


Abstract
Biochemical recurrence (BCR) after prostate cancer surgery is common, even after additional salvage radiotherapy. BCR might be explained by target miss. Improved diagnostic accuracy provided by PET could potentially circumvent this therapeutic gap. Therefore, we evaluated consecutive 68Ga-prostate-specific membrane antigen (PSMA) PET/CT, 11C-choline PET/CT, and standard CT imaging in the same patient with regard to TNM-stage migration and accordingly adapted curative radiotherapy options including ablative treatment of oligometastases (n ≤ 5). The cost efficacy of PET- versus CT-based treatment was also calculated. Methods: The prospective register database (064/2013BO1) was retrospectively searched for patients fulfilling the following 3 inclusion criteria: BCR after radical prostatectomy (pT2–pT4 pN0–pN1 cM0, postoperative radiotherapy allowed); 11C-choline PET/CT, 68Ga-PSMA PET/CT, and diagnostic CT performed within 24 h; and available clinical data. Ten treatment routines were defined according to current practice. Furthermore, intention-to-treat and treatment-related costs depending on the shift of TNM stage after imaging were analyzed. Eighty-three patients were eligible (median prostate-specific antigen level, 1.9 ng/mL). Results: Both PET examinations led to concordant results in 72% of patients, whereas the concordance of TNM staging between 68Ga-PSMA PET and diagnostic CT was only 36%. Incorrect staging would lead to “wrong” treatment and therefore to additional costs. A 68Ga-PSMA PET study would be cost-effective if additional costs do not exceed €3,844 ($4,312) (vs. CT). The number needed to image was 2 (for CT) and 4 (for 11C-choline PET) to avoid 1 incorrect treatment. In addition, 68Ga-PSMA PET staging enabled new curative options in half the patients with previous radiotherapy who otherwise receive palliative androgen deprivation therapy. Conclusion: 68Ga-PSMA PET/CT is cost-effective in all patients with regard to avoidance of incorrect treatment. It enabled new curative options for patients with previous radiotherapy who are usually treated palliatively. Therefore, 68Ga-PSMA PET/CT staging should become standard for BCR after surgery with or without radiotherapy.
Biochemical recurrence (BCR) of prostate cancer occurs in 15%–40% of cases after surgery within 5 y (1,2). Standard treatment is salvage radiotherapy (SRT) of the prostatic fossa (3,4), with an estimated freedom-from-biochemical-failure rate of 56% 5 y after SRT (5). Freedom from biochemical failure can be improved by intensification of SRT with androgen deprivation therapy (6,7). However, freedom from biochemical failure does not reach a plateau, as it drops 12 y after SRT to 32%, compared with 54% with additional androgen deprivation therapy. This underlines the limits of recent therapies (7). The efficacy of SRT may be limited if target lesions are missed during radiotherapy. Target miss due to insufficient diagnostic work-up may lead to inadequate definition of the initial prostate bed or regions of positive surgical margins (8) and to untreated microscopic or macroscopic disease distant from the prostatic fossa (N1/M1).
Considering the latter issue, Hellman and Weichselbaum developed the dialectic hypothesis of oligometastases more than 20 y ago, that is, an intermediate state between local and systemic disease with limited tumor burden. Detection of these targets and inclusion into the treated radiotherapy volume during SRT can substantially increase cure rates for local recurrence (LR) and potentially prolong freedom from biochemical failure in cases of detected and treated oligometastases. The problem of missing the target is further aggravated because SRT was usually performed without any imaging at lower prostate-specific antigen (PSA) values (9). PET/CT became an option for staging of recurrent prostate cancer according to international guidelines (10,11), but the reported sensitivity for detection of metastases applying 11C-choline as a radiotracer at PSA levels of less than 1 ng/mL remains low (12). Still, a randomized phase II study recently demonstrated that local treatment of 11C-choline PET–positive oligometastases could postpone progression and the need for systemic treatment (13). New tracers such as 68Ga- or 18F-labeled prostate-specific membrane antigen (PSMA) ligands with more specific binding to prostate cancer cells revealed superior sensitivity and specificity, especially at lower PSA levels (<0.5 ng/mL) (14,15). However, whether new diagnostic options can improve treatment strategies for BCR still needs to be determined (10).
Therefore, we evaluated consecutive 68Ga-PSMA PET/CT, 11C-choline PET/CT, and standard CT imaging in the same patient with regard to TNM-stage migration and accordingly adapted curative radiotherapy options including ablative treatment of oligometastases (n ≤ 5). The intention-to-treat analysis is accompanied by a cost–benefit analysis regarding the costs of incorrect treatment compared with the costs of imaging.
MATERIALS AND METHODS
Patients
Patients underwent PET/CT in a prospective register study at our institution and were retrospectively evaluated. The institutional review board had no objections, and all subjects signed an informed consent form (064/2013BO1). The patients had to fulfil the following 3 inclusion criteria for this analysis: BCR after radical prostatectomy (pT2–pT4 pN0–pN1 cM0, postoperative radiotherapy allowed); subsequent application of 11C-choline and 68Ga-PSMA PET/CT within 24 h combined with diagnostic contrast-enhanced CT (if no contraindications); and availability of clinical data, including Gleason score, PSA level during the course of the disease and before imaging, and pTNM stage at surgery. The time line of procedures is given in Figure 1.
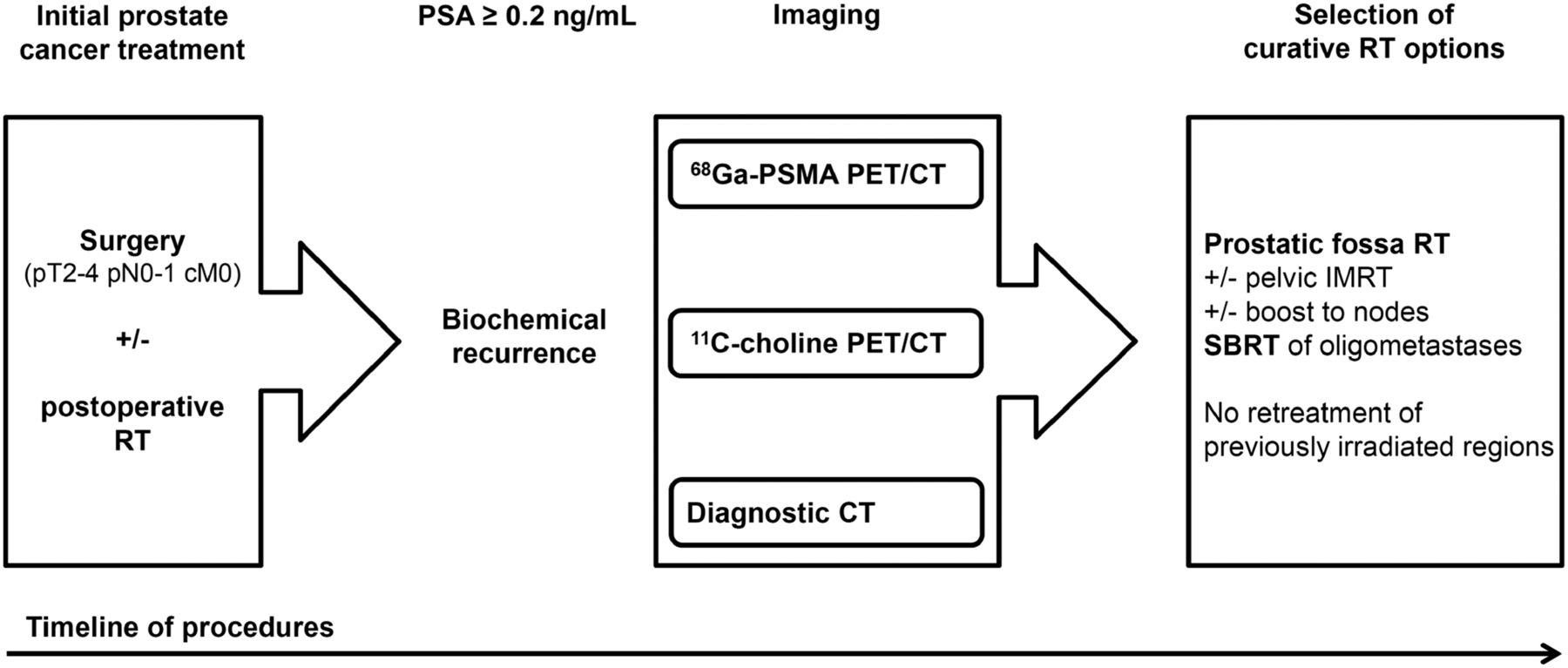
Time line of procedures. RT = radiotherapy.
Imaging Protocol
A PET/CT scan (Biograph mCT; Siemens Healthcare) was acquired 5 min after intravenous administration of a mean dose of 627 ± 25 MBq of 11C-choline combined with a diagnostic CT scan in the venous phase (120 mL of Ultravist 370 [Bayer Healthcare Pharmaceuticals]; flow rate, 2.5 mL/s). Additional late pelvic images were acquired 20 min after injection. On the same day at least 3 h later, a second PET scan was performed using 165 ± 13 MBq of 68Ga-PSMA. If possible, the tracer injection was combined with an injection of 40 mg of furosemide to facilitate micturition before the PET examination. To reduce radiation exposure, a low-dose CT scan was performed for attenuation correction of the 68Ga-PSMA PET data (n = 83). In patients with contraindications to contrast agents, a diagnostic CT scan without contrast medium was performed (n = 4). The examination field ranged from the skull base to the mid thigh. The examination protocol was previously presented in detail by Schwenck et al. (18).
Evaluation
TNM stage was assessed on diagnostic CT by 1 observer masked to PET data, whereas each individual PET examination was analyzed together with diagnostic CT by another investigator taking into account the common practice that either PET/CT or CT staging was performed. However, the PET reader was masked to the results of the PET scan with the other radiotracer. The readers had full knowledge of the clinical history of the patients. Because only patients with radical prostatectomy were included, any mass in the former prostate area was considered suggestive of LR. Suspicious lymph nodes (LNs) were defined on CT as having a short-axis diameter of 10 mm for oval nodes (16) and 8 mm for round nodes (17). In accordance with Schwenck et al. (18), focal uptake above the level of the surrounding background, and not explainable by physiologic processes, was considered suggestive of malignancy. In cases of doubt, additional board-certified specialists were consulted to achieve agreement.
Corresponding to their location, LNs were staged in line with the Prostate Cancer Molecular Imaging Standardized Evaluation criteria (PROMISE) by Eiber et al. either as N1 (pelvic LNs: internal and external iliac, sacral, and obturator) or M1a (extrapelvic LNs: mediastinal, retroperitoneal, and common iliac and inguinal) (19,20). Osteoblastic lesions were considered suggestive of bone metastases on CT (M1b), whereas focal uptake above the level of the surrounding background, and not explainable by physiologic processes, was considered suggestive of bone metastases on PET. Distant metastases in other organs were defined as M1c. According to Bluemel et al., oligometastatic disease was defined as up to 5 metastases in up to 3 organs (21).
Stage-Adapted Treatment Routines and Intention-to-Treat Analysis
Different curative radiotherapeutic options for recurrence after surgery were available depending on previous treatment (surgery ± radiotherapy) and initial nodal stage. To evaluate the impact of different imaging modalities on treatment decisions, stage-dependent treatment routines according to current practice (10,11,13,22) and ongoing phase II studies (23) were developed and an intention-to-treat analysis was performed depending on disease stage after 68Ga-PSMA PET/CT, 11C-choline PET/CT, and standard CT imaging. Treatment of LR or nodal recurrence (NR) was defined as normofractionated radiotherapy with a boost to macroscopic disease. Standard treatment of oligometastases was stereotactic body radiotherapy. Multiple metastases (n > 5) were defined as incurable disease receiving palliative treatment (12). Previous treatment (i.e., previous radiotherapy of prostatic fossa with or without pelvis) reduced the variety of potential treatment options (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org). Examples of curative treatment options and different findings are presented in Figure 2.

Example findings for 68Ga-PSMA PET, 11C-choline PET, CT, and dose distribution of curatively intended image-guided radiotherapy (IGRT) targeted on LR, NR, and oligometastases. LR was correctly identified by both PET tracers but not by CT. NR was detected by 68Ga-PSMA PET (n = 2) and 11C-choline PET (n = 1) but not by CT. Bone metastasis was correctly located on all imaging modalities. For better visualization of NR, radiotherapy plan was rotated by 180° (treatment in prone position).
Statistics, Cost Calculations, and Color Artwork
Descriptive statistics was performed with Excel 2010 (Microsoft Corp.). Treatment costs for radiotherapy regimens were estimated using the German reimbursement catalog (Einheitlicher Bewertungsmaßstab). Medication costs for androgen deprivation therapy were taken from the German medicines compendium (Rote Liste) (24). Color artwork was created using Canvas X (ACD Systems International Inc.).
RESULTS
Study Cohort
From December 2013 to December 2014, 83 patients underwent PET/CT scans with both 68Ga-PSMA and 11C-choline tracer and fulfilled the inclusion criteria for this analysis (Supplemental Table 2). Median patient age was 69.3 y (range, 51–86 y), and the patients had BCR with a median PSA level of 1.9 ng/mL (range, 0.2–33.4 ng/mL) after radical prostatectomy. Most patients (79%) were initially diagnosed with a Gleason score of 7b or higher and advanced disease (≥pT3a). The median time difference between PET examinations and radical prostatectomy was 3.7 y (range, 0.2–21.2 y). Postoperative radiotherapy was applied to the prostatic fossa (n = 33) and to the whole pelvis (n = 11).
TNM Staging by CT and PET Imaging
The T, N, and M stages of the patients were evaluated using 3 imaging modalities (68Ga-PSMA PET/CT, 11C-choline PET/CT, and CT). Previous treatment was used as a covariate potentially influencing the pattern of recurrence. Stages were defined depending on the presence or absence of the TNM parameters, for example, for LR (rT+). In addition, distant metastases were further subdivided into oligo- (n ≤ 5) and multiple metastases (n > 5): LR, NR, oligometastases in distant nodes (M1a), oligometastases in bone (M1b), other oligometastases (M1c), and multiple metastases (n > 5) were differentiated.
The TNM stages according to both PET tracers and CT are presented in Supplemental Table 3: 12%–13% presented with LR, 41%–51% had NR, and 42%–51% had distant metastases. Oligometastases (n ≤ 5) were observed in 71%–79% of all patients with metastases. However, a comparable stage distribution among all imaging modalities was not always associated with equal findings per patient. Upstaging and downstaging per imaging modality occurred in all TNM stages, with predominance in patients without radiotherapy (Supplemental Table 4). In contrast to CT, both PET tracers demonstrated a high concordance in patients after any radiotherapy. Regarding patterns of recurrence, in-field recurrence (LR, NR) in patients after previous pelvic radiotherapy was rare (68Ga-PSMA: 0% LR, 9% NR; 11C-choline: 0% LR,18% NR); that is, recurrence was distributed mainly at distant sites (cM1). Considering the influence of tracers, 11C-choline detected a lower number of NRs than did 68Ga-PSMA (34/42), especially in the group without any radiotherapy (16/23).
TNM-Stage Migration Depending on Imaging and Pretreatment
Because a significantly higher detection rate was demonstrated for 68Ga-PSMA PET/CT by our group (18) and many others, subsequent treatments have been based on 68Ga-PSMA findings with awareness that imaging is not verified by histology. For comparisons with 11C-choline PET/CT and CT imaging, we considered findings after 68Ga-PSMA PET/CT as standard and compared them with each imaging modality, differentiating between consistency and inconsistency in the TNM stage. Results consistent or inconsistent with the defined standard, 68Ga-PSMA PET, were further classified as “correct” or as “wrong” (Fig. 3). For comparison of 11C-choline PET/CT with CT imaging, we applied 11C-choline PET/CT as the standard. In contrast to detection rates (see above) with comparison of LR, NR, or distant metastases, we evaluated patient-based TNM stages further. The 2 PET tracers led to concordant results in 72% (60/83) of patients (Fig. 3A). Concordance between PET tracers further improved with increasing volumes of previous radiotherapy (prostatic fossa, 76%; prostatic fossa and pelvis, 91%) compared with no previous irradiation (64%). The weakest concordance was seen between 68Ga-PSMA PET/CT and standard CT imaging, with correct TNM stages in only 36% (30/83) (Fig. 3B). Similar results were seen for 11C-choline PET/CT compared with CT, with correctness in 40% of cases (33/83) (Fig. 3C).

TNM-stage shifts related to previous radiotherapy and image modality. Comparisons were performed for 68Ga-PSMA PET vs. 11C-choline PET (A), 68Ga-PSMA PET vs. CT (B), and 11C-choline PET vs. CT (C).
Intention-to-Treat Analysis Depending on Imaging Modality
We evaluated whether TNM-stage migration depending on imaging modality was connected to a change in treatment stratification, as these changes might be less frequent in patients after radiotherapy because of the limited curative options. Therefore, we performed an intention-to-treat analysis using the defined algorithms according to Supplemental Table 1. 68Ga-PSMA PET/CT was taken as the standard, and accordingly, the chosen treatments were assigned as the correct treatment. 11C-choline PET/CT was used as the standard for comparison with diagnostic CT. The respective treatment changes are given in Table 1. Among all patients, 69% (57/83) were scheduled for curative and 31% (26/83) for palliative treatment according to 68Ga-PSMA PET/CT. Curative options were available in approximately half the patients with previous radiotherapy and in more than 90% of patients without radiotherapy (Table 1). Correct curative treatment was selected in 72% (41/57) of patients using 11C-choline PET. The use of only CT staging reduced correctness to 33%–39% (19–22/57) compared with both PET tracers. In patients without radiotherapy, palliative treatment was in no case correctly chosen by CT according to 68Ga-PSMA PET. Regarding all patients, CT staging led to correct palliative treatment in 42% (11/26), consistent with 68Ga-PSMA.
Correctness of Curative and Palliative Treatment Recommendation According to Findings of 68Ga-PSMA, 11C-Choline PET, and Contrast-Enhanced CT
The wrong choice of curative treatment—one inconsistent with 68Ga-PSMA (i.e., curative treatment in cases of 68Ga-PSMA PET–detected palliative situations)—was selected mostly in patients after prostatic fossa radiotherapy (CT, 27% [9/33]; 11C-choline, 15% [5/33]). Wrong palliative treatment was defined as either palliative treatment in cases of a curative situation or selection of the wrong curative radiotherapy schedule, leading to insufficient and therefore a palliative outcome. Wrong palliative treatment was frequently chosen with consideration of the CT results in patients without previous radiotherapy (59% [23/39]).
Cost–Benefit Analysis Focusing on Costs of Wrong Treatment
In general, wrong treatment was usually associated with initiation of another (hopefully correct) therapy. Here, we assume that the more precise diagnostic procedure using 68Ga-PSMA leads to a better (i.e., correct) treatment. Of course, solid criteria such as overall survival need to be investigated in the future. To estimate the additional costs of a wrong treatment we used calculations from the German reimbursement catalog. Supplemental Table 5 presents the estimated costs according to this catalog, depending on the chosen radiotherapy routine. Selection of the former standard tracer, 11C-choline, would lead to additional costs of €108,510.24 ($121,721.64) per 83 patients. Regarding costs avoided by use of the correct 68Ga-PSMA PET/CT–directed treatment, a 68Ga-PSMA PET/CT study would be cost-effective if the additional costs, compared with a 11C-choline PET/CT study, do not exceed €1,307 ($1,466) per examination. CT-standard staging would result in additional costs of €319,034.88 ($357,878.97) per 83 patients. Considering the costs avoided by use of the correct 68Ga-PSMA PET/CT–directed treatment, a 68Ga-PSMA PET/CT study would be cost-effective if the additional costs, compared with a standard CT study, do not exceed €3,844 ($4.312) per examination.
Qualitative Analysis of Shifts to Cure or Palliation
To define the clinical benefits and disadvantages of CT or PET staging, we evaluated different findings and clinical scenarios. Patients with a wrong palliative treatment instead of a correct curative treatment might also have a palliative outcome, not least because of target miss or underdosing. If 68Ga-PSMA PET/CT is used, 26 of 83 patients will be correctly treated palliatively, compared with 41 of 83 (11C-choline PET/CT) and 64 of 83 (CT) patients if the other modalities are used. Altogether, potentially curative chances were reduced from 57 (100%, 68Ga-PSMA) to 42 (74%, 11C-choline) to 19 (33%, CT) patients. According to the “number needed to treat” (25) we calculated the “number needed to image” (NNI) to avoid 1 wrong treatment for a patient. The calculated NNI for 11C-choline was 4, whereas that for contrast-enhanced CT was 2, compared with 68Ga-PSMA PET.
DISCUSSION
In this analysis, we compared the impact of 3 simultaneously performed imaging modalities (68Ga-PSMA PET, 11C-choline PET, and contrast-enhanced CT) on TNM-stage migration and accordingly adapted curative radiotherapy options including ablative treatment of oligometastases (n ≤ 5) for BCR after surgery.
The main findings include the cost efficacy of 68Ga-PSMA PET by calculating the additional costs of wrong intended treatment occurring in approximately 2 of 3 patients after conventional CT staging. In addition, we were able to demonstrate that 68Ga-PSMA PET gave a high chance of curative treatment for patients without previous radiotherapy (>90%) and new curative options in patients after previous radiotherapy, who usually would otherwise receive palliative androgen deprivation therapy. The detection of macroscopic lesions after radiotherapy opened a third curative chance in half the patients (i.e., after surgery and radiotherapy): either radiotherapy of pelvic nodes or stereotactic body radiotherapy of oligometastases.
In contrast to other publications, we performed a stage-based comparison instead of a lesion-based comparison because TNM stage with differentiation of M1 disease in oligo- or multiple metastases is used to define treatment recommendations. The study cohort reflects a typical clinical situation of patients being admitted for additional staging examinations (median pT3a, median Gleason score of 7b, and median PSA level of 1.9 ng/mL) to avoid wrong treatment or overtreatment (26).
Standard staging after BCR is not routinely recommended (10,11). CT imaging in this series detected only one third of the lesions, in contrast to more than 70% of detected lesions with 11C-choline PET/CT, compared with the chosen standard, 68Ga-PSMA PET/CT (18). This finding is in line with some other series, which reported stage changes ranging from 33% to 67% by 68Ga-PSMA PET (26–31). 11C-choline–related stage and treatment changes were in the same range, at 41%–55% (32–34). The number of stage shifts in this series was in the upper range of the mentioned studies, because we defined a higher number of metastases (n = 5) as oligometastatic disease than did other studies (n = 1–3 metastases) (35). However, we decided to use a cutoff of 5 oligometastases (M1a–M1c) because nonregional nodes (M1a) are not counted in current definitions as oligometastases (CHAARTED criteria) (36). Two patients in this series presented with 4–5 bone metastases according to CHAARTED (i.e., high-volume criterion).
Furthermore, the number of stage changes and consecutive treatment adaptions depending on risk group and previous treatment are not well defined. No curative recommendations exist, especially for patients who undergo radical prostatectomy followed by any postoperative radiotherapy and then present with subsequent PSA progress. This lack underlines the need to evaluate the influence of imaging on therapeutic decision making in these subgroups.
The chosen curative radiotherapy options were defined according to current guidelines (10,11) or current practice (13,22,23). However, sometimes more than one option for local treatment might be available, such as surgery and the addition of androgen deprivation therapy (37). We focused on image-guided radiotherapy because of the advantage of treating more lesions in different regions simultaneously using hybrid imaging for treatment planning. The definition of 5 oligometastases as the threshold for curative treatment needs further prospective evaluation. In addition, palliative treatment might be the preferred choice, especially for elderly or frail patients. Therefore, the defined routines incorporating the concept of oligometastases reflect the best radiotherapy scenario for fit patients with a longer life expectancy. In many tumor entities, including prostate cancer, local treatment of oligometastases prolonged the PFS of 2–5 y for about 20% of patients (38).
Patients without previous radiotherapy may benefit from 68Ga-PSMA PET/CT imaging, considering the 90% chance to receive a curative approach. Using the other staging methods, selection of curative treatment was reduced to around 70% (11C-choline) and 33% (CT). Therapeutic decisions for SRT are made mostly without additional imaging, except for the planning CT (without contrast medium). Because undetected metastases are not treated in these cases (target miss), the impressive difference of approximately 60% between CT and PET imaging to treat patients with curative intent could explain why SRT is less effective at higher PSA levels (5).
In patients after previous radiotherapy, palliative treatment is the standard of care (10,11). Here, the pattern of recurrence after radiotherapy of the prostatic fossa was mainly NR and distant. After pelvic radiotherapy, almost all patients experienced distant relapse. Regarding the pattern of relapse, the higher concordance rates for imaging after previous radiotherapy might be related to improved local control of micrometastases in treated areas and to a lower number of treatment options after previous radiotherapy, that is, no in-field retreatment (Supplemental Table 3). Oligometastases (cM1a–cM1c) were present after any radiotherapy in approximately two thirds of patients with metastases, underlining the value of 68Ga-PSMA PET/CT for detection of this intermediate oligo-stage (Supplemental Table 3). This capability offered the possibility of a third curative treatment (after surgery and radiotherapy) in around 50% of these patients.
Any wrong treatment leads either to overtreatment (wrong curative) or to wrong palliative radiotherapy with an insufficient outcome caused by missing the target or delivering an inadequate dose to undetected lesions. In this study, overtreatment was associated with not covering all target lesions; for example, the chosen curative radiotherapy treated the prostatic fossa, but the affected LNs or distant metastases were not covered. Overtreatment of palliative-treatment patients occurred in 58% and 27% of the patients with CT and 11C-choline staging, compared with standard 68Ga-PSMA PET/CT. Inadequate palliative treatment of patients with curative options occurred in 67% with CT staging and in 28% with 11C-choline staging leading to a palliative outcome.
The cost–benefit analysis demonstrated a clear cost efficacy for hybrid imaging, according to the German reimbursement catalog. This benefit might not be present if calculated costs for PET are higher or costs of radiotherapy are much lower. Therefore, we calculated an independent measure for efficacy. We exploited the clinical tool “number needed to treat” as NNI to avoid 1 wrong treatment for a patient (25,39). The NNI for 11C-choline was 4, and the NNI for contrast-enhanced CT was 2, compared with 68Ga-PSMA PET. Both values underline the high efficacy of 68Ga-PSMA PET/CT.
Limitations of our study comprise the heterogeneous patient cohort, absence of histology for ethical reasons, and the retrospective approach leading to treatment management decisions. Objective and reproducible image interpretation is always challenging. Masked image evaluation was performed for CT, and the PET reader was masked to the results of the PET/CT scan with the other radiotracer. In addition, high reproducibility for 68Ga-PSMA and 11C-choline PET/CT image interpretation had already been demonstrated by high interobserver agreement (40,41). Because of the large number and overlap of risk factors, we could not calculate biochemical or survival endpoints for these 30 clinical scenarios that could be further individualized by personalized treatment concepts (42). Nevertheless, a comprehensive study on the influence of 68Ga-PSMA PET/CT on overall survival is still lacking, but our analysis is strengthening the evidence that the use 68Ga-PSMA PET/CT heavily influences treatment decisions. Ongoing clinical studies will evaluate 68Ga-PSMA or 11C-choline PET–directed treatment of oligo-recurrences (NCT03569241 [PEACE V]).
CONCLUSION
By using a TNM stage–based analysis and treatment stratification, we were able to demonstrate a great potential benefit for 68Ga-PSMA PET/CT in the staging of postprostatectomy recurrence. We introduced a measure of treatment efficacy (NNI with 68Ga-PSMA PET to avoid 1 wrong treatment) and could show that 68Ga-PSMA PET/CT is cost-effective when used in prostate cancer patients with BCR. In addition, 68Ga-PSMA PET/CT enables new curative treatment options, especially for patients after previous radiotherapy who are usually treated palliatively. Therefore, 68Ga-PSMA PET/CT should become the standard method for staging high-risk prostate cancer patients with BCR after surgery with or without radiotherapy.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
KEY POINTS
QUESTION: How does treatment change depend on findings in PSMA PET/CT, choline PET/CT, and CT for prostate cancer recurrences after surgery?
PERTINENT FINDINGS: Both PET examinations led to concordant results in 72% of patients, while concordance of TNM staging between PSMA PET/CT and diagnostic CT was only 36% in this register study. PSMA PET staging was cost-effective and enabled new curative options in half of the patients with previous RT who otherwise receive palliative ADT.
IMPLICATIONS FOR PATIENT CARE: PSMA PET/CT staging should become standard in staging of high-risk prostate cancer patients with BCR after surgery ± RT.
Acknowledgments
We acknowledge the assistance of Elizabeth Krämer in proofreading the manuscript.
Footnotes
Published online Mar. 8, 2019.
- © 2019 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 9, 2018.
- Accepted for publication February 11, 2019.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.