


Abstract
Metastatic infection is an important complication of Staphylococcus aureus bacteremia (SAB). Early diagnosis of metastatic infection is crucial, because specific treatment is required. However, metastatic infection can be asymptomatic and difficult to detect. In this study, we investigated the role of 18F-FDG PET/CT in patients with SAB for detection of metastatic infection and its consequences for treatment and outcome. Methods: All patients with SAB at Radboud University Medical Center were included between January 2013 and April 2016. Clinical data and results of 18F-FDG PET/CT and other imaging techniques, including echocardiography, were collected. Primary outcomes were newly diagnosed metastatic infection by 18F-FDG PET/CT, subsequent treatment modifications, and patient outcome. Results: A total of 184 patients were included, and 18F-FDG PET/CT was performed in 105 patients, of whom 99 had a high-risk bacteremia. 18F-FDG PET/CT detected metastatic infectious foci in 73.7% of these high-risk patients. In 71.2% of patients with metastatic infection, no signs and symptoms suggesting metastatic complications were present before 18F-FDG PET/CT was performed. 18F-FDG PET/CT led to a total of 104 treatment modifications in 74 patients. Three-month mortality was higher in high-risk bacteremia patients without 18F-FDG PET/CT performed than in those in whom 18F-FDG PET/CT was performed (32.7% vs. 12.4%, P = 0.003). In multivariate analysis, 18F-FDG PET/CT was the only factor independently associated with reduced mortality (P = 0.005; odds ratio, 0.204; 95% confidence interval, 0.066–0.624). A higher comorbidity score was independently associated with increased mortality (P = 0.003; odds ratio, 1.254; 95% confidence interval, 1.078–1.457). Conclusion: 18F-FDG PET/CT is a valuable technique for early detection of metastatic infectious foci, often leading to treatment modification. Performing 18F-FDG PET/CT is associated with significantly reduced 3-mo mortality.
Staphylococcus aureus bacteremia (SAB) is a severe infection known for its high morbidity and is associated with a 30-d overall mortality of 20% (1). An important complication of SAB is metastatic infection, with a reported incidence between 16% and 68% (2–7). Known risk factors for development of metastatic infection in SAB patients are community acquisition of the bacteremia, signs of infection present for more than 48 h before initiation of appropriate antibiotic treatment, fever more than 72 h after initiation of appropriate antibiotic treatment, and positive blood cultures more than 48 h after initiation of appropriate antibiotic treatment (3). Early detection of metastatic infection is crucial, because morbidity and mortality are higher in the presence of these foci, probably due to incomplete eradication during treatment (8). However, metastatic infectious foci are often asymptomatic. In up to one third of patients with Gram-positive bacteremia and metastatic foci, localizing signs and symptoms are absent (8).
During the past years, 18F-FDG PET/CT has been extensively used in diagnosing infectious diseases (IDs). Previous studies on the value of 18F-FDG PET/CT in metastatic infection have demonstrated that 18F-FDG PET/CT detects infectious foci in patients with bacteremia or infective endocarditis and leads to a decrease in relapse and mortality rate (9,10). Furthermore, 18F-FDG PET/CT has shown to be cost-effective in patients with Gram-positive bacteremia (11). The previous studies, however, did not report on how 18F-FDG PET/CT optimizes treatment in SAB, whereas the positive effect on outcome is undoubtedly caused by treatment modification. Therefore, the aim of this study was to investigate the diagnostic value of 18F-FDG PET/CT for newly diagnosed metastatic infection, subsequent treatment modifications, and outcome in patients with SAB, with a focus on patients with high-risk bacteremia.
MATERIALS AND METHODS
Study Design and Patients
This retrospective cohort study was performed at Radboud University Medical Center, Nijmegen, The Netherlands. All consecutive adult SAB cases between January 2013 and April 2016 were included. SAB was defined as 1 or more blood cultures positive for S. aureus. SAB cases were designated hospital-acquired if patients had been admitted for at least 48 h before the first positive blood culture, or as community-acquired in all other cases. Exclusion criteria were pregnancy and death within 48 h after the first positive blood culture with S. aureus. According to the Dutch law, this study was exempt from approval by an ethics committee, because of the retrospective character of this study and the anonymous processing of data. The regional institutional review board approved this retrospective study, and the requirement to obtain informed consent was waived.
Data Collection
We reviewed the medical records of all patients and collected data on patient demographic characteristics; estimated prognosis of preexisting underlying disease and comorbidity according to the Charlson comorbidity score (12); and determined onset of bacteremia, presence of intravascular catheters or foreign body material, resistance of S. aureus to methicillin, foci of infection, and clinical parameters at SAB onset, diagnostic investigations, antimicrobial therapy, and outcomes. The data were retrieved electronically from clinical charts and reports of diagnostic studies (including laboratory, microbiologic, and imaging data).
Diagnostic Workup
According to definitions established previously (3,8), cases were designated high-risk SAB if one of the following criteria for increased risk of metastatic infection was met: community acquisition of the bacteremia, signs of infection for more than 48 h before initiation of appropriate antibiotic treatment, fever more than 72 h after initiation of appropriate antibiotic treatment, positive blood cultures more than 48 h after initiation of appropriate antibiotic treatment, or already confirmed metastatic foci at the moment of presentation. For all patients with high-risk SAB, echocardiography and 18F-FDG PET/CT were recommended.
An integrated PET/CT scanner (Biograph 40 mCT; Siemens Healthcare) was used. Before 18F-FDG injection, patients fasted and any glucose- or insulin-containing infusions were discontinued for at least 6 h. In 66.7% of patients, a low-carbohydrate fat-allowed diet was followed 24 h before 18F-FDG PET/CT. Blood glucose samples were taken from all patients before 18F-FDG administration. At the time of 18F-FDG injection, glucose was below 12 mmol/L in all patients, including diabetic patients. One hour after intravenous injection of an average dosage of 3.3 MBq × body weight (kg)/min/bed position of 18F-FDG (Mallinckrodt Pharmaceuticals or IBA Molecular), a whole-body low-dose CT was acquired for anatomic correlation and attenuation correction of the PET data. Emission images of the same area were acquired. 18F-FDG PET/CT scans were considered abnormal if focal accumulation of 18F-FDG was detected. Normal test results were considered true-negative when no complicating infectious foci were diagnosed within 2 wk after 18F-FDG PET/CT was performed. Normal test results were considered false-negative when a localized infectious focus was diagnosed but not reported on 18F-FDG PET/CT. Abnormal test results not related to metastatic infection that were caused by a confirmed alternative diagnosis (i.e., cancer) were categorized as noninfectious relevant.
In all patients with SAB, the local antimicrobial stewardship program recommends bedside consultation by an ID specialist as well as echocardiography. Transthoracic echocardiography was used as a first-line screening technique, except for those patients with prosthetic valves, in whom transesophageal echocardiography was the first-line technique. Transesophageal echocardiography was recommended in all patients in whom transthoracic echocardiography was negative for endocarditis, especially when imaging was hampered by technical or anatomic problems. Endocarditis was defined according to the modified Duke criteria (13).
Patients were treated according to the national guideline for SAB, which is concordant with the Infectious Diseases Society of America guideline (14). However, for patients with risk factors for metastatic foci but without evidence of endocarditis after echocardiography and without signs of metastatic infection on 18F-FDG PET/CT, the institutional guideline recommends antimicrobial therapy for 2 wk. These patients were considered as having uncomplicated bacteremia instead of complicated bacteremia.
Diagnosis and Patient Follow-up
Patient outcome and recurrent infection were assessed by reviewing patients’ medical records. Patient follow-up after the end of antimicrobial therapy was at least 3 mo to capture SAB relapse, mortality, and cause of death. Patients were considered to be cured if no symptoms or signs of infection were present 3 mo after the discontinuation of antibiotic treatment. Relapse of SAB was defined as a second episode of SAB within 3 mo after the end of treatment.
18F-FDG PET/CT and Treatment Modifications
The impact of 18F-FDG PET/CT on treatment was determined by the investigators for all cases in a 2-step approach. First, treatment duration was determined on the basis of all clinical information available before 18F-FDG PET/CT was performed. Second, the results of the 18F-FDG PET/CT were provided, and the modifications of therapy based on these results were noted. During a weekly multidisciplinary meeting, all results of 18F-FDG PET/CT scans obtained in patients with SAB were discussed with a panel of ID specialists and nuclear medicine physicians and treatment modifications based on these results were also noted in the patient’s chart.
The impact of 18F-FDG PET/CT on treatment was classified as follows. The first was extension of antibiotic treatment including prolonged intravenous antibiotic therapy, for example, instead of oral antibiotic therapy; addition of a second antimicrobial drug, for example, rifampin, in patients with foreign body material infection; or extension of total treatment duration, for example, in the case of joint or vascular prosthesis infection. The second classification was surgical or radiologic intervention, for example, abscess drainage, removal of foreign body material. The third classification was shortening of treatment duration. If the results of the 18F-FDG PET/CT did not result in any intervention, this was also reported. To prevent interpretation bias, 2 independent physician observers reviewed hospitalization records and determined treatment modification before and after 18F-FDG PET/CT results. If there was no consensus, a third independent ID specialist with broad experience in SAB and 18F-FDG PET/CT made the final judgment. In patients with high-risk SAB, a comparison was made between patients who underwent 18F-FDG PET/CT and patients who did not.
Statistical Analysis
SPSS (version 22.0; SPSS, Inc.) was used for analyzing data. Descriptive statistics for continuous variables were represented as median ± SD. Unpaired Student t tests were used to compare continuous variables. Categoric variables were compared by use of the χ2 test or Fisher exact test when the χ2 test was not appropriate. Differences were considered to be statistically significant at a 2-sided P value of less than 0.05. To determine independent predictors of 3-mo mortality in the high-risk bacteremia group, we performed a multivariate analysis, including prognostic factors associated with a P value of less than 0.20 in univariate analysis. To limit the amount of variables in the model, the Charlson comorbidity score was used as a composite variable for age and comorbidity. As a composite variable for risk factors for metastatic infection, a risk score previously described by Fowler et al. (3) was used; community-acquisition, persistent fever longer than 72 h, and skin findings suggesting the presence of metastatic infection were separately scored as 1 point, and positive follow-up blood culture results were scored as 2 points.
RESULTS
During the study period, 195 events of SAB were identified. A total of 11 patients (5.6%) were excluded: 6 patients died within 48 h, and 5 patients were lost to follow-up. A total of 184 patients were included in the final analysis. Of these, 148 (80.0%) had 1 risk factor or more for metastatic infection and were classified as high-risk SAB. 18F-FDG PET/CT was performed in 99 of 148 (66.9%) high-risk SAB cases. In addition, 18F-FDG PET/CT was performed in 6 of 36 (16.7%) patients without risk factors for metastatic infection.
Definite endocarditis according to the modified Duke criteria was diagnosed in 16 patients (8.7%). Forty-six patients (25.0%) were admitted to the intensive care unit within 24 h before and 1 wk after SAB onset. Of 184 S. aureus strains isolated, only 5 (2.7%) were methicillin-resistant. Central venous catheter infection was considered responsible for 35 episodes (19.0%) of SAB. Baseline characteristics of all patients with and without 18F-FDG PET/CT are shown in Table 1.
Baseline Characteristics of All 184 Patients with SAB
Detection of Metastatic Infection by 18F-FDG PET/CT
18F-FDG PET/CT was performed in 105 of 184 study patients at a median of 8.0 d (mean, 8.7 d) after the first blood culture became positive. In 5 of 6 patients without risk factors for metastatic infection in whom 18F-FDG PET/CT was performed, no metastatic infection was found on 18F-FDG PET/CT. In 1 patient with a history of portal vein thrombosis, without risk factors for metastatic infection and removal of a central venous catheter 1 d after positive blood cultures, 18F-FDG PET/CT was performed and detected septic thrombophlebitis. This patient received intravenous antibiotic treatment for 6 wk. 18F-FDG PET/CT detected metastatic infectious foci in 73 of 99 patients with high-risk bacteremia (73.7%). In 52 of these 73 patients (71.2%) eventually diagnosed with metastatic infection, no signs and symptoms suggesting metastatic complications were present before 18F-FDG PET/CT was performed. Metastatic infection was most often diagnosed in the lungs, skin, and soft tissue, and as osteoarticular foci (Table 2). Of all 73 patients with metastatic infection, 47 patients (64.4%) were diagnosed with metastatic foci in more than 1 organ system. Eighteen patients had increased 18F-FDG uptake in a cardiac valve suspected for endocarditis, of whom 5 had a definite endocarditis according to the modified Duke criteria, 10 had a possible endocarditis, and in 3 patients the diagnosis of endocarditis was rejected.
Localization of Metastatic Foci and Number of Foci First Detected by 18F-FDG PET/CT in 99 High-Risk SAB Patients
Patient Outcome
The relapse rate 3 mo after treatment discontinuation was 2.2% (4/184). Overall 3-mo mortality was 18.5% (34/184). In the univariate analysis, age (59 vs. 69 y, P < 0.05), intensive care admission (22.0% vs. 38.2%, P < 0.05), Charlson comorbidity score (4.3 vs. 6.5, P < 0.05), and no 18F-FDG PET/CT performed (38.0% vs. 64.7%, P = 0.005) were significantly different between survivors and nonsurvivors.
Patients with Risk Factors for Metastatic Infection
The group with a risk factor for metastatic infection who did not undergo 18F-FDG PET/CT (risk+/PET−) was compared with the group of patients with a risk factor for metastatic infection and an 18F-FDG PET/CT performed (risk+/PET+) (Table 3). In patients with risk factors for metastatic infection in whom 18F-FDG PET/CT was performed, 3-mo mortality was significantly lower than in the risk+/PET− group (12.1% vs. 32.7%, P = 0.003). Multivariate analysis of risk factors for 3-mo mortality in the high-risk group is shown in Table 4. 18F-FDG PET/CT was the only factor that was significantly associated with reduced mortality (P = 0.005; odds ratio, 0.204; 95% confidence interval, 0.066–0.624). A higher comorbidity score was significantly associated with increased mortality (P = 0.003; odds ratio, 1.254; 95% confidence interval, 1.078–1.457).
Characteristics of Patients with 1 or More Risk Factors for Metastatic Infection in Whom 18F-FDG PET/CT Was Performed (PET+) or Not (PET−)
Univariate and Multivariate Analysis of Risk Factors for 3-Month Mortality in Patients with 1 or More Risk Factors for Metastatic Infection (n = 148)
Treatment Modifications in High-Risk Patients
In the 99 patients with high-risk SAB who underwent 18F-FDG PET/CT, 104 treatment modifications were made in 74 patients (74.7%) after the results of 18F-FDG PET/CT became available (Table 5). In 22 patients (22.2%), more than 1 treatment modification was made. In 25 patients (25.3%), treatment duration was shortened because no metastatic infection was detected. In 15 patients (15.2%), intravenous antibiotic therapy was prolonged on the basis of the 18F-FDG PET/CT results, in 10 patients (10.1%) a second antimicrobial drug was prescribed, and in 35 patients (35.4%) the total treatment duration was extended. In most cases, treatment was extended because of bone or joint involvement (22.2%), vascular prosthesis infection (19.4%), or other endovascular infection (17%). Percutaneous or surgical drainage was performed in 19 patients (19.2%) on the basis of the outcome of 18F-FDG PET/CT (Figs. 1 and 2). No treatment modification was made in 25 patients (25.3%) (Table 5).
Treatment Modifications in 99 Patients with High-Risk SAB Based on 18F-FDG PET/CT Results
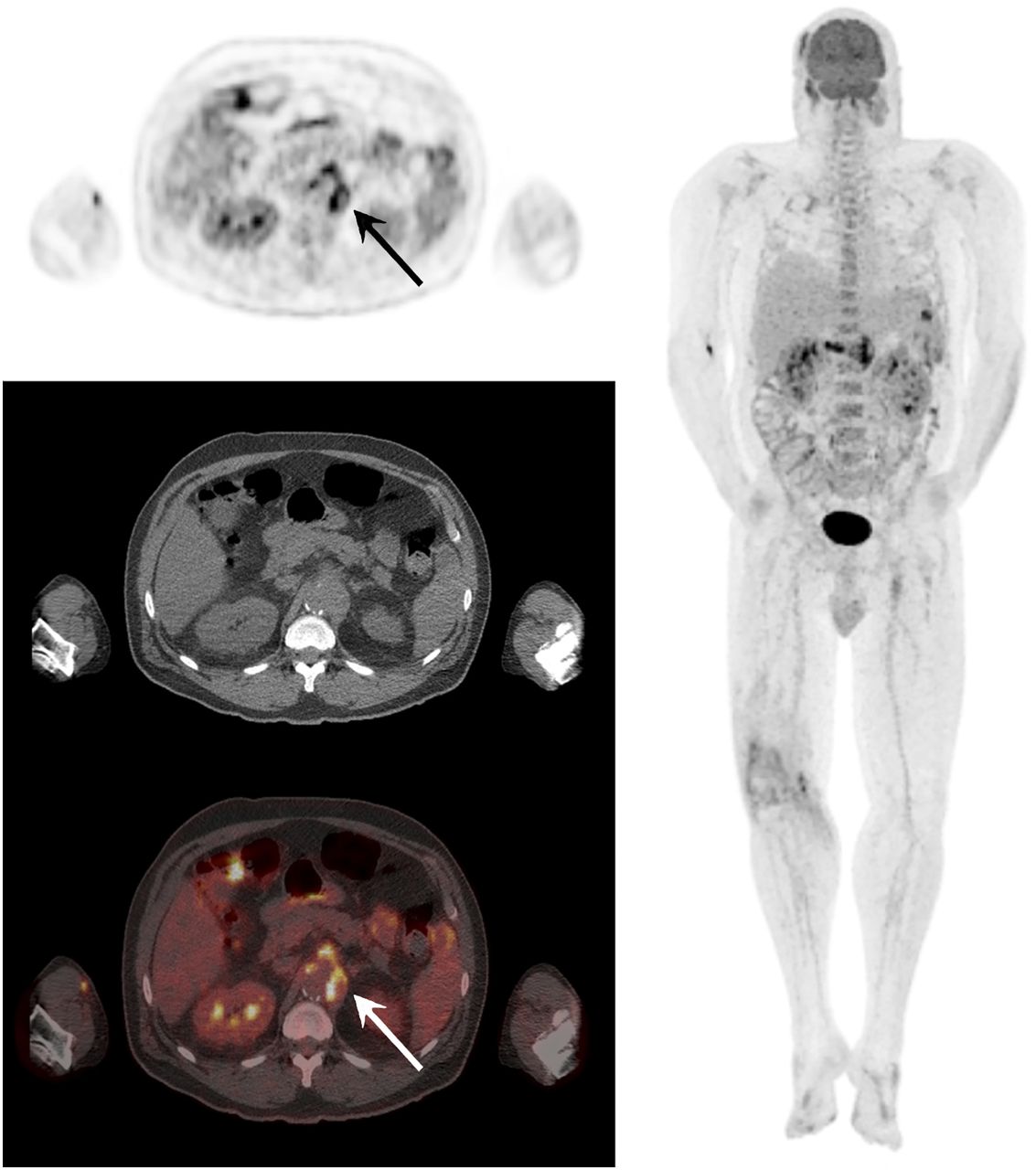
Transverse 18F-FDG PET/CT images at level of celiac trunk (left) and maximum-intensity-projection image (right) of 60-y-old man who was admitted because of septic arthritis of his right knee. Blood cultures grew methicillin-susceptible S. aureus. Transesophageal echocardiography was negative for endocarditis. Besides an arthritis of his right knee, 18F-FDG PET/CT also showed a mycotic aneurysm of celiac trunk (arrows) and multiple small abscesses in liver and spleen. This patient underwent a surgical repair of celiac trunk and was successfully treated with flucloxacillin intravenously for 6 wk after surgery.
18F-FDG PET/CT images of 84-y-old woman with right-sided closed humerus fracture after a fall. Two weeks later, she developed arthritis of her left metacarpophalangeal joints and blood cultures were positive for methicillin-susceptible S. aureus. Transesophageal echocardiography was negative for endocarditis. Besides arthritis of her left metacarpophalangeal joints, 18F-FDG PET/CT also showed metastatic infection in her right hip prosthesis, left ankle, right humerus with surrounding abscesses, and lumbar spine (L4–L5) with a right psoas abscess. This patient underwent CT-guided drainage of psoas abscess and was treated with cephazolin, because of allergy to flucloxacillin.
Of all patients with a planned treatment duration of 6 wk or more before 18F-FDG PET/CT was performed, 1 or more treatment modifications were performed in 23 of 46 patients (50.0%) on the basis of 18F-FDG PET/CT results (Fig. 3), compared with 51 of 53 (96.2%) in the group with a planned treatment duration of less than 6 wk.

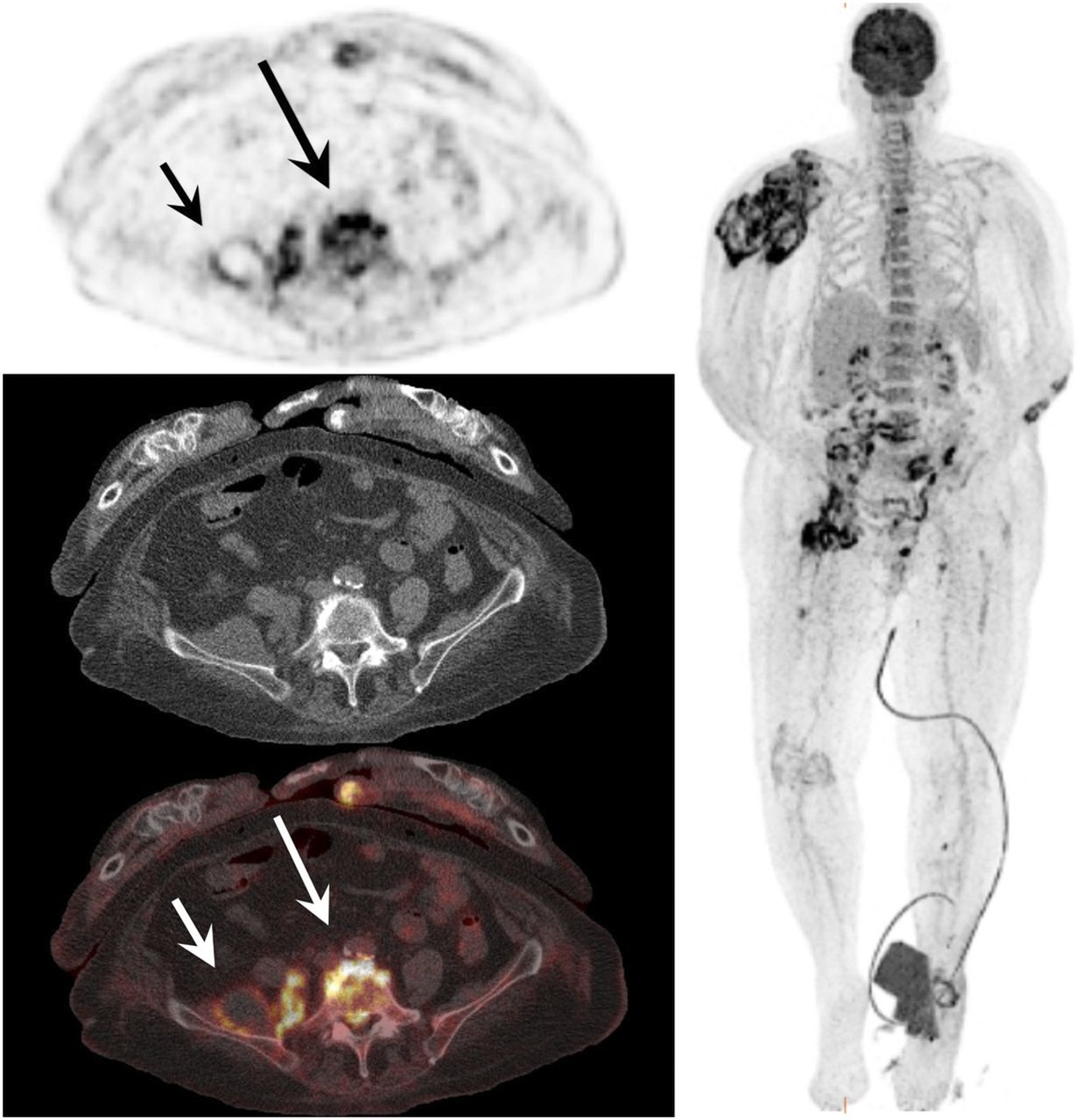
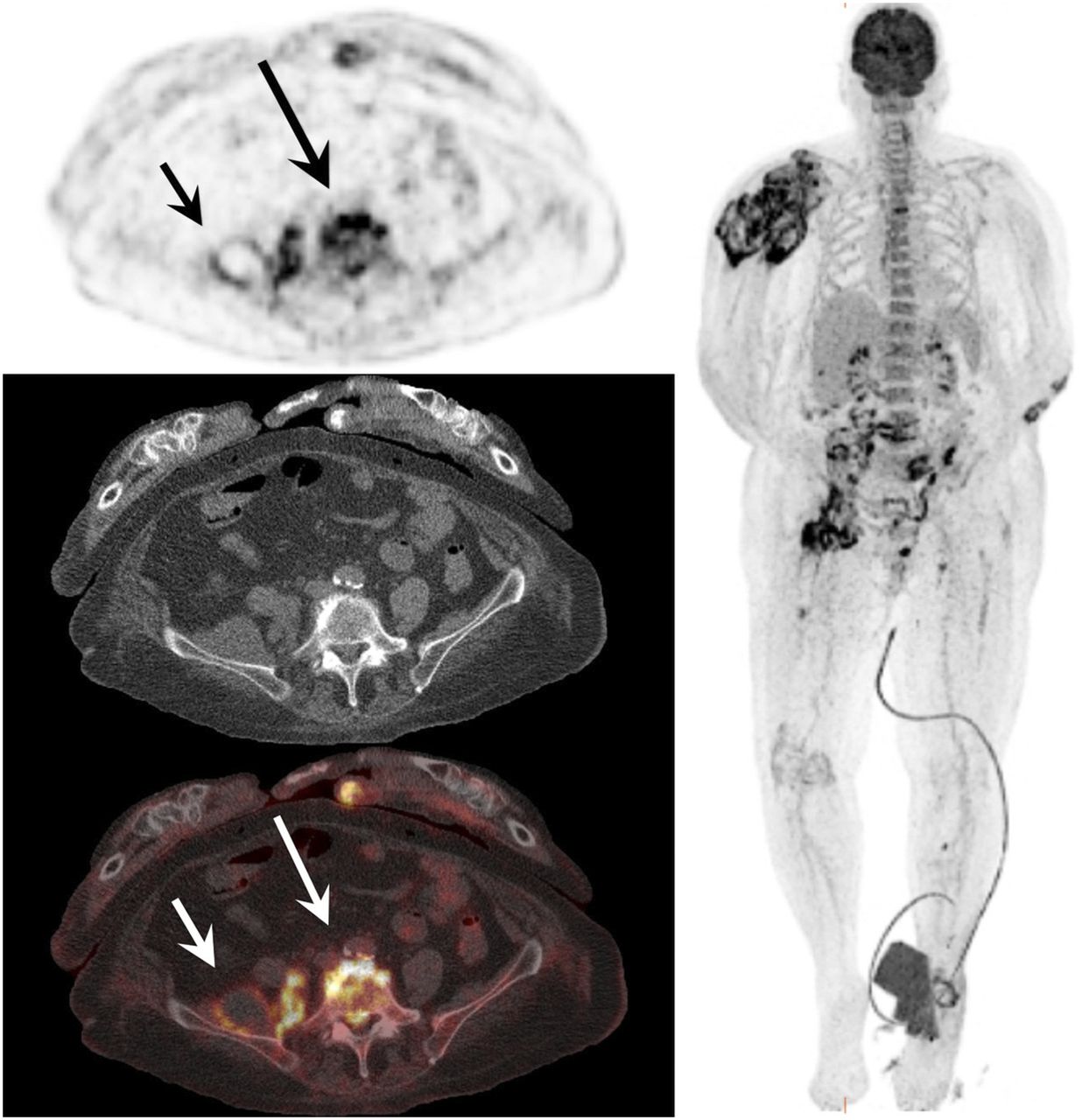
18F-FDG PET/CT images in combination with contrast-enhanced CT images (lower left) of 75-y-old man with medical history of chronic obstructive pulmonary disease, right femoropopliteal bypass, and aortobifemoral bypass who was admitted because of fever. Blood cultures were positive for methicillin-susceptible S. aureus. Transesophageal echocardiography was negative for endocarditis. 18F-FDG PET/CT showed infected right iliac vascular prosthesis. This patient was treated with antibiotic therapy for 5 mo, and because of extensive infection he finally underwent vascular surgery.
The following relevant diseases not related to SAB were diagnosed in 7 patients (7.1%): pulmonary carcinoma, mediastinal carcinoid tumor, recurrent adenocarcinoma of the rectum, recurrent vaginal carcinoma, benign thyroid adenoma, inflammatory bowel disease, and esophageal candidiasis. Irrelevant findings were found in 8 patients: in these patients 2 colonoscopies, 3 esophago-gastro-duodenoscopies, 3 ultrasounds, and 1 CT scan were obtained without a clear diagnosis.
DISCUSSION
In this study, we investigated the value of 18F-FDG PET/CT in patients with SAB for detecting metastatic infection and its role in treatment modification in these patients. In a previous prospective study on 115 patients with high-risk Gram-positive bacteremia (9), the addition of 18F-FDG PET/CT to standard care led to significantly more patients who were diagnosed with metastatic infection compared with a matched historical control group of 230 patients in whom no 18F-FDG PET/CT was performed (67.8% vs. 35.7% in the control group). Furthermore, 6-mo mortality rate decreased from 32.2% to 19.1% when 18F-FDG PET/CT was performed. An explanation for the slightly higher detection level in our study (73.7%) could be the fact that metastatic infection is more often seen in SAB than in other types of Gram-positive bacteremia. Another study on the value of 18F-FDG PET/CT for the diagnosis of metastatic infection in 47 patients with infectious endocarditis found that 18F-FDG PET/CT was associated with a 2-fold reduction in the number of relapses and 18F-FDG PET/CT enabled significantly more infectious complications to be diagnosed (57.4% vs. 18% in matched controls) (10). Orvin et al. (15) prospectively studied the value of 18F-FDG PET/CT in 40 consecutive patients with definite endocarditis according to the Duke criteria. 18F-FDG PET/CT demonstrated extracardiac complications in 17 patients (42.5%), and these findings led to a change of treatment in 14 patients (35%) while these patients already had an indication for prolonged antibiotic treatment because of endocarditis. This is comparable to our results, because treatment was still adapted in 50% of patients with an indication for prolonged treatment before 18F-FDG PET/CT was performed.
In the present study, the early detection of metastatic infectious foci facilitated the adaptation of treatment in patients at high risk of relapse. The 3-mo relapse rate was only 2.2%, which is low compared with the rates reported in the literature for complicated SAB (2.1%–23%) (16). An important finding of the present study is that patients with risk factors for metastatic infection who did not undergo 18F-FDG PET/CT had a significantly higher mortality rate than those who underwent 18F-FDG PET/CT (32.7% vs. 12.1%, P = 0.003), even though the average number of risk factors for metastatic infection in the latter group was higher. This emphasizes the importance of the risk assessment for metastatic infection and suggests that physicians should not refrain from ordering 18F-FDG PET/CT with high-risk SAB based on personal judgment. Early death may be hypothesized to be a confounding factor, because those patients were unable to undergo 18F-FDG PET/CT. However, in a sensitivity analysis excluding patients who died within 7 d after admission, the results regarding 3-mo mortality were similar. Another potential confounder could be the difference in ID specialist consultation, because ID consults have been associated with reduced mortality in patients with SAB (5,17–21). However, multivariate logistic regression analysis did not show this to be an independent predictor of survival, probably due to the high frequency of ID consultation in both groups in the present study. In our study, 18F-FDG PET/CT detected endocarditis in 18 patients and was the first imaging technique detecting endocarditis in 11 patients. In contrast, 8 patients were diagnosed with a definite endocarditis according to the modified Duke criteria but had a negative 18F-FDG PET/CT result. Whether 18F-FDG PET/CT could be used for diagnosing native valve endocarditis needs further investigation, because small studies performed on this subject show limited evidence (22).
Our study has several limitations. First, this is a single-center study that was not prospectively conducted. In 26.6% of patients, 18F-FDG PET/CT was indicated but not performed. The reasons for nonadherence to the local guidelines are not known, and this could potentially have led to selection bias. Second, although we used a 2-reviewer adjudication process to determine treatment modification, it is possible that misclassification occurred. To reduce bias, the 2 reviewers were masked from each other and disagreements were resolved by a third experienced reviewer.
CONCLUSION
The performance of 18F-FDG PET/CT is significantly associated with reduced mortality in patients with high-risk SAB and leads to the detection of metastatic infectious foci in 73.7% of patients, resulting in important treatment modifications. 18F-FDG PET/CT should be recommended as a standard imaging technique for all patients with 1 or more risk factors for metastatic infection in SAB guidelines.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
↵* Contributed equally to this work.
Published online Mar. 23, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication February 17, 2017.
- Accepted for publication March 13, 2017.





{kind=link}
{kind=link}
{kind=link}