


Abstract
The purpose of this study was to quantify the economic value of bone SPECT/CT versus CT or metal artifact reduction sequence (MARS)-MRI for the diagnostic assessment of recurrent moderate-to-severe pain after total knee arthroplasty (TKA). Methods: An Excel-based simulation model was developed to compare bone SPECT/CT versus CT or MARS-MRI from a payer perspective. Clinical endpoints (diagnosis—delayed or otherwise, and the subsequent treatment and complications) and their corresponding cost data (2017 U.S. dollars) were obtained by performing a best evidence review of the published literature. Studies were pooled and parameters weighted by sample size. A cost-utility analysis was performed estimating the incremental cost per quality-adjusted life years gained between bone SPECT/CT and the comparative scans. One-way (±25%) sensitivity analysis was performed to gauge the model robustness. Results: For every 1,000 TKA patients, diagnostic bone SPECT/CT was expected to lead to 3-y cost savings up to $1,867,695 versus CT (or $622.6 per patient per year) and $1,723,435 versus MARS-MRI (or $574.5 per patient per year) for a payer. With corresponding incremental quality-adjusted life years gains of 39.7 and 41.0 against CT and MARS-MRI, SPECT/CT can be considered as a cost-saving and dominant strategy in the workup of persistent/recurrent pain in TKA patients. The model was limited by the still sparse literature data, was most sensitive to imaging-related sensitivity/specificity, but proved robust for varying prevalence of surgical/nonsurgical causes of pain. Conclusion: Bone SPECT/CT is a potentially highly cost-saving and dominant imaging intervention versus CT or MARS-MR scanning in patients with recurrent and persistent knee pain after TKA.
A record number of 4.7 million Americans were alive with a total knee arthroplasty (TKA) in 2010, and the annual number of procedures is projected to increase to 3.5 million by 2030 (1,2). In parallel, the TKA revision rate has increased 105.9% between 1991 and 2010 (3). With a cost that is 60% higher than the primary procedure, this poses a considerable budgetary challenge and emphasizes the need for careful patient selection (4). The most frequent indications for revision TKA are newly onset or persistent pain (5–7), instability, stiffness, or periprosthetic joint infection (8). Even though pain recurrence after TKA is well documented, the reported prevalence varies widely (between 4.8% and 44%). Identifying the precise cause of pain remains challenging as symptoms and history often lack specificity (9–14). This may delay a correct diagnosis, postpone optimal therapeutic intervention, increase the cost of the diagnostic workup, and can potentially adversely affect patient outcome (8).
Current modalities used in TKA imaging include conventional radiographs, stress radiographs, CT, MRI, planar bone scintigraphy with or without SPECT, or 18F-FDG PET/CT (14). Multidetector CT offers better bone and implant detail than radiographs, which are considered the preferred first-line imaging procedure (15–17). CT can assess the extent of osteolysis, periprosthetic fractures, and TKA malpositioning, but the technique is limited in differentiating inactive from active anatomic lesions (15). More recently, due to improvements in metal artifact reduction sequence (MARS) protocols, there is renewed interest in the use of MRI in this setting (15). In parallel, fully integrated SPECT/CT devices have overcome the limited spatial resolution of SPECT-only imaging, resulting in significantly improved diagnostic accuracy and providing a unique combination of simultaneous evaluation of skeletal anatomy and physiology (14,16). Moreover, the use of bone-affine tracers with SPECT/CT offers the advantage of linking bone turnover patterns with biomechanical information on TKA placement and loading (18). This additional information can assist in selecting appropriate clinical management and assessing whether further surgical treatment is warranted (14,16,17,19). However, it is unclear whether these clinical benefits translate into successful economic and humanistic (e.g., quality-of-life [QoL]) outcomes. Therefore, this economic simulation study aimed to quantify the potential economic value and cost utility of bone SPECT/CT compared with other imaging technologies (CT, MARS-MRI) in assessing persistent or recurrent knee pain after TKA from a payer perspective.
MATERIALS AND METHODS
Model Scaffold
The diagnostic algorithm published by Park et al. combines physical examination, radiographs, and laboratory workup to stratify patients toward further diagnostic procedures (6). Following this decision-tree, instability/malposition and acute infection were not considered within the current model, as these conditions may be adequately characterized without advanced imaging techniques. However, additional imaging may be required for the accurate diagnosis of implant loosening/wear/osteolysis, chronic low-grade infection, and patellofemoral problems (includes anterior knee pain, extensor mechanism problems, avascular necrosis, and patellar overstuffing/maltracking). On the basis of an extensive literature review, the model focused on the differential diagnosis of these 3 conditions as these represent the most frequent causes of post-TKA pain (Fig. 1) (14,16,20–41). The model also assumed: 1 primary causal condition; a nondiagnostic CT would be complemented with a MARS-MRI and vice versa, and an equal split between CT and MARS-MRI when bone SPECT/CT was nondiagnostic; the second imaging procedure was always diagnostic (to avoid an infinite loop); in case of a nondiagnostic scan, a subsequent scan was done after a 6-mo medical pain management regimen; medical management involved a 70:30 mix of nonsteroidal antiinflammatory drugs (NSAIDs) plus physiotherapy or steroid injections with occasional nonnarcotic analgesics (e.g., acetaminophen); with regular office visits for pain-monitoring and treatment of any adverse events (including general, cardiovascular or gastrointestinal toxicity, skin flares, or sepsis); and medical management did not result in long-term relief given the severity of the underlying condition and associated functional limitations.
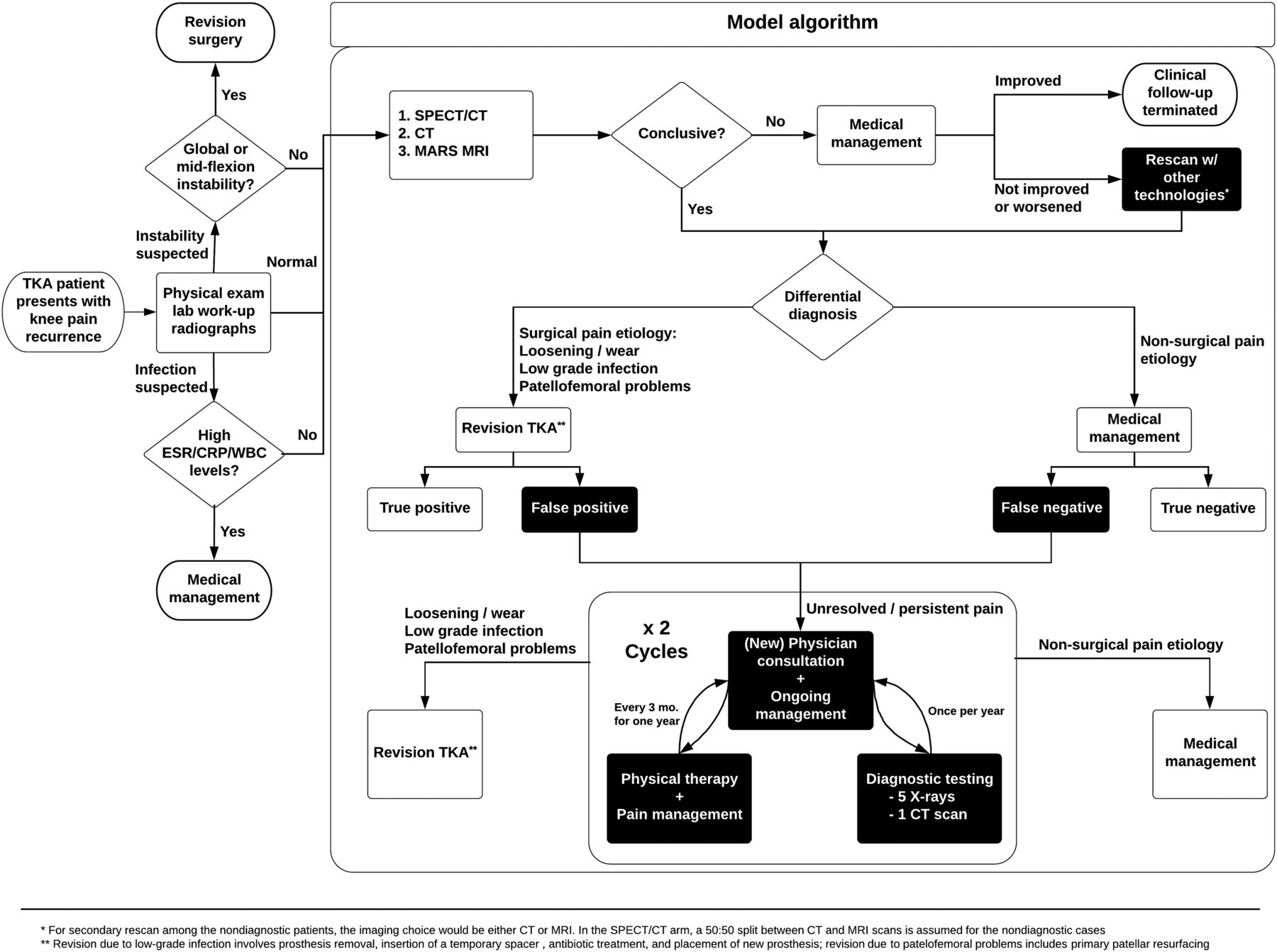
Model scaffold: proposed care pathway. CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; WBC = white blood cells.
The study modeled a hypothetical cohort of 1,000 TKA patients experiencing recurrent moderate-to-severe pain over a 3-y period. If diagnosed with a noninfectious cause, patients undergo a 1-stage revision TKA: removal of TKA components and implantation of revision TKA (42). Primary patellar resurfacing was done in the case of patellofemoral issues, whereas 13.8% of the loosening group also received secondary patellar resurfacing (Table 1) (21). For the chronic infection cohort, a 2-stage exchange arthroplasty was performed: removal of all components, placement of a temporary antibiotic-laden cement spacer with subsequent extended intravenous or oral antibiotic regimen to eradicate the infection, followed by revision TKA (43). To model specificity, 10% of the cohort was assumed to have pain caused by other conditions that did not require a surgical intervention, as first-line workup was expected to detect most of these patients before entering the modeled pathway (Fig. 1). The model also accounted for the risk of major and minor complications among the surgery patients (Table 2). Patients correctly treated with surgical intervention (true-positives) were assumed to have no further treatment beyond the standard postsurgery management (e.g., physiotherapy and monitoring) and to remain pain-free for the duration of the study (Table 3). All improperly treated patients (i.e., the false-positives and -negatives) were assumed to have failed the treatment and to have derived no benefits. These patients continued to experience painful knees of undetermined origin and spend at least 2 y (44) in identifying the true cause of their condition before undergoing delayed TKA revision. During this wait-and-watch strategy, patients received annual radiographs and a CT scan and intensive medical management (70:30 mix of NSAIDs and steroid injections) with physiotherapy. Concurrently, quarterly visits to an orthopedic surgeon or general practitioner for consulting and management reasons were included. True-negatives continued to be on a medical management pathway. These event pathways were constructed on the basis of a literature review and clinical expert opinion.
Demographic, Disease, and Imaging Model Parameters
Revision Surgery and Unresolved Pain Base Case Model Parameters
Medical Management Base Case Model Parameters
A best evidence review of PubMed articles published between January 1, 2006, and March 31, 2017 was performed to obtain default parameter values. Selection criteria included English-language studies considered to be most relevant (e.g., adult human subjects, in vivo) to the clinical and imaging application(s) in question. Case reports and case series with a sample size of fewer than 15 (arbitrarily chosen) were excluded. For the imaging-related parameters, studies assessing sensitivity, specificity, or nondiagnostic rates were identified. Descriptive data from single-modality series were used if direct comparison data were unavailable. Sample size weighted estimates were synthesized in the case of multiple data sources to mitigate outlier bias (45).
Health States
Seven health states were considered in total (Fig. 2). After revision surgery, a transition was assumed within 3 mo, to one of the following: full-benefit state, an early failed/limited-benefit state, or death. The latter was an absorbing state because of surgical mortality. A successfully revised patient was allocated to the full-benefit health state until the end of the model. False-positives and -negatives entered the failed/limited-benefit state. After the implementation of the wait-and-watch strategy, they would be correctly treated for the underlying cause of the pain, before transitioning to the full-benefit state.
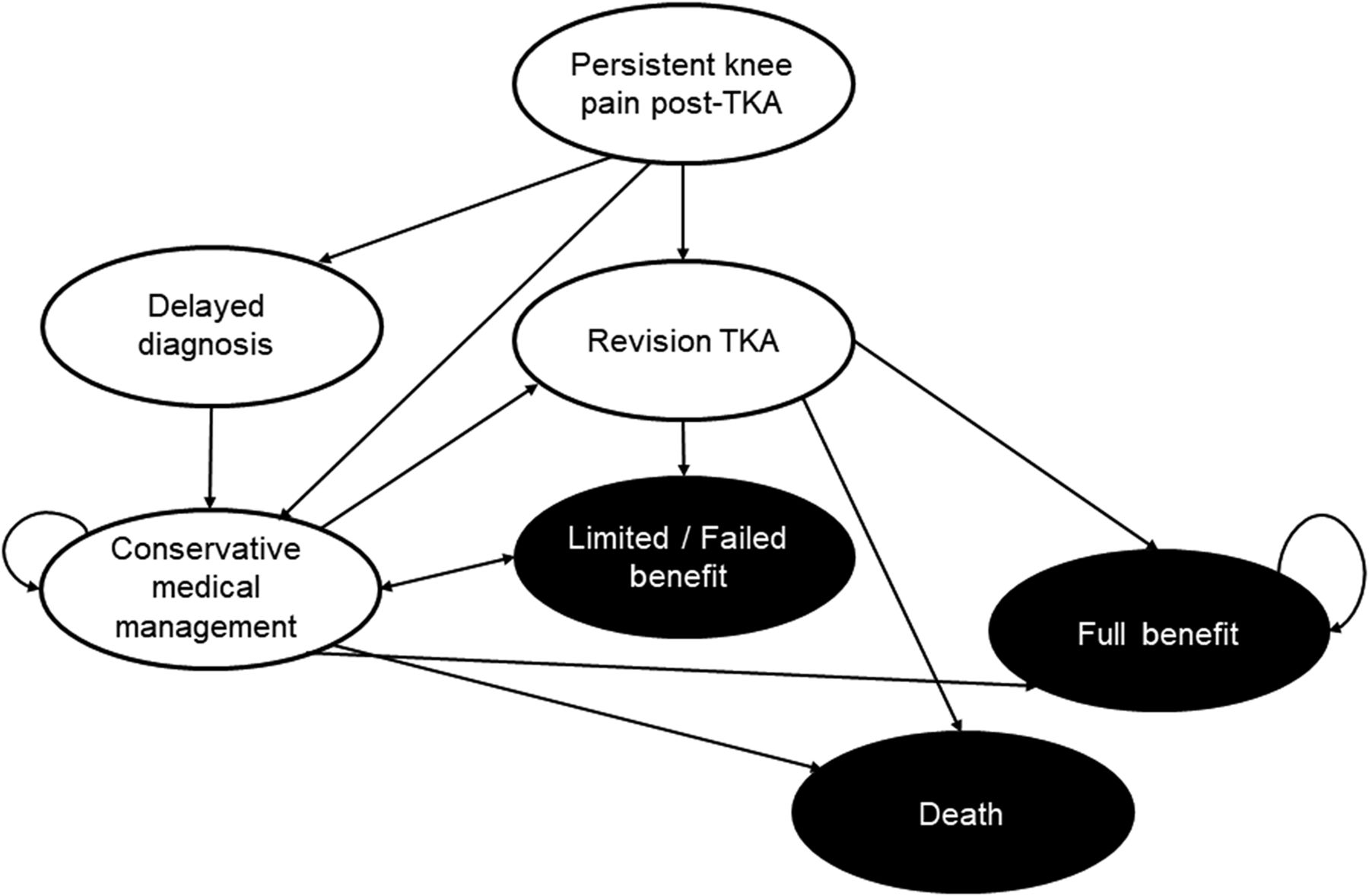
Health state diagram representation.
Utilities
Utility factors (0 = death; 1 = perfect health) were assigned to all health states (based on orthopedic literature data) to adjust survival for QoL and were expressed as quality-adjusted life years (QALYs) by multiplying the length of time spent in a health state with its corresponding utility (Table 4) (46). To represent the short-term negative impact of TKA revision on QoL (47) (reduced mobility, pain, and nonlethal complications after surgery), a one-time deduction was applied by multiplying the acute procedure toll with the recovery time (3 mo) to the patient QALYs in the procedure year (48). On the basis of published evidence, the disutility of having a revision TKA was set at −0.19 with no distinction placed on the aseptic and septic cause given the low prevalence of chronic infection in our model (16.7%).
Utilities (Time): Base Case Model Parameters
Cost Estimates
To represent the payer’s perspective, the 2017 national average Medicare professional and technical fees were extracted on the basis of the specific current procedural terminology (CPT) codes for each modality (49). Baseline revision arthroplasty procedure cost was derived from 2014 Health Care Cost and Use Project data (50) with add-on costs for each additional complexity (e.g., antibiotic-laden spacer and antibiotic regimen for infectious patient (51), patellar resurfacing (52), and any perioperative complication(s) (27,40,41,47,53–55)). Medical management costs accrued during the 3-mo postsurgery period accounting for care provided in inpatient settings, physician services, and postacute care facilities (e.g., skilled nursing or rehabilitation facilities, home health, hospice, or long-term care) were included. Cost estimates were inflated to 2017 U.S. dollars using the Bureau of Labor Statistics’ US Medical Care Consumer Price Index (56). Non-Medicare (commercial) payments were calculated for persons aged 65 or younger based on Medicare payments. Given the study’s short time frame, discounting was not considered.
Outcomes
For each imaging modality: the total 3-y cost burden was the cumulative cost of diagnostic imaging scan and rescans; revision surgery (surgery, perioperative complications) and postsurgical management; medical management (office visits, physiotherapy, NSAIDs, injections, analgesics, and any potential adverse events associated with these treatments); and monitoring (radiographs, CT, surgeon consultations, office visits) during the wait-and-watch approach. Total QALYs were calculated as the sum of the utility of each of the 7 health states multiplied by the time spent in each health state.
Cost-effectiveness of SPECT/CT was defined as the ratio of incremental difference in costs and QALYs between SPECT/CT and the comparator technique and expressed as the incremental cost-effectiveness ratio of SPECT/CT per QALY gained.
Sensitivity Analysis
To assess the impact of the individual model parameters and robustness of the findings, a 1-way sensitivity analysis was conducted by varying each model parameter by ±25% of its base case estimate. Further, the impact of the 10% prevalence of nonsurgical causes on the results was explored in a separate sensitivity analysis, to increase the applicability of the model’s findings in other care settings. This model was built using Excel 2013 (Microsoft Corp.).
RESULTS
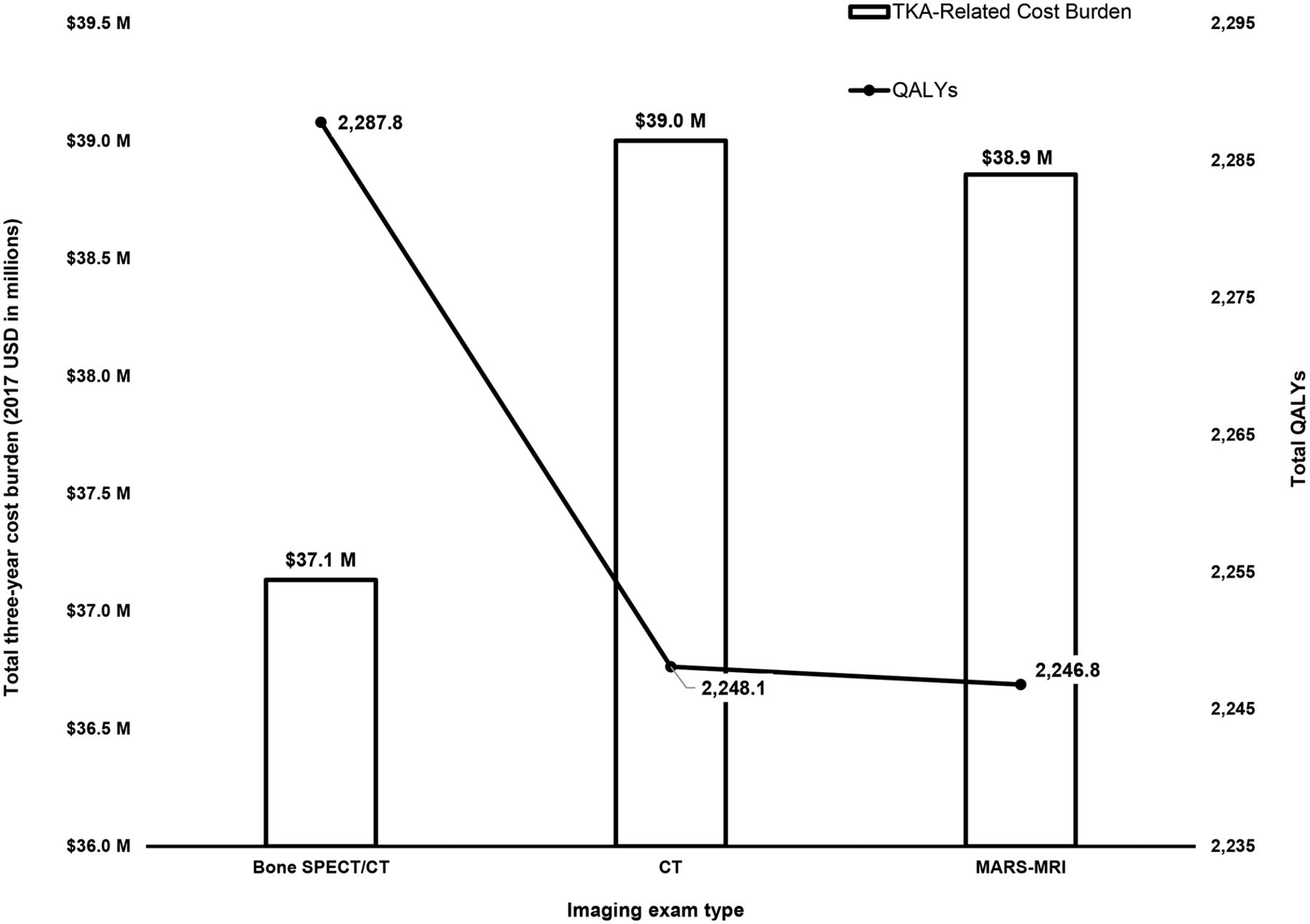
For every 1,000 TKA patients experiencing recurrent and persistent moderate-to-severe pain and undergoing diagnostic bone SPECT/CT, CT, or MARS-MRI, the total 3-y burden was expected to be $37,133,788, $39,001,483, and $38,857,223, respectively (Fig. 3). Therefore, SPECT/CT was found to result in $1,867,695 lesser costs for a payer versus CT over 3 y or $622.6 per patient per year. SPECT/CT’s lower costs against CT appeared to be primarily driven by its improved accuracy, thus avoiding undue surgeries and ad hoc medical management for the major duration of the study period. Switching from MARS-MRI was also found to save the payer approximately $1,723,435 ($574.5 per patient per year). SPECT/CT’s relatively higher sensitivity and specificity reduced overall use, which in turn lowered costs for the hybrid technology cohort. A total of 908, 926, and 914 revision surgeries were performed in the SPECT/CT, CT, and MARS-MRI cohorts, respectively, of which 1.7%, 18.8%, and 16.9% were deemed as late/delayed procedures because of a false-negative diagnosis, respectively.

Economic burden and QALYs, by imaging type.
In terms of QALYs, SPECT/CT, CT, and MARS-MRI were found to be associated with QALYs of 2,287.8, 2,248.1, and 2,246.8, respectively: that is, QALY gains of 39.7 and 41.0 for SPECT/CT versus CT and MARS-MRI, respectively. The life-years gained were a direct function of the bone SPECT/CT cohort receiving the highest successful revision surgery rate early during the study period. CT’s nonoptimal management because of its lower diagnostic rate and specificity was also found to have contributed to its lower QALYs. Since SPECT/CT was found to lower costs and improve QALYs, this imaging modality can be considered as a highly cost-effective and dominant strategy for diagnosing recurrent and persistent knee pain in TKA patients.
Sensitivity Analysis
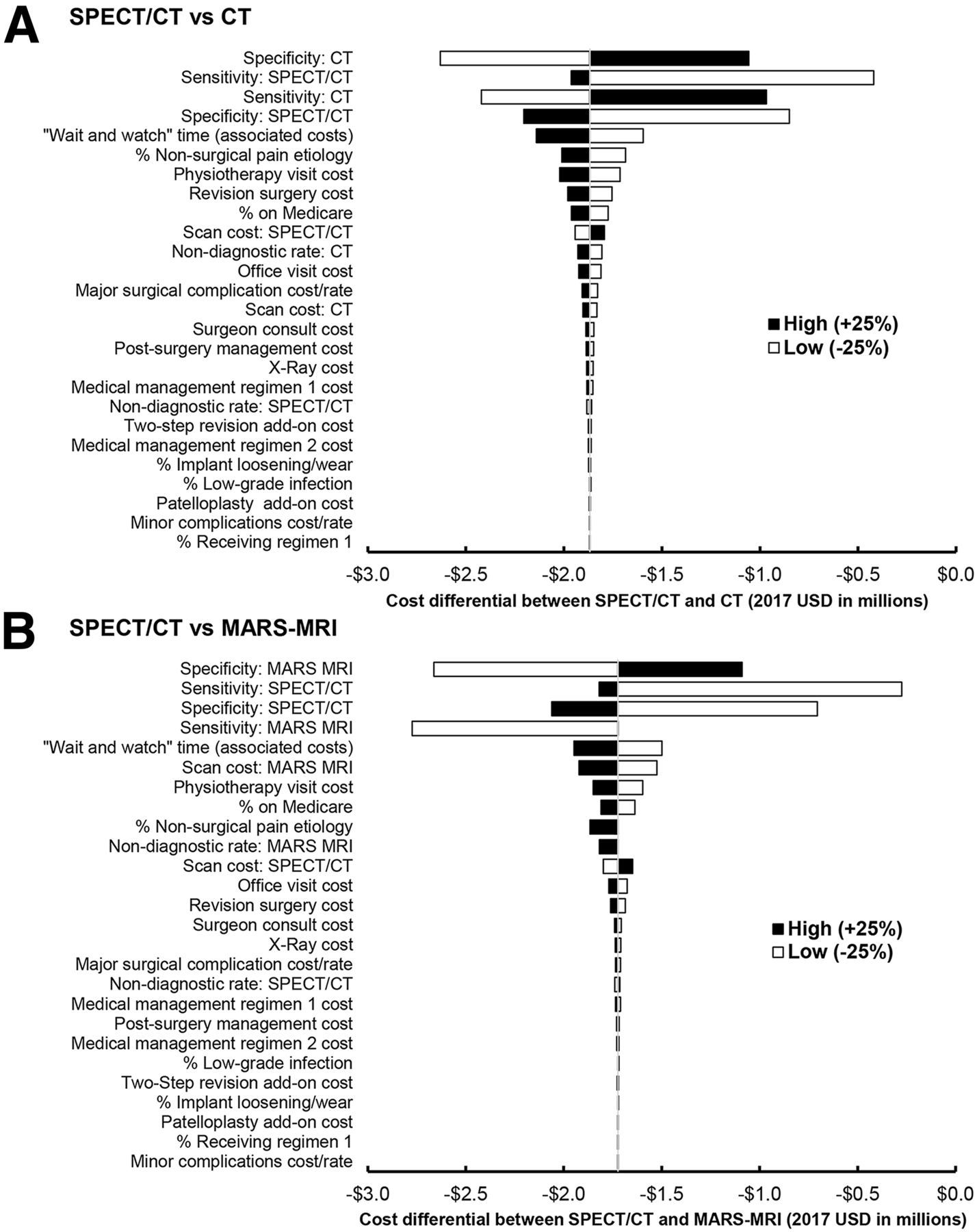
The model was most sensitive to imaging-related parameters, especially sensitivity/specificity, and wait-and-watch-period related costs (Fig. 4). SPECT/CT was found to be always cost-saving/neutral even with a ±25% change in their base case parameter values. In addition, changing the prevalence of nonsurgical causes of painful TKA affected the cost-savings and QALYs gained by SPECT/CT over CT and MARS-MRI in a proportional way, but it remained cost-saving and dominant (Supplemental Fig.1; supplemental materials are available at http://jnm.snmjournals.org).
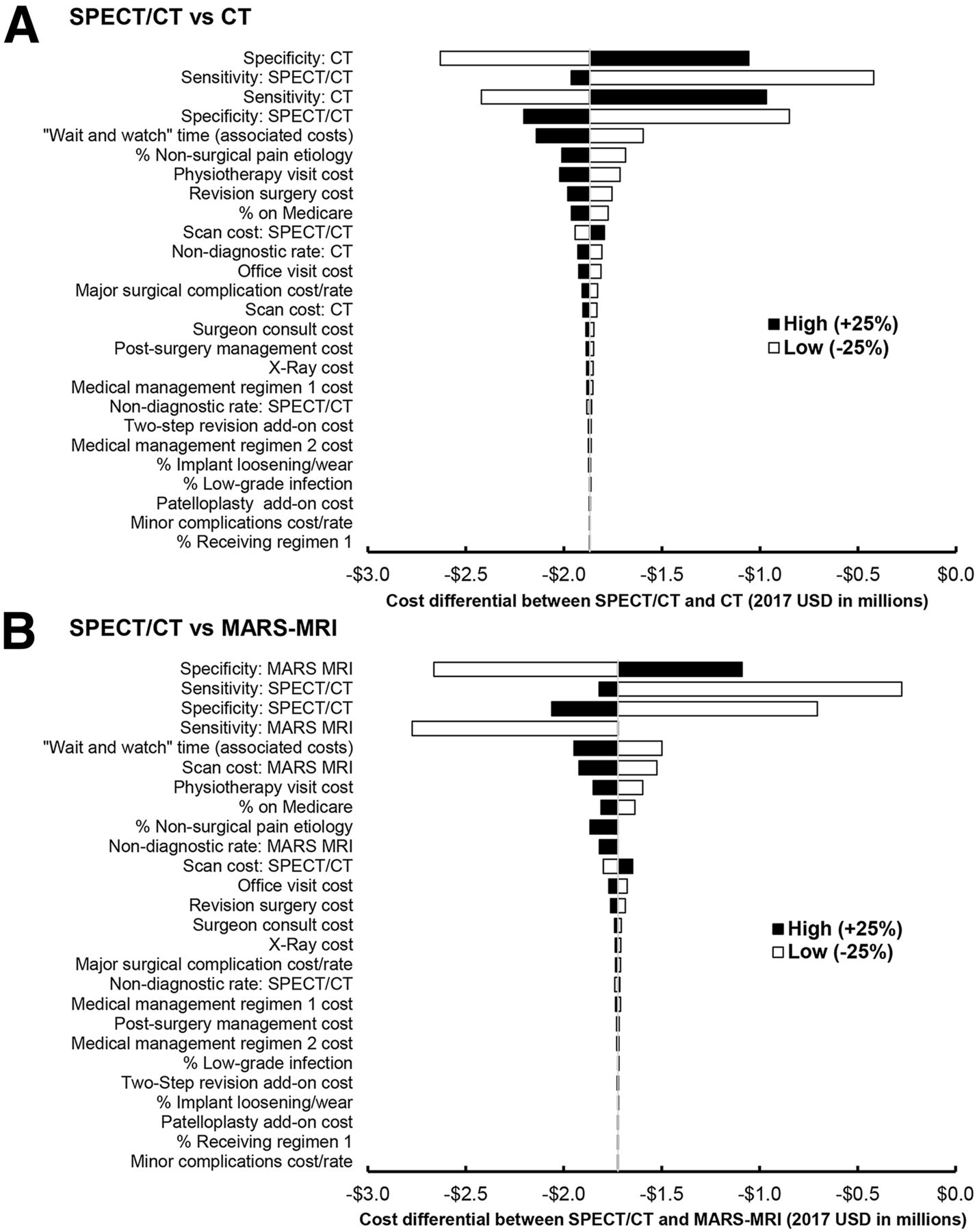
One-way sensitivity analysis (tornado diagram) for SPECT/CT vs. CT (A) and MARS-MRI (B).
DISCUSSION
Despite plateauing TKA failure times (mean, 5.9 y) (57–59), increasing primary TKA rates are driving the growing number of revision procedures (∼101,290 in the United States in 2017) (2). With an average hospitalization cost of $29,584 (50), the total inpatient revision TKA burden in 2017 alone aggregated to nearly $3 billion, highlighting the impact on budgets and increasing strain on surgeons, patients, and health systems (2,50). A prompt and accurate diagnosis is pivotal, as the outcome of revision is very poor (failure rate up to 80%) if the root cause is left undetermined before surgery (60). Diagnostic algorithms to streamline the workup and maximize their yield firmly rely on imaging procedures (6,14). It is therefore not surprising that imaging services account for 18.2% of payments of knee osteoarthritis–related health care expenditure, exceeding the cost of outpatient office evaluations and prescription nonnarcotic analgesic medications (61). Hence, interventions that can improve diagnostic accuracy and assist surgeon decision making will be of paramount importance for optimal patient management, long-term outcomes, and budget control. Integrated bone SPECT/CT is the newest entry in this space and is considered superior to conventional bone SPECT imaging because of its improved resolution, attenuation and scatter correction, and accurate anatomic localization (62). Indeed, very high diagnostic accuracies of bone SPECT/CT have recently been reported for evaluating knee prosthesis patients, translating into a change in diagnosis or treatment plan in nearly 50.7% (16%–85.5%) of cases (14,16,17,19) compared with the impact of MRI or CT, which was only 36%–48.8% (24,63,64). The current study, to our knowledge, is the first to evaluate the value of bone SPECT/CT from a cost perspective.
For every 1,000 patients experiencing moderate-to-severe persistent pain after TKA, the 3-y burden was calculated to be $37.1, $39.0, and $38.9 million for diagnostic SPECT/CT, CT, or MARS-MRI, respectively. SPECT/CT’s cost savings (per patient per year of $622.6 and $574.5 vs. CT and MARS-MRI, respectively) are driven by its higher diagnostic accuracy and reduction of unnecessary revision surgeries (18 and 6 procedures for every 1,000 CT/MARS-MRI patients switching to SPECT/CT). In addition, avoiding surgeries saved 17 (vs. CT) and 14 (vs. MARS-MRI) more lives, thereby improving the SPECT/CT cohort’s survival by 2% and 1%, respectively. SPECT/CT was also found to be associated with QALY gains of 39.7 and 41.0 compared with CT and MARS-MRI, making it a dominant intervention. The additional life-years gained by the SPECT/CT cohort are likely realized by redirecting patients sooner to the appropriate surgical intervention compared with other techniques, whereas CT’s nonoptimal management (e.g., high nondiagnostic rate) further lowered QALYs in that group. Indeed, early and timely management at relieving pain may prevent the domino effect of a chronic failed state on a patient’s QoL. Conservatively, our model did not assume an increase in pain severity during the 2-y wait-and-watch period, even though this may be important (44,65).
Incorporating novel imaging techniques such as SPECT/CT in the presurgery workup may contribute to improved selection of appropriate surgical approach. Indeed, identifying the origin of the pain and whether or not it has a surgically rectifiable cause is critical to optimize patient management. Coupled with the anticipated rise in revision procedures, SPECT/CT may prove to be an important component to optimize revision arthroplasty effectiveness. We recognize that the management of painful TKA requires a multidisciplinary approach involving surgeons, physiotherapists, and pain management teams (7), and the optimal use of SPECT/CT will require a further intensive collaboration of the referring orthopedic surgeon and the nuclear medicine physician or radiologist (14). This could be facilitated by the introduction of multidisciplinary team discussions, similar to those ubiquitously established in the oncology setting.
Like every economic analysis, this model is limited by its simplistic real-world representation. In particular, it focuses only on the top 3 of most common intrinsic pathologies requiring surgery, and assumes a singular causal condition. Conflicting reports exist in implicating aseptic (polyethylene wear, prosthetic loosening, and instability) and septic indications as the primary mechanism for failed TKA. Variability also exists across patient characteristics, failure modes, procedure types, and use across hospitals and regions, which the model does not address (21). The reader should therefore carefully assess the applicability of our findings to his or her own context. It should also be acknowledged that available literature evaluating the accuracy of imaging tests is relatively sparse, and the published studies often had small patient numbers and differed with respect to image acquisition protocols (which may evolve over the time) and reference standards (typically a composite of clinical, radiologic, laboratory, and surgical follow-up). None of the included studies on SPECT/CT or CT implemented MAR techniques that may further improve their accuracy. However, this limitation in our dataset applied to both techniques and did not favor one above the other. Taken together, our results are subject to the heterogeneity present in current literature data but are sufficiently provocative to merit further research.
CONCLUSION
For every 1,000 patients experiencing moderate-to-severe persistent pain after TKA, the total 3-y burden was calculated to be $37.1, $39.0, and $38.9 million for bone SPECT/CT, CT, or MARS-MRI, respectively, leading to SPECT/CT’s per patient per year cost savings of $622.6 (vs. CT) and $574.5 (vs. MARS-MRI). With corresponding incremental QALY gains of 39.7 and 41.0 against CT and MARS-MRI, SPECT/CT can be considered as a cost-saving and dominant strategy for orthopedic knee diagnostic purposes. Future evaluation of this technique in a larger number of patients and multiple centers, possibly in a prospective and controlled fashion, would help to more confidently address the value of this technique.
DISCLOSURE
This study was sponsored by GE Healthcare. Swetha R. Palli and Ryan J. Imhoff are employees of CTI Clinical Trial and Consulting Services, Inc., which is a paid consultant to GE Healthcare. Dr. Hirschmann reports personal fees from DepuySynthes, Lima, Symbios, Smith&Nephew, and Arthrex, as well as grants from Finceramica, Italy, outside the submitted work. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Mar. 30, 2018.
- © 2018 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication November 20, 2017.
- Accepted for publication March 15, 2018.





{kind=link}
{kind=link}
{kind=link}
{kind=link}