


Abstract
Biochemical recurrence (BCR) is a concern for prostate cancer patients after local treatment. 68Ga-labeled prostate-specific membrane antigen (PSMA) ligands have significantly improved prostate cancer imaging. However, several 18F-labeled ligands that were developed as fluorinated tracers might present advantages. In this study, we analyzed the potential of 18F-PSMA-1007 in patients with BCR. Methods: Twelve patients with BCR after local treatment underwent PET/CT scans 1 and 3 h after injection of 18F-PSMA-1007. Results: 18F-PSMA-1007 PET/CT detected lesions in 9 of 12 patients (75%). A significant difference was observed when comparing the tracer uptake in 18F-PSMA-1007–positive lesions 1 and 3 h after injection (median SUVmax, 7.00 vs. 11.34; P < 0.001; n = 76). Forty-four (88%) of 50 18F-PSMA-1007–positive lymph nodes had a short-axis diameter of less than 8 mm. Conclusion: In this pilot study, 18F-PSMA-1007 PET/CT presented high potential for localization of recurrent disease in prostate cancer patients with BCR.
Biochemical recurrence (BCR) represents a concern for patients after initial curative treatment of prostate cancer. Early detection of recurrent disease is important, to be able to offer a salvage therapy with curative intent. However, in the setting of BCR, full-body bone scans and cross-sectional abdominopelvic CT imaging offer only limited detection rates for metastatic or recurrent prostate cancer lesions (1). Introduction of 68Ga-labeled prostate-specific membrane antigen (PSMA)–11 significantly improved prostate cancer imaging. With data from more than 3,000 evaluated patients so far (2–6), this tracer has already demonstrated impressive results in the setting of BCR and is most likely also superior to 18F-choline PET/CT (7,8).
Fluorinated tracers, however, might present practical advantages, as the longer half-life of 18F compared with 68Ga (110 min vs. 68 min) might enable centralized production and distribution to satellite centers. Furthermore, there are fewer limitations caused by generator capacity. Therefore, several 18F-labeled ligands were developed, and new tracers have already been evaluated in preliminary clinical investigations (9,10).
One candidate for introduction to clinical routine is 18F-PSMA-1007, which benefits from a low background activity in the urinary tract (10). Unspecific bladder activity can challenge delineation of primary tumors (11) or local recurrence (12,13) and can even hamper evaluation of the pelvic lymph nodes (LNs) by introducing halo artifacts in PET/MR systems (12,13). 18F-PSMA-1007 has already demonstrated its potential for primary tumor staging (10). In the present study, we report the results for 18F-PSMA-1007 PET/CT in the setting of BCR.
MATERIALS AND METHODS
Patients
From May 2016 to July 2017, 12 patients presenting with a rising level of serum prostate-specific antigen (PSA) (median, 0.60 ng/mL; range, 0.08–6.50 ng/mL) after previous local treatment underwent 18F-PSMA-1007 PET/CT. Detailed patient characteristics are provided in Table 1. The institutional review board approved the study (permit S-321), and all subjects gave written informed consent. The data of one study patient (patient 4) have also been published in a case report (14).
Patient Characteristics
PET/CT Imaging
All imaging was performed on a Biograph mCT Flow scanner (Siemens). Images were acquired 63 ± 6 min (1 h) and 180 ± 5 min (3 h) after injection of 18F-PSMA-1007. Median injected activity was 251.5 MBq (range, 154–326 MBq). Tracer synthesis, examination protocol, and image reconstruction were performed as previously described (10).
Tumor Uptake
Tumor lesions were evaluated by a dedicated, board-certified nuclear medicine physician. Lesions were counted and tracer uptake was quantified by SUVmax at 1 and 3 h after injection. Volumes of interest were automatically defined by an isocontour of 40% with e.soft/TrueD software (Siemens). Furthermore, ratios of tumor to blood pool (the volume of interest in the thoracic aorta) were calculated for each lesion.
CT Volumetric LN Assessment
Using semiautomated software (Fraunhofer MEVIS), volumetric analysis on CT correlates of PET-positive LNs was performed as previously described (15) and validated visually by a radiologist. After semiautomated segmentation, short-axis diameter, long-axis diameter, and volume were determined automatically.
Statistical Analysis
Statistical analysis was performed using SPSS software, version 23.0 (IBM Corp.). For comparison of tracer uptake, as well as the ratio of SUVmax to blood pool, at 1 and 3 h after injection, the Wilcoxon signed-rank test was used.
RESULTS
Patient Findings
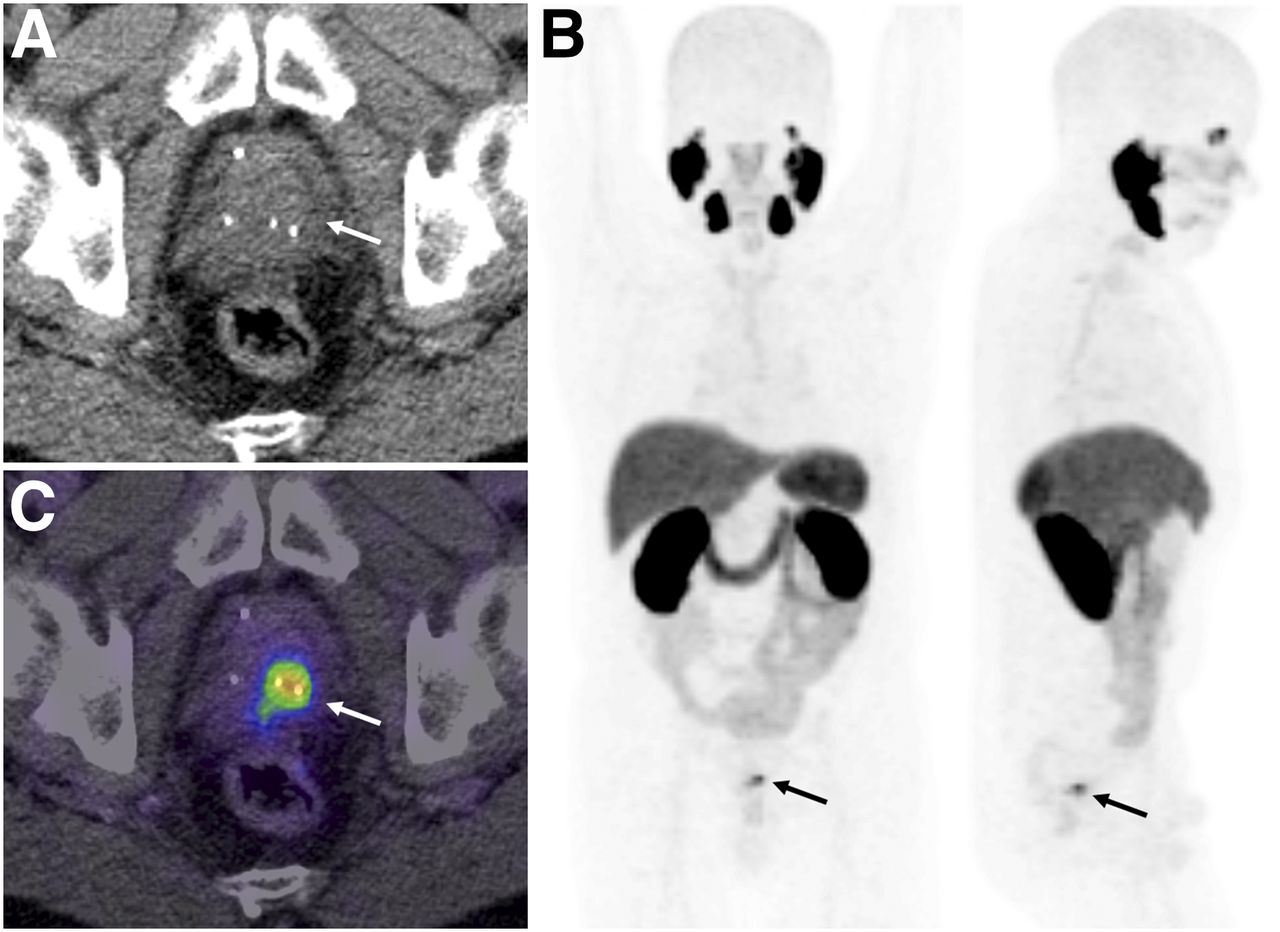
18F-PSMA-1007–positive lesions were detected in 9 of 12 patients (75%). A single local recurrence was found in 3 of 12 patients. Patient 1, initially treated with low-dose brachytherapy, presented with focal uptake between the radioactive seeds (Fig. 1). LN metastases (n = 50) were found in 5 of 12 patients (patients 5–7, with a single 18F-PSMA-1007–positive pelvic LN; patient 5, with 17 positive LNs; and patient 8, with 30 positive LNs) (Fig. 2). Bone metastases (n = 23) were found in 3 of 12 patients, one of whom had no LN metastases. 18F-PSMA-1007 PET/CT was unable to detect any tumor-suggestive lesions in patients 10–12, all of whom had PSA levels of 0.5 ng/mL or less. Table 1 illustrates the distribution of 18F-PSMA-1007–positive lesions among the patients.
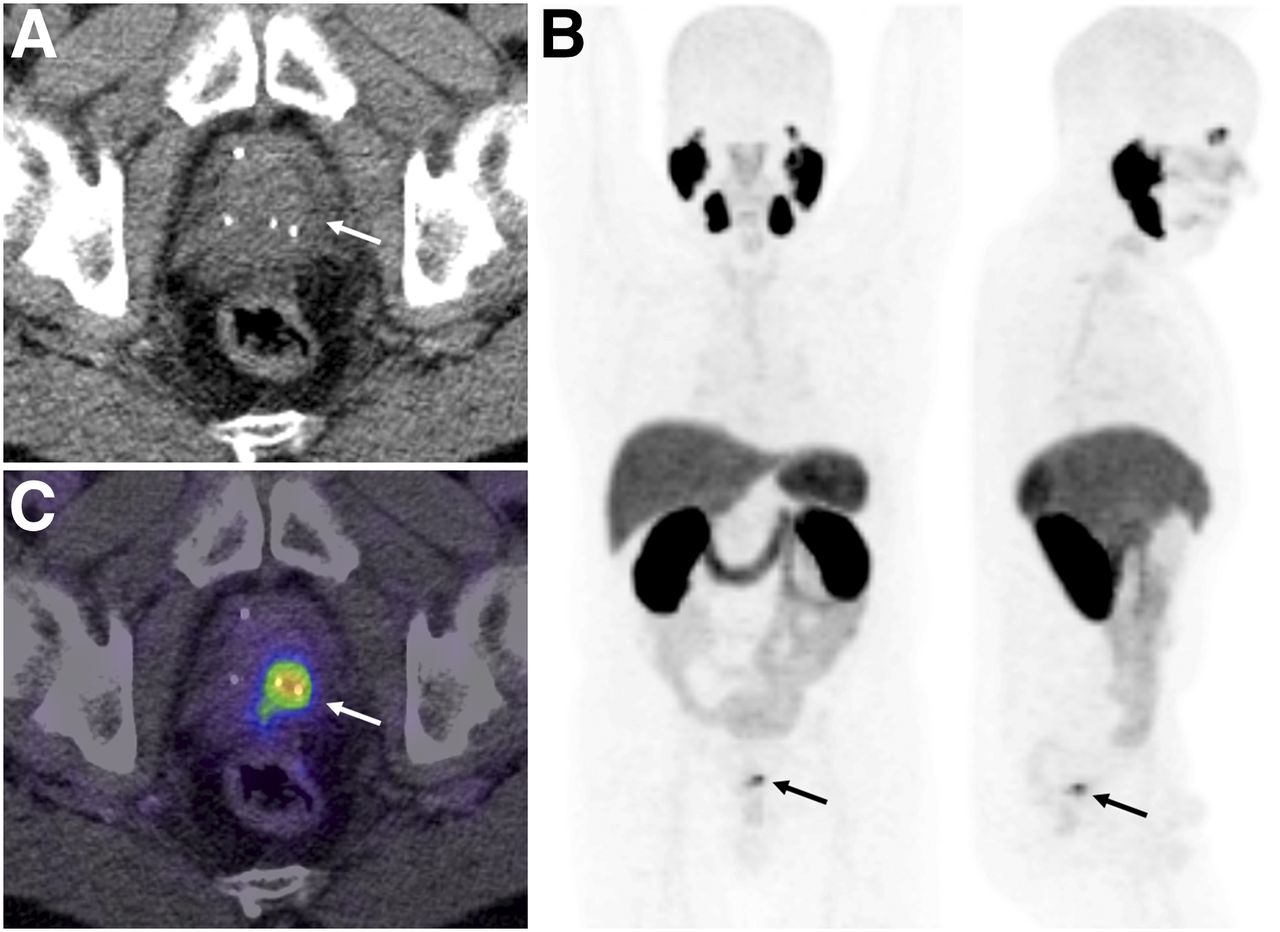
Images of patient 1. (A) After initial brachytherapy, no tumor detection within prostate is achievable with CT alone. (C) With 18F-PSMA-1007 PET/CT, good delineation of local recurrence is possible. (B) Maximum-intensity projection highlights advantage of low urinary clearance, because no PET signal derives from urinary bladder. Arrows indicate location of tumor.
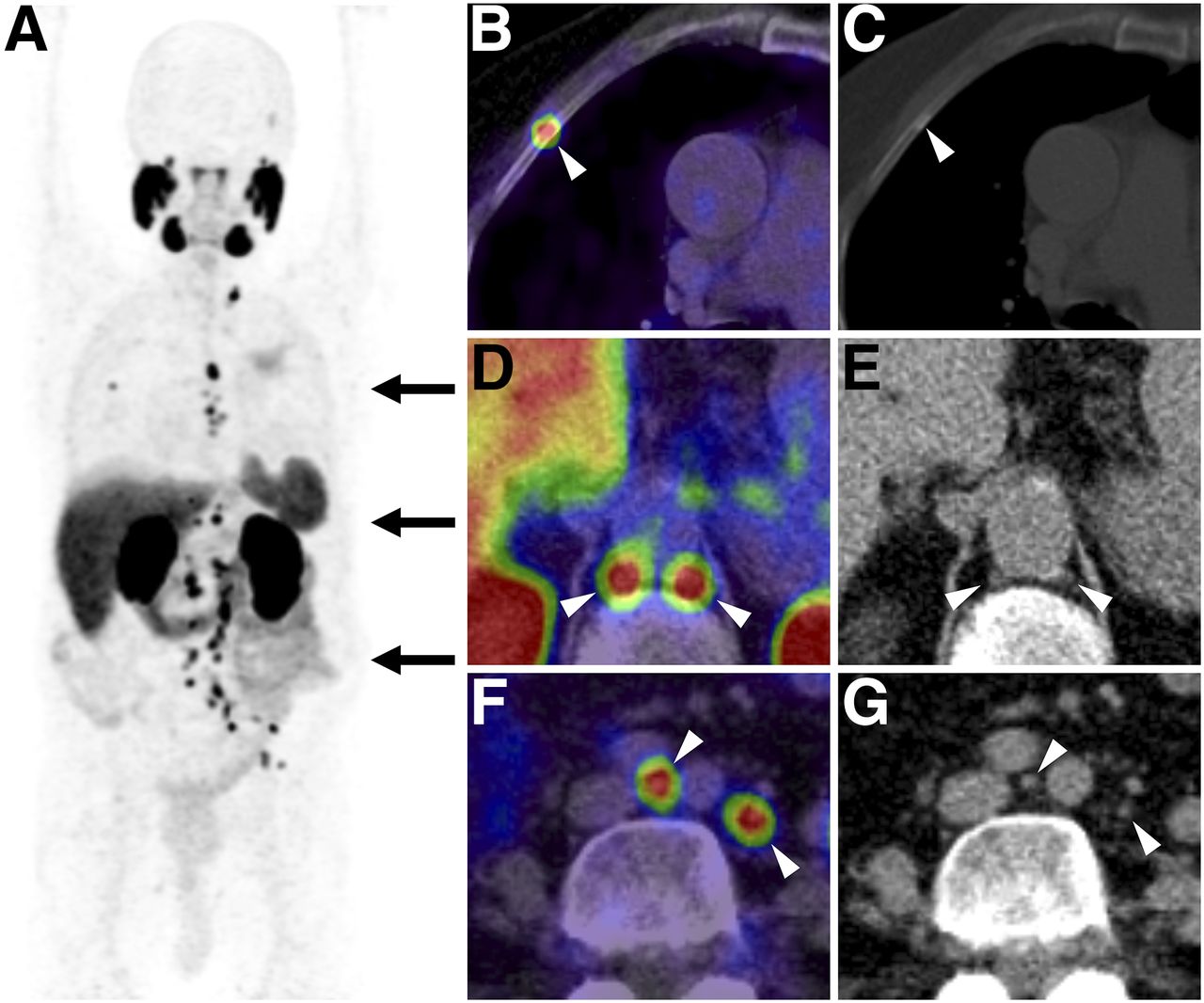
Images of patient 8, who presented with BCR after radical prostatectomy and salvage radiotherapy. 18F-PSMA-1007 PET/CT (maximum-intensity projection, A) detected recurrent disease with multiple bone metastases (B and C) and LN metastases (D–G) 8 y after initial diagnosis. All images were acquired 3 h after injection. Arrowheads indicate locations of tumors.
Clinical Impact
Of the 3 patients diagnosed with local recurrence, 2 had undergone prior radical prostatectomy and were eligible for salvage radiation with a local boost to PET-positive lesions. The patient diagnosed with local recurrence after primary radiotherapy underwent radical prostatectomy with concomitant lymphadenectomy, which confirmed organ-defined recurrence (pTXypN0). In patients 4, 7, 8, and 9, diagnosed with extrapelvic LN or bone metastases, systemic therapy was initiated. Notably, in routine management of BCR these patients would have been candidates for salvage radiation. Patient 5, presenting with a single PET-positive pelvic LN, received salvage surgery, which confirmed the PET/CT results histologically. On follow-up, PSA was undetectable and PSMA PET/CT did not reveal any tumor-suggestive findings.
Tumor Uptake Characteristics
18F-PSMA-1007 PET/CT detected 76 lesions (3 representing local recurrence, 50 representing LN metastases, and 23 representing bone metastases). The median SUVmax for all lesions at 1 h after injection was 7.00 (range, 2.04–40.01). SUVmax increased significantly by 3 h after injection (median, 11.35; range, 2.36–55.05; P < 0.001). Additionally, the ratio of median SUVmax to blood pool increased significantly between 1 and 3 h after injection (2.10 vs. 4.57, P < 0.001). Uptake dynamics and the ratio of SUVmax to blood pool for each lesion group are shown in Figure 3.

(A) Tumor SUVmax increased from 1 to 3 h after injection in all lesion groups. (B) Ratios of SUVmax to blood pool presented improved contrast at delayed time point. Data are mean and SE.
Volumetric Characteristics of PSMA-Positive LNs
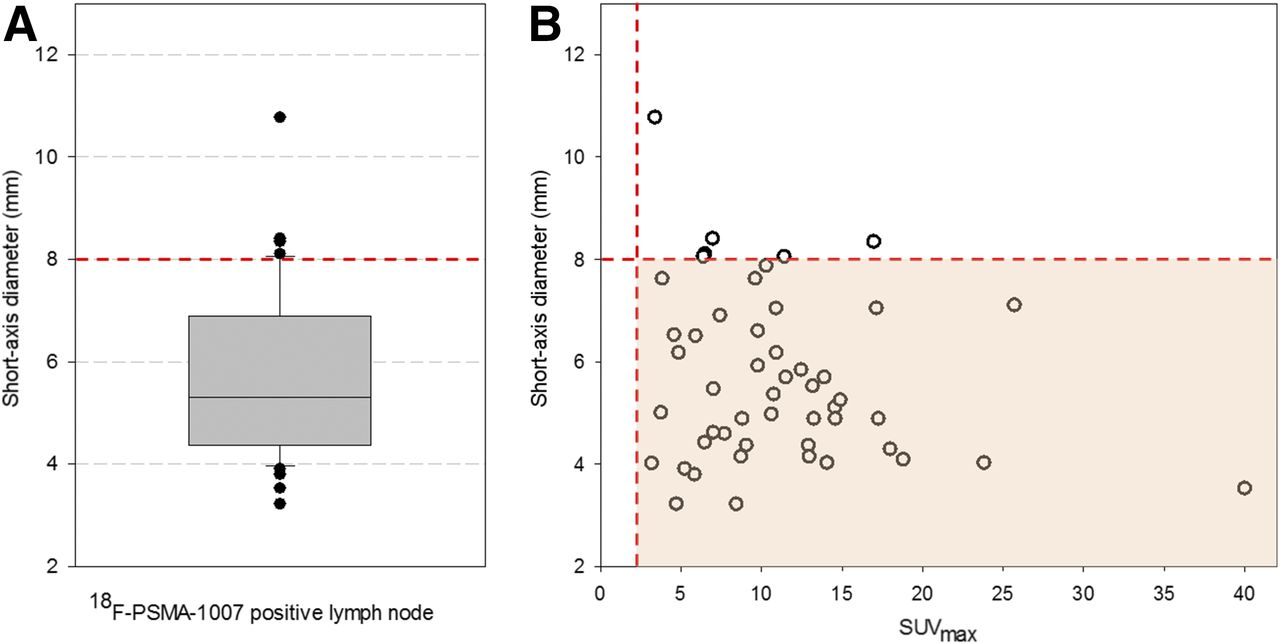
In total, 50 18F-PSMA-1007–positive LNs were evaluated. Their mean short-axis diameter was 5.7 mm (95% confidence interval, 5.2–6.1 mm), their mean long-axis diameter was 8.1 mm (95% confidence interval, 7.5–8.8 mm), and their mean volume was 0.3 mL (95% confidence interval, 0.2–0.4 mL).
Forty-four (88%) of 50 18F-PSMA-1007–positive LNs had a short-axis diameter of less than 8 mm. Figure 4 shows detailed volumetric characteristics and the relation between SUVmax and short-axis diameter.

(A) Analysis of short-axis diameter of 18F-PSMA-1007–positive LNs indicates that 18F-PSMA-1007 PET/CT detects micrometastases that could be missed on CT or MRI. (B) No dependency of SUVmax on lesion diameter was found. Orange dashed reference lines are shown for short-axis diameter of 8 mm and SUVmax of 2.0.
DISCUSSION
To our knowledge, this was the first study evaluating 18F-PSMA-1007 PET/CT in the setting of BCR of prostate cancer. The source of PSA elevation was successfully located in 9 of 12 patients (75%). All 3 patients with negative PET findings had PSA values of 0.5 ng/mL or less. However, 1 patient with positive PET findings had a PSA level of 0.08 ng/mL. These results suggest that 18F-PSMA-1007 has a limited sensitivity below a PSA level of 0.5 ng/mL—a limitation that may be general among PSMA tracers, as similar findings have been reported for 68Ga-PSMA-11 and 18F-DCFPyL (16). In patients undergoing 68Ga-PSMA-11 PET/CT, a sensitivity of 33%–46% has been reported for a PSA level of 0.5 ng/mL or less, improving to more than 80% for higher PSA levels (6,16).
Because the positron energy of 18F is lower than that of 68Ga (0.65 vs. 1.9 MeV), the theoretic achievable resolution of 18F is slightly better than that of 68Ga (17). Therefore, it is hypothesized that the sensitivity of PSMA PET could be further improved by the introduction of 18F-tracers. However, phantom measurements in human scanners found comparable results for both nuclides (18), and a study comparing 68Ga-PSMA-11 and 18F-DCFPyL found minimal differences between the two, with the sensitivity of both decreasing abruptly when PSA was below 0.5 ng/mL (16). Larger comparative trials are required to demonstrate those differences with regard to 18F-PSMA-1007. Nevertheless, the actual findings already imply that, rather than the applied radiolabel, it is the technical resolution limit of current PET/CT scanners (2–3 mm) that might be the limiting factor in the detection of micrometastases.
Assuming similar diagnostic accuracy, the actual added value of 18F-tracers might lie in the possibility of producing large-scale batches in a cyclotron and supplying them through a satellite center, because of the longer half-life. A specific advantage of 18F-PSMA-1007 for the detection of local recurrence may be its low urinary clearance. Additionally, although yet unproven, the similar chemical structure of 18F-PSMA-1007 might allow closer prediction of uptake of the therapeutic ligand PSMA-617, which can be used for PSMA-targeted radioligand therapy (19).
CONCLUSION
This study showed the potential of 18F-PSMA-1007 PET/CT for prostate cancer patients with BCR, confirming that nonvisualization of the urinary bladder facilitates the evaluation of lesions close to the urinary tract, such as local recurrence and pelvic LNs. Nevertheless, these initial results, although limited by a small number of patients, appear comparable to those of 68Ga-PSMA-11 PET/CT.
DISCLOSURE
There have been patent applications for PSMA-617 by Klaus Kopka and Uwe Haberkorn and for PSMA-1007 by Jens Cardinale, Uwe Haberkorn, Frederik Giesel, and Klaus Kopka. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Martin Schäfer for synthesis of the tracer.
Footnotes
Published online Feb. 1, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication May 22, 2017.
- Accepted for publication December 19, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Intraoperative 68Ga-PSMA Cerenkov Luminescence Imaging for Surgical Margins in Radical Prostatectomy: A Feasibility Study
- Detection Efficacy of 18F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- Interobserver Agreement for the Standardized Reporting System PSMA-RADS 1.0 on 18F-DCFPyL PET/CT Imaging