


Abstract
Assessment of cardiac 123I-meta iodobenzylguanidine (123I-mIBG) uptake relies on the heart-to-mediastinum ratio (HMR) derived from planar images. We have developed novel semiautomated quantitative methodologies for assessing HMR from SPECT images using a dedicated cardiac multipinhole SPECT/CT system and determined the lower limit of normal (LLN) SPECT-derived HMR and the correlation to planar-derived HMR. Methods: Twenty-one healthy volunteers were injected with 123I-mIBG and imaged using 2 different cameras. Planar images were acquired using a conventional SPECT camera equipped with parallel hole collimators, and hybrid SPECT/CT images were acquired using a dedicated cardiac SPECT system with 19 pinhole collimators interfaced with 64-slice CT. Planar HMR was calculated as per standard guidelines (manual traditional method) and elliptic region-of-interest (Elip-ROI) and region-growing (RG-ROI) techniques. SPECT HMR was quantified using a new method that incorporates various cardiac and mediastinal segmentation schemes in which upper and lower limits of the heart were determined from CT and the left ventricular ROI, and mean counts were calculated using Elip-ROI and RG-ROI techniques. Mean counts in mediastinal ROI were computed from a fixed volume in 3 different regions: upper mediastinum (UM), lower mediastinum (LM), and contralateral lung (CL). HMRs were processed by 2 observers, and reproducibility was assessed by intraclass correlation coefficient and Bland–Altman analysis. Results: Planar HMR calculated using the RG-ROI method showed highest intra- and interobserver levels of agreement compared with Elip-ROI and manual traditional methods. SPECT HMR calculated on the basis of UM, LM, and CL background regions showed excellent intra- and interobserver agreement. SPECT HMR with UM resulted in highest correlation (R = 0.91) with planar HMR compared with that with LM (R = 0.74) and CL (R = 0.73). The LLN of SPECT HMR with UM and that of planar HMR was calculated as 5.5 and 1.6, respectively. The normal values of SPECT-derived HMR and planar-derived HMR were correlated linearly. Conclusion: We reconfirmed the previous planar HMR threshold and determined SPECT LLN HMR for SPECT. Planar HMR can be estimated from SPECT HMR via a simple linear regression equation, allowing use of the new cardiac-dedicated SPECT camera for 123I-mIBG imaging.
Reduced myocardial sympathetic innervation is a prominent feature of heart failure (HF) due to posttranscriptional downregulation of the cardiac norepinephrine transporter (1–3). Myocardial imaging with 123I-meta iodobenzylguanidine (123I-mIBG), an analog of norepinephrine, is recognized as a useful tool for risk stratification of HF patients with reduced ejection fraction (1–7) and has been studied as a potential identifier of patients with increased risk for ventricular arrhythmic events (4,6,8–13). Previously published data have demonstrated that clinical utility of quantifying the heart-to-mediastinum ratio (HMR) and washout ratio (WR) from planar radionuclide images to assess myocardial 123I-mIBG uptake provides a risk assessment of major adverse cardiac events and mortality (1–13). A low HMR value on delayed (3 h posttracer injection) images has been shown to be an independent predictor of ventricular tachyarrhythmia (14,15), appropriate implantable cardioverter defibrillator therapy (16,17), and sudden cardiac death (18) in HF patients. Moreover, an increased myocardial washout of 123I-mIBG has been associated with poor prognosis (7). The ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure), a multicenter prospective trial of subjects with New York Heart Association II and III HF and left ventricular (LV) function of 35% or less, revealed an association of lower HMR of 123I-mIBG uptake with higher 2-y incidence of cardiac events (19). In the ADMIRE-HF study, an HMR threshold of 1.6 derived from planar 123I-mIBG images was used to dichotomize high- and low-risk patients based on the incidence of cardiac events. However, normal limits of HMRs derived from 123I-mIBG SPECT images have not been extensively investigated.
Despite the proven prognostic value of 123I-mIBG in patients with HF, there remain limitations to the use of 123I-mIBG imaging (4). One of the common limitations is the variation among different methods used for HMR and WR quantifications. This variation can be caused by image acquisition time and duration, location, and size of the heart and mediastinal region of interest (ROI) (13,20,21) as well as the level of expertise and experience for WR calculation (22). Additionally, SPECT 123I-mIBG quantification is technically challenging because of the regional variation of myocardial 123I-mIBG uptake, potential artifacts related to radioactivity in adjacent lung and liver areas, and reduced global 123I-mIBG uptake that is commonly observed in patients with severe systolic dysfunction (23). Although cardiac-dedicated SPECT cameras with solid-state detectors and multipinhole collimators provide superior 3-dimensional (3D) image resolution in the small cardiac ROI, these imaging devices are not capable of acquiring traditional 2-dimensional planar images due to the nonconventional geometry and magnification of multipinhole collimation, limiting the use of these new imaging devices for 123I-mIBG imaging.
The purpose of this study was to develop novel semiautomated quantitative methodology for 123I-mIBG HMR quantification using a dedicated cardiac SPECT/CT camera equipped with solid-state detectors and pinhole collimators and compare SPECT-derived HMR to traditional planar-derived HMR in a cohort of normal patients. In addition, we sought to assess the reliability of planar and SPECT 123I-mIBG quantifications using traditional as well as automated software and determine the lower limits of normal (LLNs) SPECT-derived 123I-mIBG HMRs from normal subjects.
MATERIALS AND METHODS
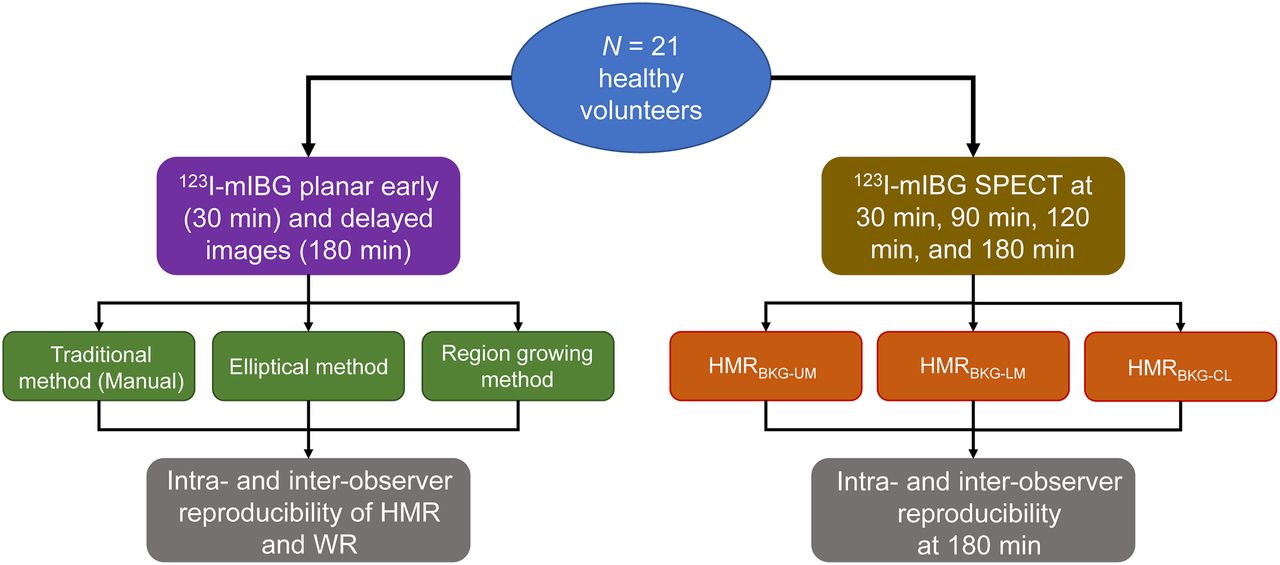
After the approval of the Institutional Review Board, we enrolled 21 healthy normal volunteers (10 men and 11 women) between the ages of 32 and 64 y (48 ± 12 y) with mean body mass index of 26.3 ± 4.9 kg/m2. All subjects signed a written informed consent form. Subjects who were pregnant or with cognitive impairment, any heart disease, or other significant illness or medications that could influence the sympathetic activity of the heart were excluded from this study. All subjects had a normal baseline 12-lead electrocardiogram and were injected with 123I-mIBG (209 ± 44 MBq; AdreView [GE Healthcare]) after administration of Lugol’s solution (100 mg). Planar and SPECT/CT images were acquired for all subjects (Fig. 1).
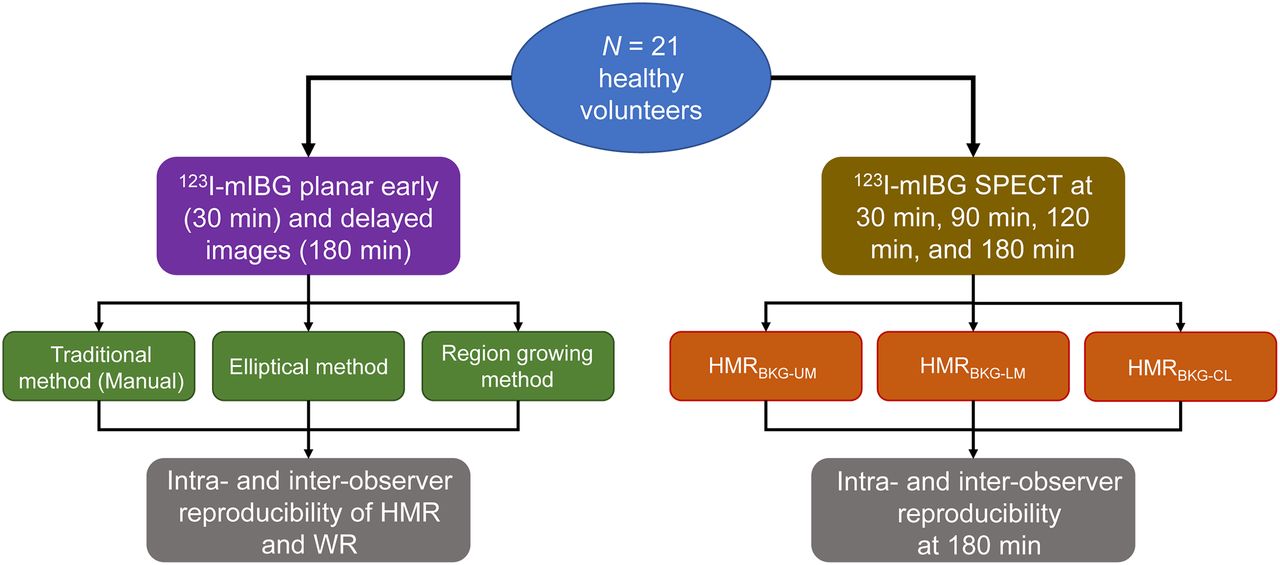
Flowchart of patient study, 123I-mIBG planar and SPECT imaging, and data analyses.
Planar MIBG Image Acquisition and Analysis
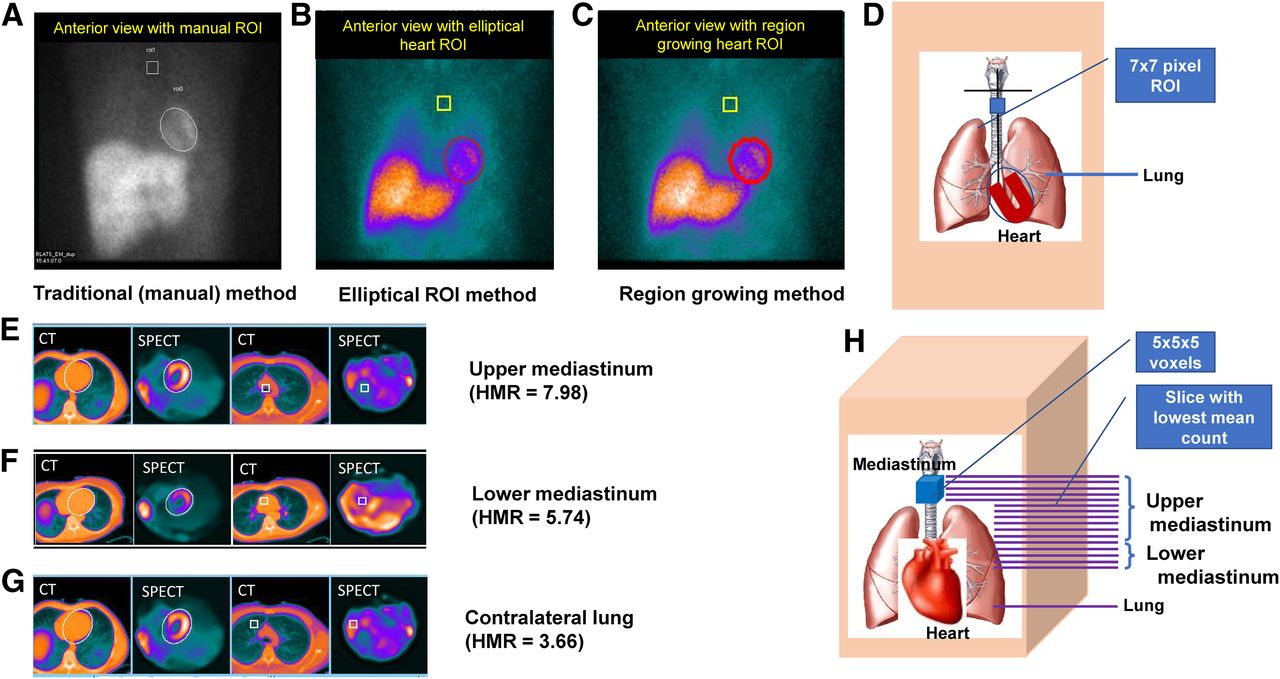
Planar images with a 128 × 128 matrix and 3.3 × 3.3 mm2 pixel size were acquired at 30 min (early images) and 180 min (late or delayed images) after 123I-mIBG injection, with the patient supine, for 10 min using a dual-head SPECT system equipped with low-energy high-resolution collimators (Infinia; GE Healthcare). HMR was assessed with 3 different methods. For the first method, as per the Adreview package insert (traditional method), HMR was calculated from planar 123I-mIBG images on which heart and mediastinal ROIs were manually drawn using XELERIS postprocessing software (Infinia; GE Healthcare). The heart ROI was determined by the epicardial border visualized using the medial aspect of lower part of the lungs for an anatomic guidance. The lung apices were visually estimated using a horizontal line intersected by the vertical line equidistant from the medial aspects of upper part of the lungs. A square ROI of 7 × 7 pixels was centered and drawn at the location with the lowest count visualized along the vertical line below the horizontal line intersection (Fig. 2). For the second method (elliptic ROI method), HMR was calculated using the Yale Cardiac Quantification (Yale-CQ) software in which an initial elliptic ROI was placed over the heart and the elliptic ROI was adjusted in length, width, and axial angle to visually fit the heart region using a user graphical interface, and a square ROI of 7 × 7 pixels was centered and drawn at the location with the lowest counts along 12 pixels of the vertical line starting at 4 pixels below the horizontal line intersection. For the third method (region growing), the heart ROI was further refined and recalculated using a region-growing algorithm developed at Yale. For the mediastinal ROI, a horizontal line was placed on the lung apices, and a box of 7 × 7 pixels was automatically determined by the Yale-CQ software. Using the above 3 methods for determination of the heart and mediastinal ROIs, HMR was calculated by dividing the mean count (counts/pixel) in the heart ROI by that in the mediastinal ROI (Figs. 1 and 2A–2D).
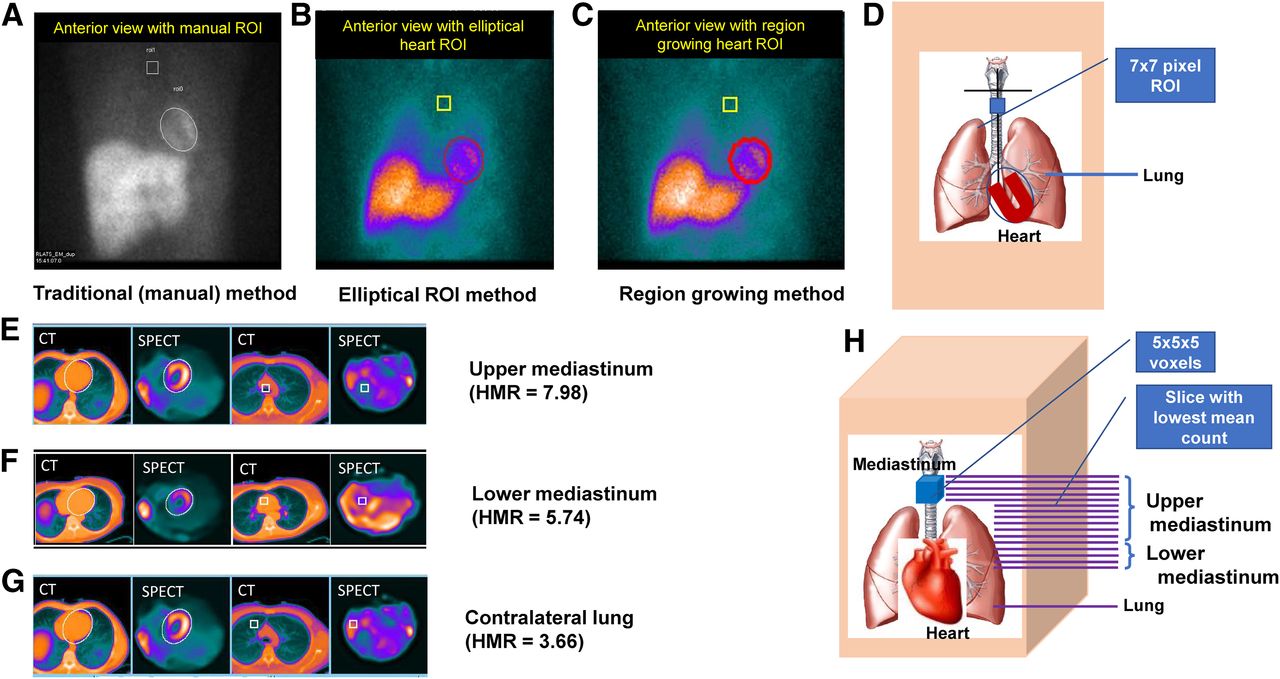
Planar-HMR quantification methods: planar images with heart and mediastinal ROIs (A–C) and schematics showing relative positions of heart and mediastinal regions in 2D (D). SPECT HMR quantification methods from fused SPECT/CT images: coregistered central SPECT and CT slices of heart and mediastinal regions (E–G) and schematics showing relative positions of heart and 2 different mediastinal regions in 3D (H).
123I-mIBG WR was calculated from early and late (delayed) planar images without background correction, WR (%) = (He-Hl)/He × 100, and with background correction, WRBKG-corrected (%) = [(He-Me) − (Hl-Ml)]/(He-Me) × 100, where H represents the mean count from the heart ROI and M denotes the mean count in the mediastinal ROI for early (e) and late (l) 123I-mIBG planar images (24).
SPECT 123I-mIBG Image Acquisition and Analysis
SPECT raw images with a 32 × 32 matrix and 2.5 × 2.5 mm2 pixel size were acquired for 15 min at 30, 90, 120, and 180 min after 123I-mIBG tracer injection using a stationary cardiac-dedicated hybrid SPECT/CT scanner equipped with cadmium zinc telluride (CZT) detectors and 19 tungsten pinhole collimators (Discovery NM/CT 570c; GE Healthcare). A noncontrast CT scan used for SPECT attenuation correction was acquired with 120 kVp, 50 mA, a pitch of 0.984, a slice thickness of 2.5 mm, and a rotation speed of 0.4 s and was reconstructed using filtered backprojection with a voxel size of 0.977 mm3. SPECT images were reconstructed with a matrix size of 70 × 70 and pixel size of 3.2 × 3.2 mm2 using the maximum-likelihood expectation maximization algorithm incorporated with the CT-based attenuation correction. For SPECT-derived HMR quantification, the upper and lower limits of the heart were determined by the central tranaxial slice of CT images coregistered with SPECT, and the ROI of the LV myocardium was automatically segmented using a previously published bimodal median threshold algorithm (25,26). Mean counts in the LV myocardium were calculated from the LV regions segmented, and background mean counts were calculated from 3 different regions (upper mediastinum [UM], lower mediastinum [LM], and contralateral lung [CL]) each with a fixed volume of 5 × 5 × 5 voxels manually defined (Figs. 1 and 2E–2H).
Reproducibility of HMR Quantification
Analyses of intra- and interobserver agreements were performed to evaluate the reproducibility of HMR and WR quantifications. Intraobserver variability was assessed by a single operator (A), who processed all images twice with 4 wk apart to avoid recall bias. For interobserver variability, the images were processed independently by 2 different operators (A and B). The LLN was calculated by mean – 2 × SD.
Statistical Analysis
All statistical analyses were performed using Microsoft Excel and SPSS (Statistical Package for the Social Sciences) software. Continuous variables were expressed as mean ± SD. Paired t test and 1-way ANOVA were used for comparisons among variables. Quantification performed by different operators were compared using the linear regression equation and correlation analysis. Intraclass correlation coefficient (ICC) was calculated to assess the reliability measure with the ICC being classified as poor, fair, good, and excellent based on values of less than 0.49, 0.49 to 0.59, 0.60 to 0.74, and greater than 0.74, respectively (27). Bland–Altman plots were used to assess agreements between the quantified data (28).
RESULTS
Planar HMR quantified using the region-growing method resulted in highest intraobserver (Table 1; Supplemental Figs. 1 and 2 [supplemental materials are available at http://jnm.snmjournals.org]) and interobserver (Table 1; Supplemental Figs. 3 and 4) reproducibilities as compared with elliptic ROI and traditional manual methods. There was no significant difference among mean WRs calculated using the 3 methods. However, WRs obtained from the region-growing method were more reproducible and precise (more repeatable) than those obtained from the elliptic ROI method and traditional methods in terms of intra- (ICC = 0.94) and interobserver (ICC = 0.96) variabilities (Table 2). For all 3 methods, WRs without background correction were more reproducible and precise than those with background correction (Table 2; Supplemental Figs. 5 and 6). The LLN of HMR derived from planar images using the 3 methods above ranged from 1.56 to 1.64.
Early and Delayed Planar HMR for Intra- and Interobserver Analysis
Washout Rates for Intra- and Interobserver Analysis
SPECT HMRs calculated on the basis of the upper mediastinum (HMRBKG-UM), lower mediastinum (HMRBKG-LM), and contralateral lung (HMRBKG-CL) background regions showed excellent intra- and interagreements (Table 3; Supplemental Fig. 7). However, HMR calculated using the UM background resulted in highest linear correlation with region-growing ROI planar HMR (R = 0.91) compared with those calculated using the LM (R = 0.74) and CL background (R = 0.73) as shown in Figure 3. The LLN of the HMR derived from HMRBKG-UM was higher than those derived from HMRBKG-LM and HMRBKG-CL (Table 3). Table 4 shows the mean HMRBKG-UM and LLN processed by observer A1 at 4 different tracer injection times (t = 30, 90, 120, and 180 min). As seen, SPECT-derived HMR and LLN increased as a function of the SPECT imaging time. Paired HMR comparisons between 120, 90, and 30 min versus 180 min are shown in Figure 4. The correlation between HMR at 120 min and HMR at 180 min was highest among these 3 paired comparisons. The difference between HMRs at 120 and 180 min was not significantly different, and LLNs at 120 and 180 min were similar (5.1 and 5.6, respectively). The normal values of SPECT-derived HMR and planar-derived HMR were linearly correlated by y = 3.77 × −0.21, where y = SPECT-derived HMR and x = planar-derived HMR.
SPECT HMR and Intra- and Interobserver Analysis

Correlations between planar HMR quantified using region-growing ROI and SPECT HMRs calculated on basis of 3 background (BKG) regions: HMRBKG-LM (A), HMRBKG-CL (B), and HMRBKG-UM (C), and correlation between planar and SPECT mean counts in heart ROI (D).
LLN for SPECT HMRBKG-UM

Correlations of SPECT HMRBKG-UM at 180 min versus (A) 120 min, (B) 90 min, and (C) 30 min, after 123I-mIBG injection.
DISCUSSION
We have reported herein the quantification reproducibility and precision of 123I-mIBG myocardial uptake from planar and SPECT images using traditional methods and the semiautomated Yale approach. In the normal low-risk population, we have determined the normal limits of myocardial 123I-mIBG uptake from planar and SPECT images and established a linear correlation between the planar and SPECT HMRs determined using various 123I-mIBG quantification methods. The present study also demonstrated that the intra- and interobserver reproducibilities for the 123I-mIBG image quantifications were excellent.
Although we have presented various unique approaches to the quantification of 123I-mIBG myocardial uptake, substantial efforts had been made by others to standardize the methods for HMR quantification from 123I-mIBG myocardial scintigraphy. For planar mIBG imaging, most previous investigators used traditional manual methods similar to those we used for HMR quantification (8,22,23,29). Although planar images are comparatively easier to acquire and quantify, SPECT imaging for 123I-mIBG has considerable benefits because of its potential to evaluate regional heterogeneities of the myocardial mIBG uptake above and beyond the HMR and WR assessments. Moreover, with SPECT imaging superimposition of the anatomic structures seen in 2-dimensional planar images (e.g., lungs overlapping the heart) can be minimized and identification of the heart limits in 3D is feasible, leading to more accurate quantification (a measurement close to the true value). For SPECT 123I-mIBG quantification, several different methods have been reported. Van der Veen et al. assessed cardiac innervation using volumetric quantification of 123I-mIBG with planar and SPECT acquisitions in 54 patients referred for imaging before placement of an implantable cardioverter defibrillator. In that study, 123I-mIBG SPECT HMR was derived from an automated system using midventricular-short-axis and vertical- and horizontal-long-axis SPECT slices to create 3D volume of interest for the heart and mediastinum regions (29). Another study by Bellevre et al. reported 123I-MIBG HMR quantification using a CZT-based camera (D-SPECT; SPECTRUM Dynamic Medical) with a dual-isotope protocol (123I and 99mTc) and compared the HMR with that quantified from the conventional planar images, which were acquired using an Anger-SPECT camera with low-energy and high-resolution collimators. The planar HMR was quantified using the traditional method by drawing the ROI manually on the LV and over the UM area, and SPECT 123I-MIBG HMR was quantified using the same ROI drawn on the 99mTc SPECT images (30). In our study, however, we used the traditional method as well as the semiquantitative methods for planar HMR calculation and compared the results with the SPECT HMRs obtained by incorporating the SPECT and CT image coregistration. In addition, there were 3 other reports that assessed the cardiac sympathetic denervation based on the mismatch score of 123I-mIBG and 99mTc-labeled perfusion images using a severity measure on the standard 17-segment model (8,23,31). In our study, the planar images were acquired using a dual-head SPECT system with low-energy high-resolution collimators. Although the HMR values can be varied by different types of collimators and imaging systems used, Nakajima et al. have demonstrated that standardization of HMR using a cardiac calibration phantom method is feasible (32).
In the present study, we used semiautomated software involving the placement of an automatically adjustable elliptic-shaped ROI around the heart using the region-growing method. An alternative semiautomated elliptic ROI method was also introduced in this report for HMR quantification, although this approach was found to be inferior to the region-growing method in terms of reproducibility and precision, presumably due to the variability in the ROI placement using the elliptic method. More specifically, unlike the averaged mediastinum ROI counts, the elliptic-shaped ROI being placed around the heart can be variable in width and shape, as well as angular placement, and therefore somewhat operator dependent (27). However, this variability can be reduced by the region-growing method, which automatically adjusts the elliptic ROI around the heart using a heuristic region-growing algorithm, thereby minimizing intra- and interobserver variabilities. In comparison, the traditional manual method is highly operator-dependent and is less reliable and reproducible than both automated methods (elliptic ROI and region-growing ROI). These findings were further confirmed by the ICCs and Bland–Altman analyses in this report. More specifically, the ICC, a measure of reliability, was highest using the region-growing ROI method as compared with the elliptic ROI and traditional methods.
For SPECT HMR quantification, all the 3 ROI methods showed excellent intra- and interobserver reproducibility, and reliability as indicated by ICC greater than 0.90 for all 3 methods, and by the narrow limits of agreement defined by Bland–Altman analysis. These results were somewhat expected, however, because all these 3 methods were implemented in an automated manner, in which HMR was calculated with a minimal user interaction with the software. In this study, the SPECT region-growing ROI method using the UM location for calculations of the background and SPECT HMR resulted in the strongest linear correlation with planar HMR. Lower correlations between planar HMR and SPECT HMR were observed when the LM or CL was used as background in the HMR calculation (Figs. 3A–3C). This difference was attributed to the variation of the mean counts calculated from these 3 background ROIs. The best correlation between the planar-derived and SPECT-derived HMRs was noticed when the UM ROI was used for background (Fig. 3C). Also, as seen in Figure 3D, there was a strong linear correlation between the SPECT and planar mean counts from the heart ROI, which was not affected by the background. The variation of the mean counts calculated from the background ROIs mentioned above usually exists but may be more modest for CZT SPECT cameras with limited field of view. This background variation may in turn lead to the reduction of ICC for WR (Table 2). In the present study, we selected the most upper SPECT slices near the UM region that could be reliably reconstructed by the CZT SPECT so that a good correlation between the planar and SPECT HMR was feasible. However, the UM region we used for SPECT HMR calculation may not be the same region commonly used for planar HMR calculation.
The LLN HMR (1.56–1.64) derived from the planar images in this study was consistent with the previous HMR cutoff of 1.6 proposed by Jacobson et al. (4) for optimal risk stratification of HF patients. For SPECT images, the HMR LLN calculated with the UM ROI was higher than those with the LM or CL ROIs (Table 3). This HMR difference can be attributable to the increased mean counts from the background structures in the LM or CL ROIs. As demonstrated in this study, the SPECT-derived HMR that incorporated the UM background ROI and region-growing ROI method provided the highest correlation with the planar-derived HMR along with best reproducibility and reliability. Thus, it may be feasible to estimate the normal values of SPECT-derived HMR from planar-derived HMR or vice versa via the linear regression equation (SPECT_HMR = 3.77 × planar_HMR − 0.21) established in the present study.
The application of myocardial 123I-mIBG SPECT imaging in the risk stratification of patients with ischemic heart disease has been focused on the detection of sympathetic innervation based on the calculation of HMR or WR. Although a strong association between regional innervation abnormality and susceptibility to arrhythmias has been demonstrated particularly in the ischemic setting (10,12,19,33,34), further studies are needed to evaluate the utility of SPECT-based HMR value in predicting future cardiac arrhythmic events. In the current study, we have introduced a new semiautomated method for reproducible quantification of 123I-mIBG HMR and WR from planar and SPECT images. Our results showed a linear relationship between planar and SPECT HMR values, indicating the feasibility of estimating the normal values of SPECT-derived parameters from planar images or vice versa. However, this study cohort comprised evaluation of all normal healthy volunteers; hence, further validation in abnormal individuals is warranted in future investigation.
CONCLUSION
The quantification of 123I-mIBG HMR and WR from SPECT images using the semiautomated methods was extremely reproducible and precise. The LLN HMRs quantified from SPECT and planar images were derived using normal volunteers. The LLN of planar HMR was consistent with the HMR cutoff used for the risk stratification in the ADMIRE-HF study. The LLN HMR quantified from SPECT images is greater than that from planar images. It may be feasible to translate 123I mIBG HMR values from SPECT into a value for conventional planar HMR value via a simple linear equation.
DISCLOSURE
This work was supported in part by an Investigator Initiated Trial Grant from GE Healthcare, Inc., and a Grant-in-Aid research grant from the American Heart Association (14GRNT19040010). No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Vera Tsatkin, Ramesh Fazzone-Chettiar, and Stephanie Thorn, PhD, for their technical assistance in this study. This research was presented in part at the Annual Meeting of American College of Cardiology April 2–4, 2016 (ACC 2016), Chicago, Illinois.
Footnotes
Published online Sep. 15, 2017.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 7, 2017.
- Accepted for publication August 30, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.