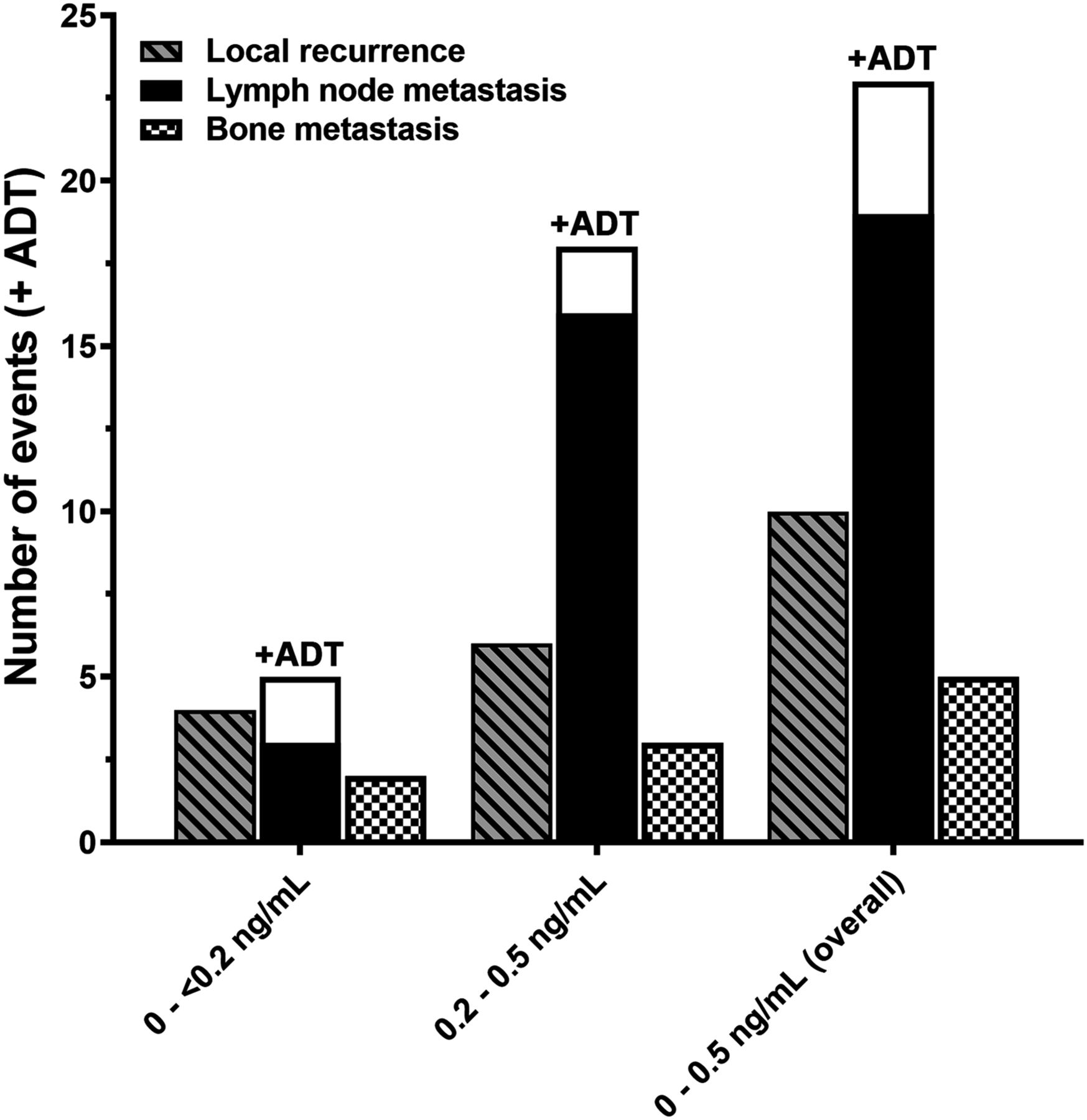
Number of 68Ga-PSMA-11 PET/MRI-positive events stratified by localization and PSA level at time of scan. ADT before scanning increased detection of positive lymph node metastases. Data are total number of events.
Reported Detection Rates in Patients with Very Low PSA Values at Scanning
Localization of 68Ga-PSMA-11 PET/MRI–Positive Lesions Within a Standard sRT Volume
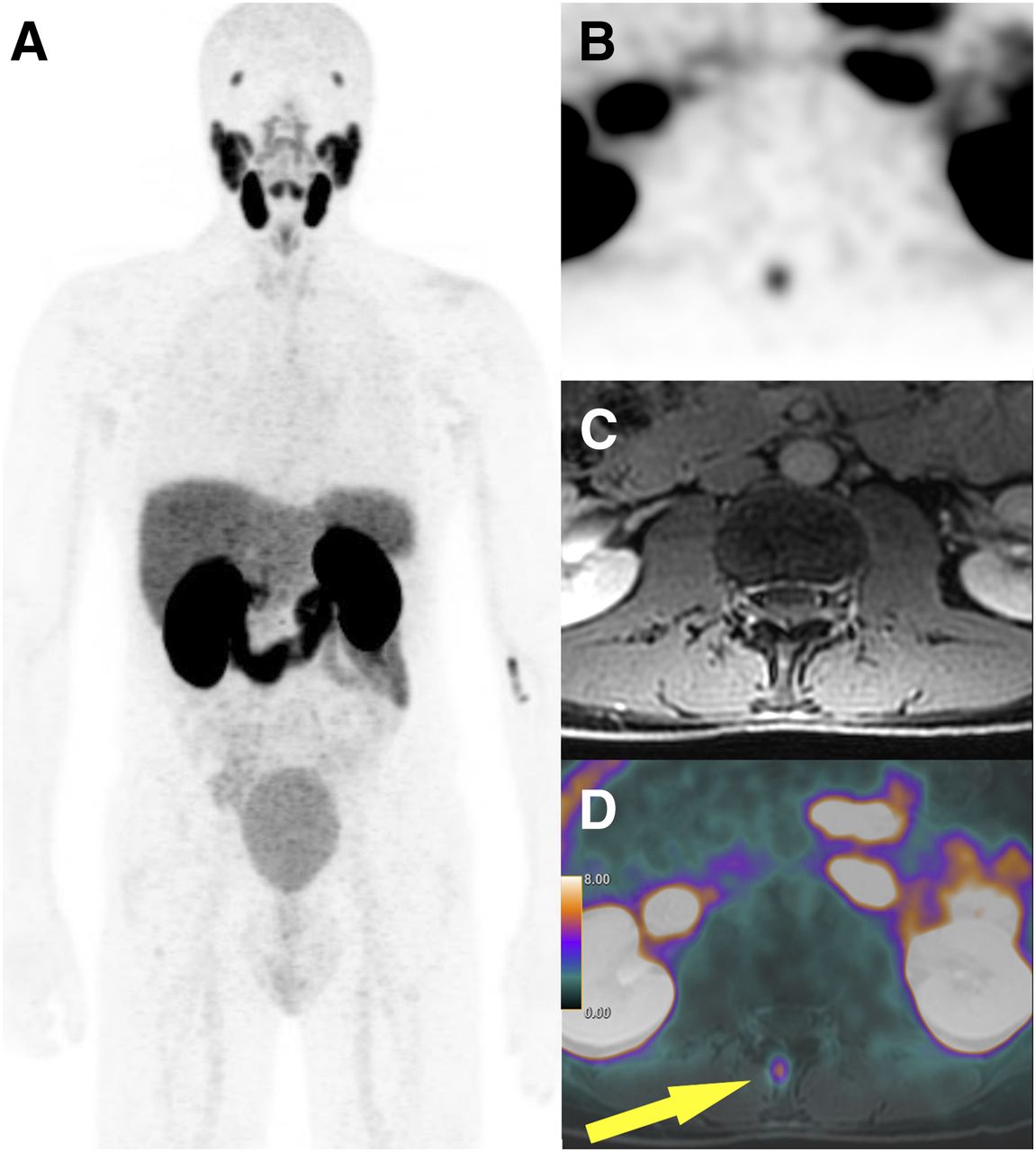
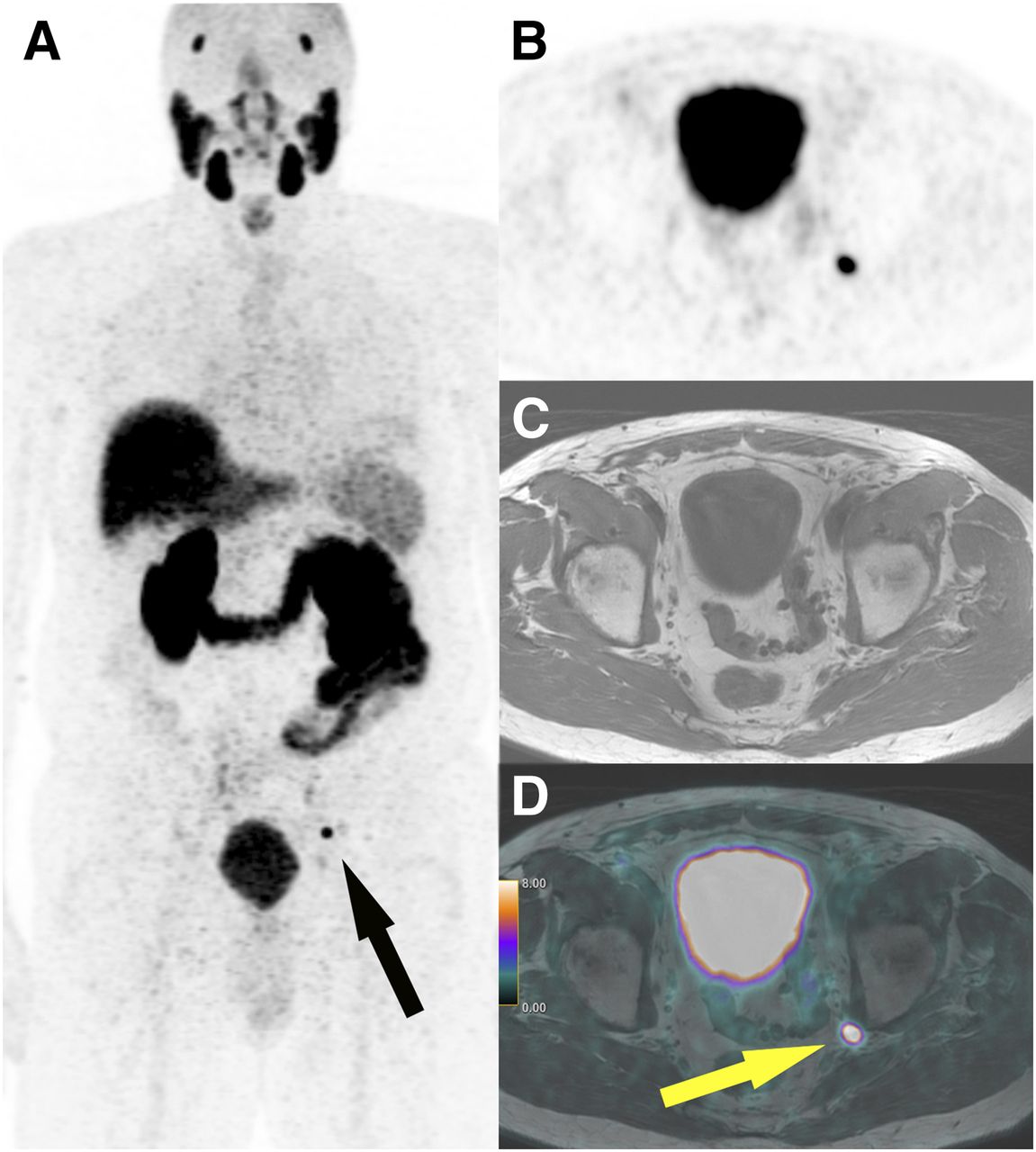
A reanalysis of all patients with positive findings on 68Ga-PSMA-11 PET/MRI discovered that in 26 of 36 patients (72.2%) with positive lesions, at least 1 lesion would not have been covered by the standard RT target volume. In all 8 patients with previous RT, PSMA-positive findings were found outside a standard RT target volume. In 18 of 28 patients without previous RT, PSMA-positive lesions outside a standard RT target volume were detected. Overall, 68Ga-PSMA-11 PET/MRI detected PSMA-positive lesions outside a standard RT target volume in 26 of 66 patients (39.4%). An example of an unexpected bone metastasis that would have changed the RT target volume is given in Figure 3. In 4 patients, the PSMA-positive finding would have led to an additional boost to the focal finding; an example is given in Figure 4. In only 11 patients (16.6%) with PSMA-positive findings would neither the RT target volume nor the dosing have been changed by 68Ga-PSMA-11 PET/MRI findings.
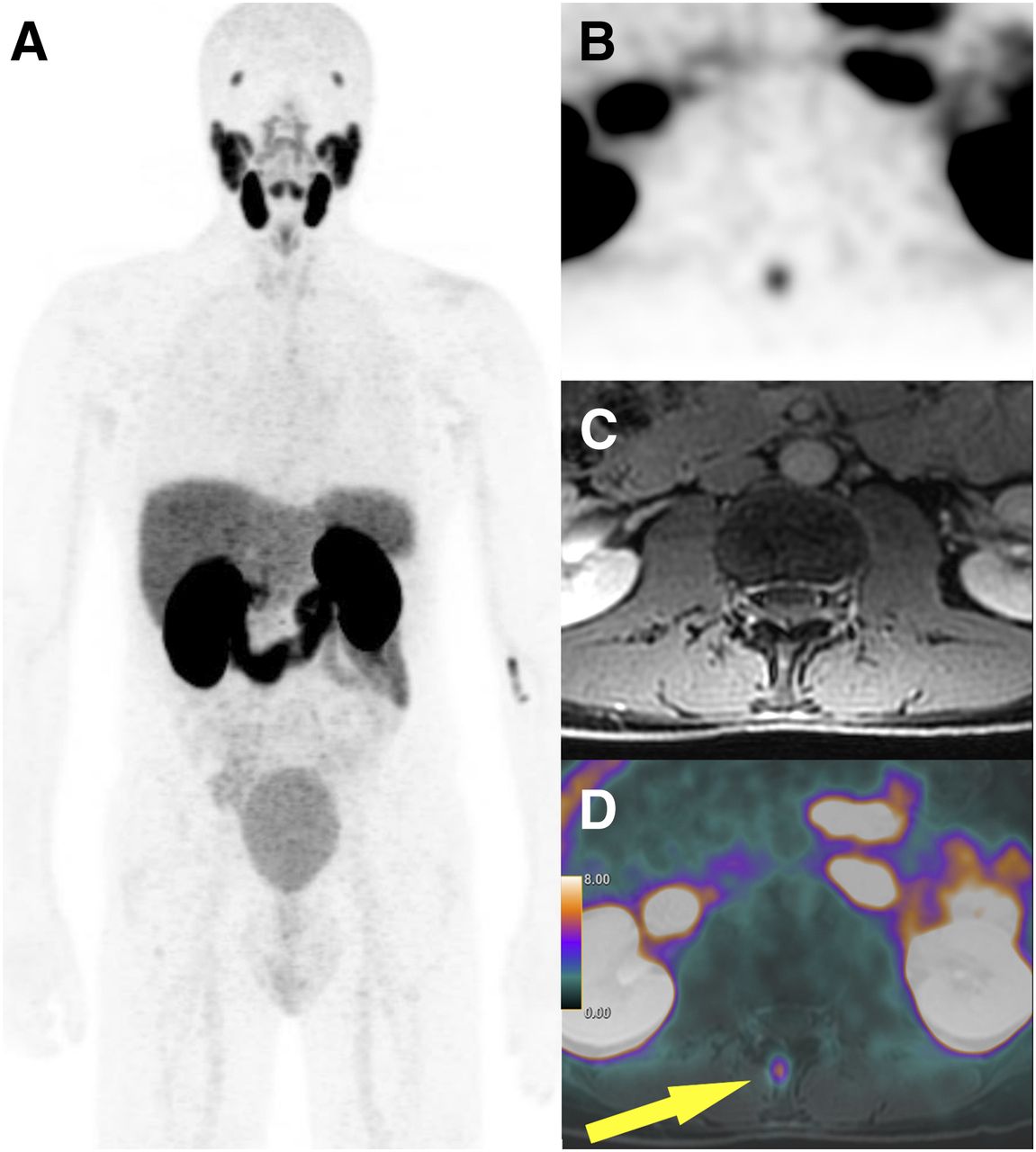
A 57-y-old patient referred for 68Ga-PSMA-11 PET/MRI after prostatectomy for pT1c, pN0, cM0, Gleason 7 tumor with PSA level of 0.5 ng/mL. (A) No clearly delineated focal uptake is seen on coronal maximum-intensity PET projection. (B and C) On axial PET image, focal uptake is seen in processus spinosus of 12th thoracic vertebra (SUVmax, 5.6) (B), corresponding to minimally contrast-enhancing focus on axial T1-weighted fat-saturation image (C). (D) Correlation is confirmed on fused image (arrow).
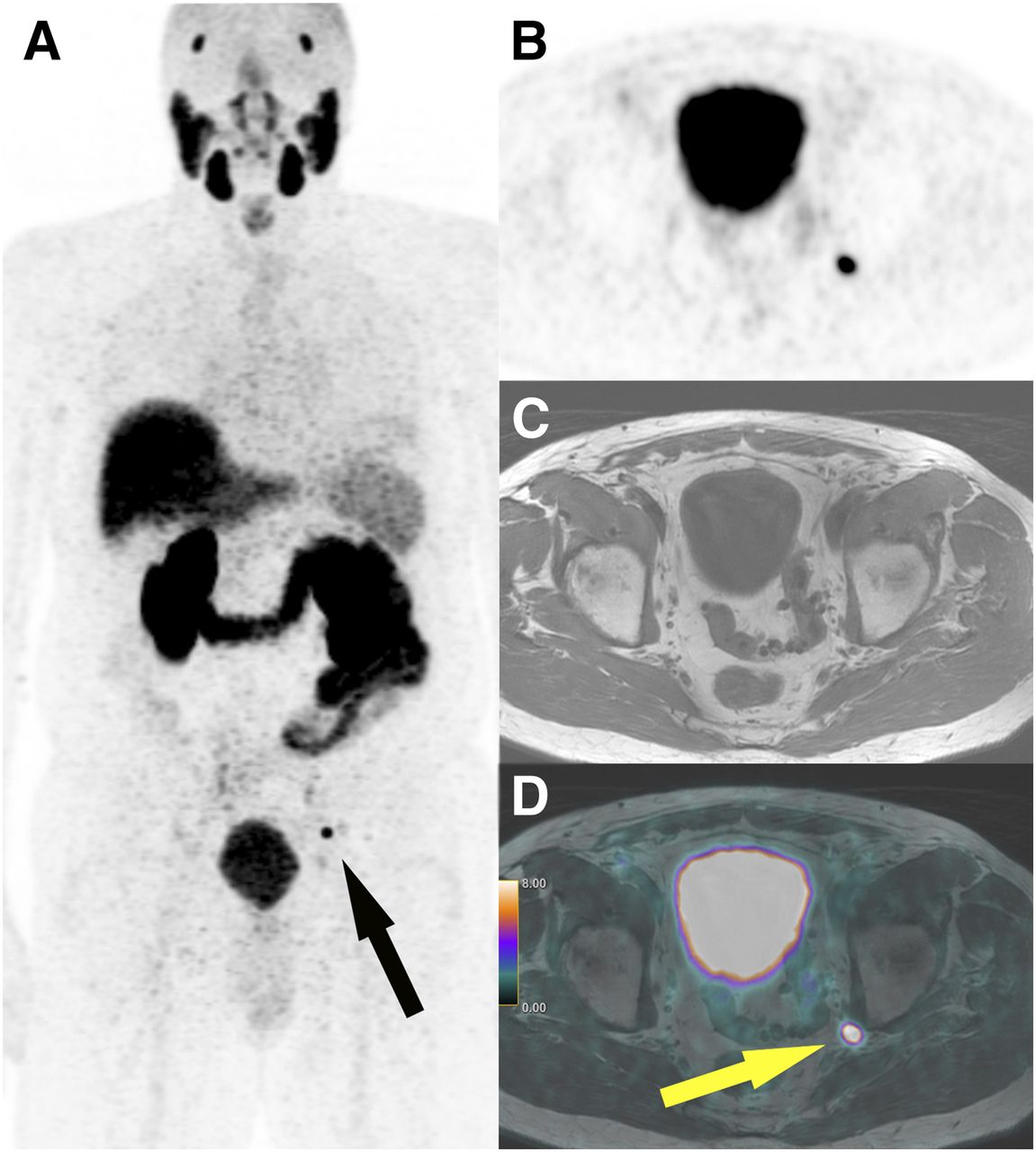
A 73-y-old patient referred for 68Ga-PSMA-11 PET/MRI after prostatectomy for pT3a, pN0, cM0, Gleason 7 tumor with rise in PSA level to 0.41 ng/mL 3.5 y after prostatectomy. (A) Coronal maximum-intensity PET projection shows solitary intense focal PSMA uptake in left internal iliac area (arrow). (B and C) Axial PET image confirms local uptake (SUVmax, 23) (B), corresponding to nonenlarged lymph node in left iliac internal region on axial T1-weighted sequence (C) and on fused PET/MRI (arrow) (D). Our radiation oncologist assessed this finding as indicating need to change radiation plan.
Overall Interreader Agreement
Generally, the interreader agreement for all 3 readers was almost perfect (κ = 0.855; 95% CI, 0.782–0.907). An almost-perfect agreement was also detected for lymph node metastases (0.914; 95% CI, 0.870–0.94), for local recurrence (0.903; 95% CI, 0.855–0.938), and for bone metastases (0.851; 95% CI, 0.776–0.904).
DISCUSSION
In this study, we confirmed the previously reported promising detection rate for 68Ga-PSMA-11 PET/MRI even in patients with PSA values of 0.5 ng/mL or lower. An overall detection rate of 65% was observed in patients with PSA values between 0.2 and 0.5 ng/mL. Even at low PSA values of 0.5 ng/mL or lower, only 12.1% of all patients had PSMA-positive recurrent disease limited to the prostatic bed, and extrapelvic disease was detected in 13.6% of the cohort. Overall, 68Ga-PSMA-11 PET/MRI would have changed the standard sRT volume in 39.4% of all patients.
Given the improved opportunity for a cure when sRT is performed on patients with PSA values below 0.5 ng/mL, a precise restaging for patients with BR after radical prostatectomy is of the utmost interest. Ceci et al. published the hitherto largest cohort of 138 prospective patients with PSA values between 0.2 and 0.5 ng/mL and found a detection rate of 37.9% using 68Ga-PSMA-11 PET/CT (15). In the same PSA range, Rauscher et al. presented a detection rate of 55% in 134 retrospectively analyzed patients (16). Farolfi et al. reported an overall detection rate of 34.4% in 119 patients (17). In addition, Afshar-Oromieh et al. described a detection rate of 46% in 108 patients (18). However, their cohort included patients not only after primary radical prostatectomy but also after primary radiation therapy, which might influence the detection rate. Others reported only small cohorts of 10–24 patients and found detection rates between 36% and 57.9% (19–22). In our 68Ga-PSMA-11 PET/MRI cohort, we observed a considerably higher detection rate of 65% in patients presenting with PSA values between 0.2 and 0.5 ng/mL at the time of the scan. Published data on the detection rate in patients with even lower PSA values (<0.2 ng/mL) are scarce and include only small patient cohorts (18,19,22,23). Reported detection rates for this cohort with a very low PSA range between 33% and 47.1%. We observed a detection rate of 38.5% for patients with very low PSA values (<0.2 ng/mL).
In our cohort, only 8 of 66 patients (12.1%) were found to have PSMA-positive lesions limited to the prostatic bed. The most common site for PSMA-positive recurrence was lymph nodes. However, only 13% of the PSMA-positive lymph nodes were larger than 8 mm. This is even slightly lower than the published data of Giesel et al., which showed that only around 36% of the lymph nodes detected on 68Ga-PSMA-11 PET/CT are pathologically enlarged (10).
Besides PSA levels, other factors influencing the detection rate of 68Ga-PSMA-11 PET imaging are currently under investigation. First preclinical data suggest that ADT might increase PSMA expression in vitro and in vivo (24–26). A case study by Hope et al. showed a 7-fold increase in PSMA uptake in a patient treated for 4 wk with ADT (27). Rauscher et al. published a first investigation trying to define predictors for 68Ga-PSMA-11 PET/CT positivity in a retrospective cohort of 272 patients after radical prostatectomy (16). In a multivariate analysis, they found that the PSA value at the time of scanning (odds ratio, 4.20; 95% CI, 1.15–15.37) and concurrent ADT (odds ratio, 9.25; 95% CI, 1.17–73.31) are significant independent predictors of 68Ga-PSMA-11 PET/CT positivity. On the other hand, a first prospective trial in 8 patients with serial 68Ga-PSMA-11 PET scans 9, 18, and 28 d after the start of ADT did not confirm the expected transient rise in 68Ga-PSMA-11 uptake (28), and a retrospective analysis of 10 patients found that continuous long-term ADT between 42 and 369 d significantly reduced the visibility of castration-sensitive prostate cancer in 68Ga-PSMA-11 PET/CT (29). In our cohort, only 4 patients had ongoing or prior ADT at the time of the scan. In all these patients, PSMA-positive lymph nodes were found, even at very low PSA values. However, additional investigations are needed to further elucidate the impact of ADT on the uptake of 68Ga-PSMA-11 in different settings and tumor stages. Apart from these factors, PSMA tracer kinetics also seem to affect the detection rate in patients with BR. The newly introduced 18F-PSMA-1007 shows only minimal activity in the urinary tract, possibly improving the detection of local recurrence or locoregional lymph nodes (30,31). However, studies directly comparing the detection rate of 68Ga-PSMA-11 and 18F-PSMA-1007 have not yet been performed.
In addition, a rapidly increasing body of literature investigates the alteration of RT target management based on 68Ga-PSMA-11 imaging. However, these are commonly rather small cohorts with a wide PSA range. A change in RT target planning or management was described in 50%–77% of all patients using 68Ga-PSMA-11 PET/CT (32–34). In addition, it has been shown that a 68Ga-PSMA-11 PET/CT–based RT target leads to a significant PSA response in patients with BR (5,6). In our cohort, 68Ga-PSMA-11 PET/MRI–positive lesions outside a standard RT target volume were found in more than 70% of all patients with PSMA-positive lesions. However, the impact of targeted RT on cancer-specific survival or time to cancer recurrence is still unknown. Future investigations will be needed to reveal whether targeted treatment of oligometastatic disease based on 68Ga-PSMA-11 PET/MRI improves cancer-specific survival.
A limitation of our study is its retrospective nature, leading to an inherent selection bias. Because of the retrospective data acquisition, there is a lack of clinical information in some patients. Furthermore, the reported patient collective is still relatively small and lacks a comparison to the histopathology of PSMA-positive lesions. However, it is the largest cohort investigating the impact of 68Ga-PSMA-11 PET/MRI in patients with very low PSA values and recurrent prostate cancer.
CONCLUSION
Our data confirm that 68Ga-PSMA-11 PET/MRI has a high detection rate for recurrent prostate cancer even at low PSA levels no higher than 0.5 ng/mL. In addition, we show that 68Ga-PSMA-11 PET/MRI detected PSMA-positive lesions outside a standard sRT volume in nearly 40% of all patients.
DISCLOSURE
The Department of Nuclear Medicine holds an institutional Research Contract with GE Healthcare. We thank the Sick Legat and the Iten-Kohaut Foundation for their financial support. Irene Burger and Philipp Kaufmann have received research grants and speaker honoraria from GE Healthcare. Irene Burger received research grants from Swiss Life and speaker honoraria from Bayer Health Care and Astellas Pharma AG. Matthias Guckenberger has received research grants from Varian. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How many PSMA-positive lesions were located outside a standard sRT field within the presented cohort?
PERTINENT FINDINGS: This retrospective analysis focusing on the detection rate for 68Ga-PSMA-11 PET/MRI in patients with recurrent prostate cancer and low PSA values no higher than 0.5 ng/mL revealed an overall detection rate of 54.5%. Moreover, in 65% of all patients with a PSA level between 0.2 and 0.5 ng/mL, PSMA-positive lesions were detected, making this imaging modality a promising tool for restaging of prostate cancer.
IMPLICATIONS FOR PATIENT CARE: The results of this study encourage further investigation of the value of 68Ga-PSMA-11 PET/MRI in patients with recurrent prostate cancer and low PSA values.
Acknowledgments
We acknowledge the technician Marlena Hofbauer and her team for the excellent work on high-quality PET/MRI images.
Footnotes
Published online Aug. 2, 2019.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication January 2, 2019.
- Accepted for publication July 22, 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}