


Abstract
At diagnosis, 22% of colorectal cancer (CRC) patients have metastases, and 50% later develop metastasis. Peptide receptor radionuclide therapy (PRRT), such as 177Lu-PSMA-617, is used to treat metastatic prostate cancer. 177Lu-PSMA-617 targets prostate-specific membrane antigen (PSMA), a cell-surface protein enriched in prostate cancer and the neovasculature of other solid tumors, including CRC. We performed 68Ga-PSMA-11 PET/CT imaging of 10 patients with metastatic CRC to assess metastasis avidity. Eight patients had lesions lacking avidity, and 2 had solitary metastases exhibiting very low avidity. Despite expression of PSMA in CRC neovasculature, none of the patients exhibited tumor avidity sufficient to be considered for 177Lu-PSMA-617 PRRT.
Colorectal cancer (CRC) is the fourth most common cause of cancer-related death (1). At diagnosis, 22% of patients have metastases, and 50% develop metastasis during their lifetime (1).
Theranostics uses tumor-selective ligands conjugated to radionuclides and cytotoxic agents for, respectively, cancer imaging and treatment (2). By targeting tumor cell-surface antigens, these agents are delivered selectively to malignancies (2). Using a diagnostic positron-emitting radionuclide and PET, tumor burden is quantified and response to therapy predicted on the basis of tumor avidity (2). In peptide receptor radionuclide therapy (PRRT), therapeutic α- or β-emitting radionuclides, conjugated to the same PET imaging target, induce DNA damage and cell death (2). PRRT is a mainstay treatment for neuroendocrine tumors and is emerging for metastatic prostate cancer (PC) (2).
The PRRT target prostate-specific membrane antigen (PSMA) is enriched in metastatic PC and has low expression in normal tissues (3,4). It is also elevated on the endothelial cells of certain solid tumors, including CRC, where 75%–80% of primary tumors and metastases express PSMA, which correlates with poor outcome (5,6). PSMA-11, a high-specificity and high-affinity ligand for PSMA that incorporates a radiometal chelator (7), is applied for PET imaging of metastatic PC using 68Ga-PSMA-11 (8) and PRRT using 177Lu-PSMA-617 (9).
Several case reports note CRC avidity during 68Ga-PSMA-11 imaging for metastatic PC, potentially supporting PSMA-targeted PRRT in advanced CRC (10,11). Responding to a recent call for prospective studies in place of incidental case reports or series (12), we assessed metastatic CRC avidity for 68Ga-PSMA-11 to determine whether the avidity meets the criteria for 177Lu-PSMA-617 PRRT.
MATERIALS AND METHODS
Patients
Inclusion and exclusion criteria (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org) and sample size (n = 10) were from PET imaging studies assessing tumor avidity (8,13,14). Recruitment would continue if initial results indicated that at least 30% of patients met the TheraP trial (NCT03392428) criteria to progress to PRRT.
PET Scans and Interpretation
The study had Human Research Ethics Committee approval (HREC/18/QPCH/51). Recruitment was from August to November 2018. Imaging used PSMA-11 (HBED-CC; ABX). 68Ga was labeled as previously described (15), with a labeling efficiency of more than 98%. PET and CT images were reconstructed, and SUVmax and tumor-to-liver (background) SUVmax ratio were determined as previously described (16). 18F-FDG PET/CT or contrast-enhanced CT localized metastases of low 68Ga-PSMA-11 avidity, and SUVmax was compared between 68Ga-PSMA-11 PET, 18F-FDG PET, and contrast-enhanced CT. The TheraP trial criteria to stratify patients as likely responders to PRRT required an SUVmax of at least 10 at all tumor sites not subject to partial-volume artifact (i.e., >10 mm in diameter), an SUVmax of more than 20 at the most avid site, and 68Ga-PSMA-11 avidity higher than 18F-FDG avidity at all sites, when recent 18F-FDG imaging was available (17).
Immunohistochemistry
The study had Human Research Ethics Committee approval (HREC/11/QRBW/453; P2139). Immunohistochemistry was performed on a tissue microarray of matched CRC primary tumors and metastases from 37 patients, using anti-PSMA clone 3E6 (Agilent) and Biocare Medical MACH1 mouse horseradish peroxidase polymer. Signal was quantified by a pathologist as nil, weak, moderate, or strong on the basis of, respectively, no, ≤2.5%, ≥2.5–≤4.5%, or ≥4.5% positive tumor cells.
Statistical Methods
Statistics were performed using Prism (version 7; GraphPad). Data represent the highest SUVmax of representative lesions per anatomic region. Quantification was consistent with the reporting guidelines of the Standards for Reporting of Diagnostic Accuracy Studies (18).
RESULTS
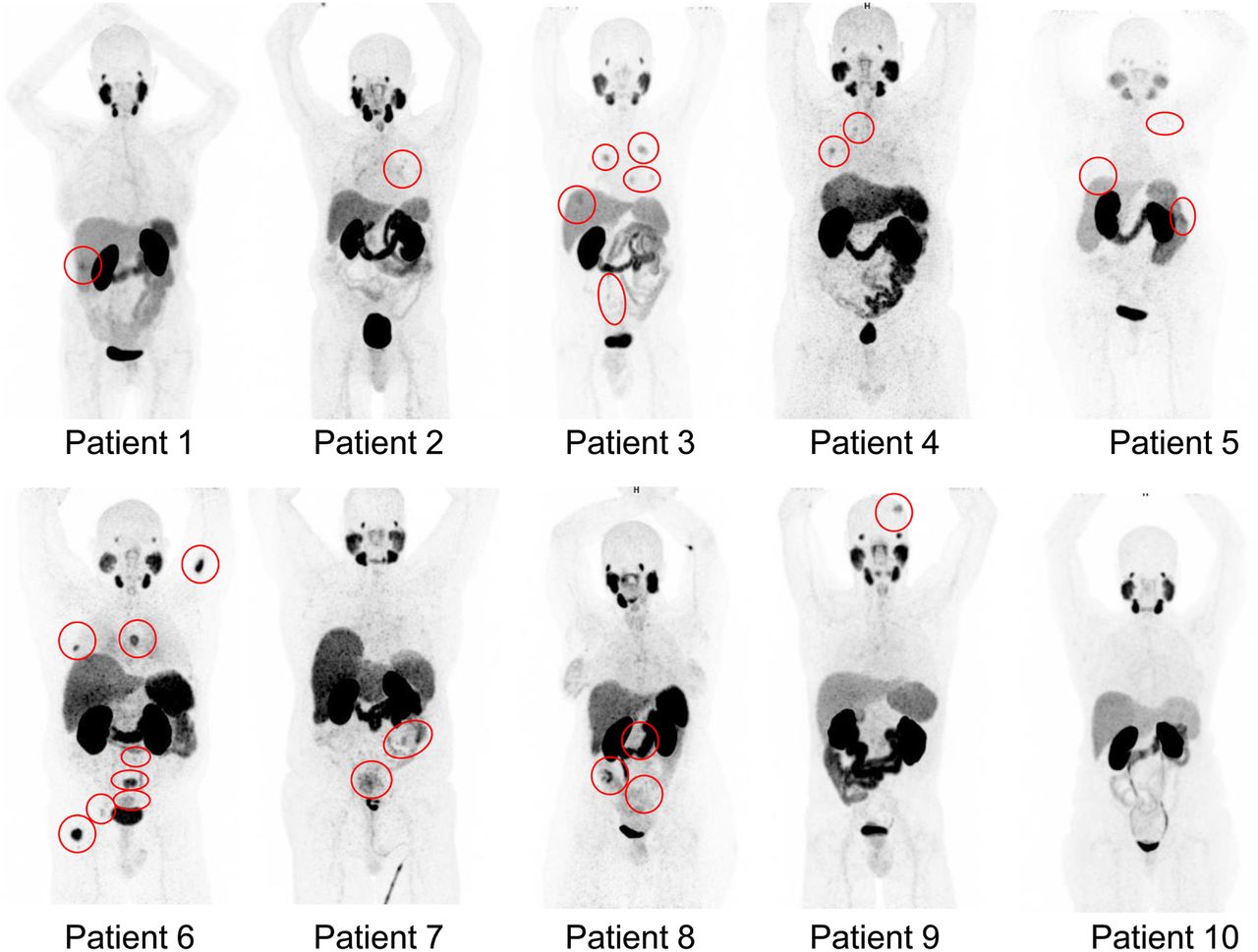
68Ga-PSMA-11 PET imaging of 10 patients with metastatic CRC (Supplemental Tables 2 and 3) resulted in no adverse events. Maximum-intensity projections of participants are shown in Figure 1, and SUVmax is in Figure 2, including TheraP criteria 1 and 2 (19). The metastases of all patients fell significantly short of satisfying criteria 1 and 2, except for liver lesions in patient 3 and lymph nodes in patient 8. Liver metastases in patient 3 met criterion 1 but not criterion 2. Patient 3 had synchronous lung and omental metastases that had insufficient avidity to satisfy criteria 1 and 2. Primary tumor and pelvic lymph node metastases in patient 8 exhibited avidity greater than criterion 1 but not criterion 2. This patient also had locoregional lymph node metastases that failed to satisfy criteria 1 and 2. Two of 3 patients with primary tumors (patients 6 and 7) failed to satisfy both criterion 1 and criterion 2. Bone metastases in patient 6 had the greatest avidity of all lesions and satisfied criterion 1 but fell just short of satisfying criterion 2. Locoregional and retroperitoneal lymph nodes and adrenal metastases in patient 6 failed to satisfy both criterion 1 and criterion 2.

68Ga-PSMA-11 PET maximum-intensity-projection images of patients with metastatic CRC. Red circles = avid lesions.

SUVmax of 68Ga-PSMA-11 metastatic CRCs. Green line = TheraP criterion 1, SUVmax ≥ 10, required at all sites. Red line = criterion 2, SUVmax > 20, required at most avid site.
Also of note, patient metastases lacked consistency in tumor-to-liver SUVmax ratios (Fig. 3) and no patient satisfied criterion 3 that 68Ga-PSMA-11 avidity be greater than 18F-FDG avidity (Supplemental Table 4). Supplemental Table 5 lists the lesions of each patient as detected by 18F-FDG PET, contrast-enhanced CT, and 68Ga-PSMA-11 PET, including the number missed by 68Ga-PSMA-11 PET. The time between 68Ga-PSMA-11 PET imaging and 18F-FDG PET or contrast-enhanced CT is provided in Supplemental Table 6. Eight of 10 patients (patients 2, 3, 4, 5, 6, 7, 8, and 10) had lesions detected by 18F-FDG PET or contrast-enhanced CT but missed by 68Ga-PSMA-11 PET. Liver and lymph node metastases in patients 1 and 8 had heterogeneous uptake, with only a portion of lesions avid. Although patient 6 had bone metastases with significantly higher avidity during 68Ga-PSMA-11 PET than other soft-tissue and visceral lesions, avidity was still significantly lower than 18F-FDG PET avidity. Supplemental Figure 1 provides representative images of pelvic lymph node metastases with negligible avidity during 68Ga-PSMA-11 PET, compared with high 18F-FDG avidity, for patients 7 and 8. No lesions were detected by 68Ga-PSMA-11 PET that were not also identified during 18F-FDG PET. Patients 2, 3, 4, 9, and 10 had previously received neoadjuvant, adjuvant, or palliative chemotherapy, with patient 3 receiving palliative chemotherapy 8 weeks before 68Ga-PSMA-11 PET, which likely had minimal effect on avidity because tumor response was poor. For the remaining 4 patients, at least 7 months had elapsed since chemotherapy.
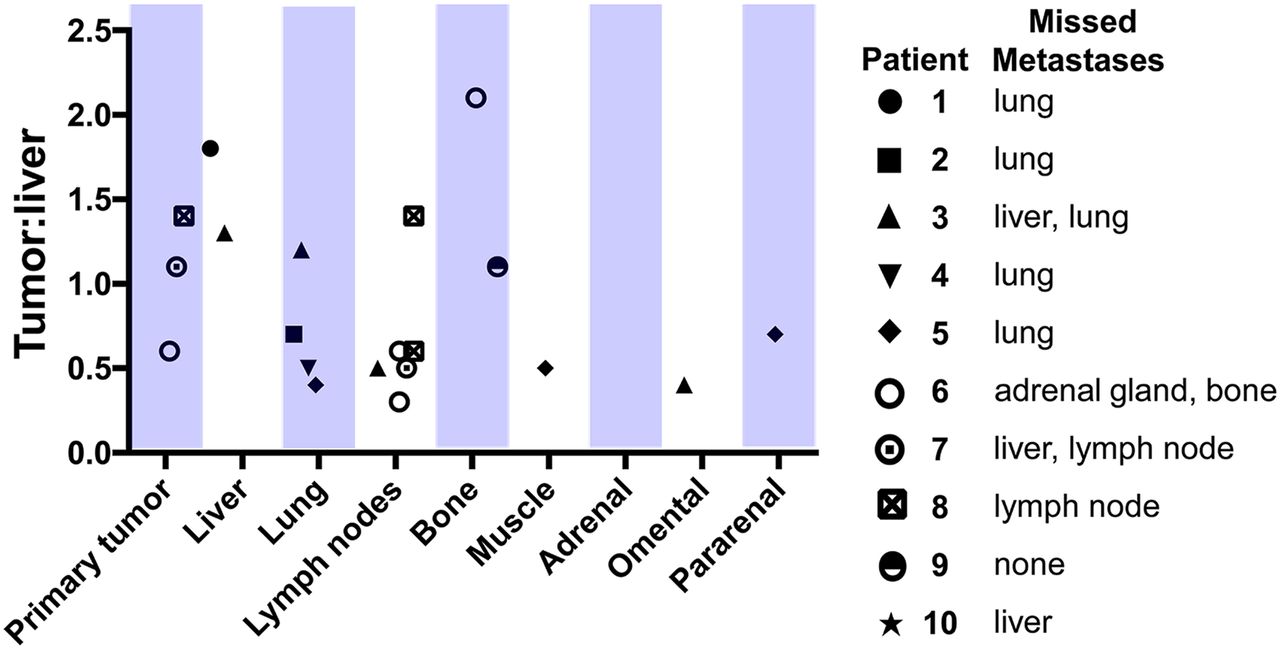
CRC tumor-to-liver (background) SUVmax.
Because resected tumors from the 10 patients were unavailable to explore the reason for the lack of tumor avidity, we performed immunohistochemistry for PSMA in matched primary tumors and metastases from an independent cohort of 37 patients (Supplemental Tables 7 and 8). PSMA was exclusive to endothelial cells of the tumor vasculature, which consistently comprised about 5% of the cells in tumors. Representative images of tumor regions displaying moderate (≥2.5–≤ 4.5% positive cells) and strong (≥4.5% positive cells) PSMA expression (Supplemental Fig. 2A) demonstrate that tumor expression was consistently very low. Quantitative analyses indicated that the invasive edge of 79% of primary tumors and 87% of central regions of primary tumors had nil or weak PSMA expression (Supplemental Figure 2B), with levels consistent between tumor regions (Supplemental Fig. 2C). In metastases, the invasive edge of tumors and the central region of 95% of tumors displayed nil or weak PSMA expression (Supplemental Fig. 2D), and expression was also consistent between these regions of metastases (Supplemental Fig. 2E). These data suggest that the low observed PSMA ligand avidity was due to consistently low PSMA expression in CRC tumors.
DISCUSSION
Responding to the recent call for prospective trials to assess the utility of PSMA-targeted theranostic agents for cancers beyond PC (12), this study indicated that 68Ga-PSMA-11 PET has low avidity in metastatic CRC, with heterogeneous or nonexistent uptake in lesions. A range of factors may contribute to low tumor avidity, the most likely of which is low PSMA expression on tumor vasculature. Although PSMA expression has been reported on colorectal neovasculature (5,6), PSMA messenger RNA is 10–20 times lower in CRC than in PC (19), with our immunohistochemistry confirming low PSMA protein levels in CRC vasculature.
Although it is also possible that low avidity was due to a lack of homing of 68Ga-PSMA-11 to CRC tumors, this is unlikely because we used a protocol that identifies metastatic PC and allows sufficient time for radioligand circulation, antigen binding, and internalization by PSMA-expressing cells (8). Other potential contributing factors include heterogeneous neovascularization and microvessel density in CRC lesions (20), tumor coopting of normal vessels lacking PSMA expression (21), and vascular mimicry with tumor blood-conducting channels lined by malignant cells (22).
We estimated that 68Ga-PSMA-11 PET for metastatic CRC can be beneficial if tumor avidity is sufficient to progress at least 30% of patients to PRRT. However, none of the patients had sufficient avidity to progress to PRRT. Because our sample size was small, we cannot be definitive that 68Ga-PSMA-11 PET is not justified for CRC. However, we note that, using binomial probability, there was only a very small chance (3%) that none of the 10 patients would have sufficient tumor avidity to warrant PRRT, justifying our decision not to continue recruitment beyond 10 patients.
CONCLUSION
68Ga-PSMA-11 PET/CT is not sufficiently sensitive to detect metastatic CRC. Further research is required to identify cell-surface receptors as theranostic targets for imaging and treatment of CRC metastasis.
DISCLOSURE
The study was supported by the Redcliffe Private Practice Fund, the Royal Brisbane and Women’s Hospital Foundation, and the Mater Foundation. No other potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: Can PSMA expression on CRC neovasculature be targeted using 68Ga-PSMA-11 with high sensitivity and avidity to qualify patients for 177Lu-PSMA-617 therapy?
PERTINENT FINDINGS: This prospective pilot study assessed the tumor avidity of 10 patients with metastatic CRC using 68Ga-PSMA-11. Overall, 68Ga-PSMA-11 was insensitive in detecting CRC metastases. Identified lesions had avidity that was insufficient to warrant PSMA-targeted therapy.
IMPLICATIONS FOR PATIENT CARE: Theranostic ligands targeting specific receptors on metastatic CRC cells should be sought in place of targeting PSMA expressed by tumor neovasculature.
Acknowledgments
We acknowledge the generous support of the Royal Brisbane and Women’s Hospital radiochemistry staff in performing radiolabeling, the Herston Imaging Research Facility in performing PET/CT imaging, and the Royal Brisbane and Women’s Hospital and the Redcliffe Hospital in recruiting patients.
Footnotes
Published online May 1, 2020.
- © 2020 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication July 20, 2019.
- Accepted for publication March 9, 2020.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.