


Abstract
This work aimed at estimating the kinetic parameters, and hence cumulated activity (AC), of a diagnostic/therapeutic convergence radiopharmaceutical, namely 64Cu-/177Lu-labeled antibody (64Cu-/177Lu-cetuximab), that acts as anti–epidermal growth factor receptor. Methods: In mice bearing esophageal squamous cell carcinoma tumors, to estimate uptake (K), release rate constant (kR), and hence AC, a kinetic model analysis was applied to recently published biodistribution data of immuno-PET imaging with 64Cu-cetuximab and of small-animal SPECT/CT imaging with 177Lu-cetuximab, including blood and TE-8 tumor. Results: K, kR, and AC were estimated to be 0.0566/0.0593 g⋅h−1⋅g−1, 0.0150/0.0030 h−1, and 2.3 × 1010/4.1 × 1012 disintegrations (per gram of TE-8 tumor), with an injected activity of 3.70/12.95 MBq, for 64Cu-/177Lu-cetuximab, respectively. Conclusion: A model is available for comparing kinetic parameters and AC of the companion diagnostic/therapeutic 64Cu-/177Lu-cetuximab that may be considered as a step for determining whether one can really use the former to predict dosimetry of the latter.
Theragnostics strategy relies on noninvasive quantitative immuno-PET to select patients eligible for radioimmunotherapy. In this framework, Song et al. recently investigated a companion diagnostic/therapeutic radiopharmaceutical acting as anti–epidermal growth factor receptor (EGFR) antibody that was prepared via identical chelator, 3,6,9,15-tetraazabicyclo[9.3.1]-pentadeca-1(15),11,13-trience-3,6,9,-triacetic acid (PCTA), labeled with 64Cu or 177Lu (64Cu-/177Lu-PCTA-cetuximab) (1). This compound was designed for assessing EGFR expression level in esophageal squamous cell carcinoma (ESCC) tumors as well as for subsequent radioimmunotherapy. Any advance in this field is of major interest because innovative therapeutic strategies are actually needed in ESCC patients. In ESCC tumor–bearing mice, the authors reported biodistribution data from immuno-PET imaging with 64Cu-cetuximab and small-animal SPECT/CT imaging with 177Lu-cetuximab, including blood (i.e., the tracer input function [IF]) and TE-8 tumor.
We suggest that further information can be derived from Song et al.’s results, which may prove of interest to comprehensively characterize this novel companion diagnostic/therapeutic radiopharmaceutical. Thus, the aim of this work was to estimate uptake (K), release rate constant (kR), and hence cumulated activity (AC)—that is, the number of disintegrations per gram of TE-8 tissue that have occurred from the time of tracer administration (zero) to (theoretically) infinity, after administration of 64Cu-cetuximab and 177Lu-cetuximab for immuno-PET and small-animal SPECT/CT imaging, respectively. To this end, a simple model derived from a previously published kinetic model analysis was used (2,3). Furthermore, this study addresses the issue of determining whether 64Cu-cetuximab imaging might predict 177Lu-cetuximab AC, and hence its dosimetry, in a real clinical situation.
MATERIALS AND METHODS
A previously published formula was used for estimating AC (expressed per gram of TE-8 tissue, in g−1), including K and kR (3): Eq. 1where AUCIF is the area under the curve of the tracer IF (i.e., total number of disintegrations per gram of blood that have occurred from the time of tracer administration to infinity, in g−1). AC can be derived from mean blood data obtained by Song et al. in a TE-8 tumor model at 2, 24, 48, and 72 h after injection for 64Cu-cetuximab: 20.5, 6.4, 4.4, and 2.5 %ID/g (percentage injected radioactivity dose per gram of tissue; Supplemental Table 1 in Song et al. (1)). For 177Lu-cetuximab, mean blood data obtained in a TE-8 tumor model at 2, 24, 72, and 120 h after injection were used: 30.2, 12.1, 6.0, and 3.1 %ID/g (Supplemental Table 2 in Song et al. (1)). First, the decay correction of Song et al.’s data was removed—that is, the data were multiplied by exp(− λ t), where λ is the 64Cu/177Lu physical decay constant (i.e., Ln2/12.7 and Ln2/160 h−1, respectively). Then, data were fitted with a monoexponential decreasing function (time constant α, in h−1):
Eq. 1where AUCIF is the area under the curve of the tracer IF (i.e., total number of disintegrations per gram of blood that have occurred from the time of tracer administration to infinity, in g−1). AC can be derived from mean blood data obtained by Song et al. in a TE-8 tumor model at 2, 24, 48, and 72 h after injection for 64Cu-cetuximab: 20.5, 6.4, 4.4, and 2.5 %ID/g (percentage injected radioactivity dose per gram of tissue; Supplemental Table 1 in Song et al. (1)). For 177Lu-cetuximab, mean blood data obtained in a TE-8 tumor model at 2, 24, 72, and 120 h after injection were used: 30.2, 12.1, 6.0, and 3.1 %ID/g (Supplemental Table 2 in Song et al. (1)). First, the decay correction of Song et al.’s data was removed—that is, the data were multiplied by exp(− λ t), where λ is the 64Cu/177Lu physical decay constant (i.e., Ln2/12.7 and Ln2/160 h−1, respectively). Then, data were fitted with a monoexponential decreasing function (time constant α, in h−1): Eq. 2where Ab(t = 0) is expressed in %ID/g. In Equation 1, AUCIF is simply Ab(t = 0)/α.
Eq. 2where Ab(t = 0) is expressed in %ID/g. In Equation 1, AUCIF is simply Ab(t = 0)/α.
The constant kR (h−1) appearing in Equation 1 can be estimated from the following formula that applies to both PET and SPECT tracer (2): Eq. 3where tmax is the uptake peak of the TE-8 tumor time–activity-curve, as published by Song et al. (i.e., involving decay correction): tmax = 48 and 120 h for 64Cu-cetuximab and 77Lu-cetuximab, respectively (1). Equation 3 can be solved for kR using a solver (Excel; Microsoft).
Eq. 3where tmax is the uptake peak of the TE-8 tumor time–activity-curve, as published by Song et al. (i.e., involving decay correction): tmax = 48 and 120 h for 64Cu-cetuximab and 77Lu-cetuximab, respectively (1). Equation 3 can be solved for kR using a solver (Excel; Microsoft).
The constant K (g. h−1.g−1) appearing in Equation 1 can be estimated from the following formula involving trapped tracer activity in TE-8 tumor, ATrap(t) (2): Eq. 4Mean tissue data published by Song et al. for ATrap(t) in a TE-8 tumor were used: 17.5 and 55.7 %ID/g at t = 48 and 120 h for 64Cu-cetuximab and 177Lu-cetuximab, respectively (Supplemental Tables 1 and 2 in Song et al. (1)). The decay correction of these data was removed—that is, they were multiplied by exp(−λ × t) where λ is the 64Cu/177Lu physical decay constant. Note that Equation 4 does not involve free tracer in blood and interstitial volume, because the part of free tracer becomes negligible in comparison to trapped tracer at late imaging. Indeed, the value of F × Ab(t) (with F < < 1; no unit) is much lower than that of ATrap(t) at t = 48 and 120 h for 64Cu-cetuximab and 177Lu-cetuximab, respectively (Fig. 1) (2,3).
Eq. 4Mean tissue data published by Song et al. for ATrap(t) in a TE-8 tumor were used: 17.5 and 55.7 %ID/g at t = 48 and 120 h for 64Cu-cetuximab and 177Lu-cetuximab, respectively (Supplemental Tables 1 and 2 in Song et al. (1)). The decay correction of these data was removed—that is, they were multiplied by exp(−λ × t) where λ is the 64Cu/177Lu physical decay constant. Note that Equation 4 does not involve free tracer in blood and interstitial volume, because the part of free tracer becomes negligible in comparison to trapped tracer at late imaging. Indeed, the value of F × Ab(t) (with F < < 1; no unit) is much lower than that of ATrap(t) at t = 48 and 120 h for 64Cu-cetuximab and 177Lu-cetuximab, respectively (Fig. 1) (2,3).
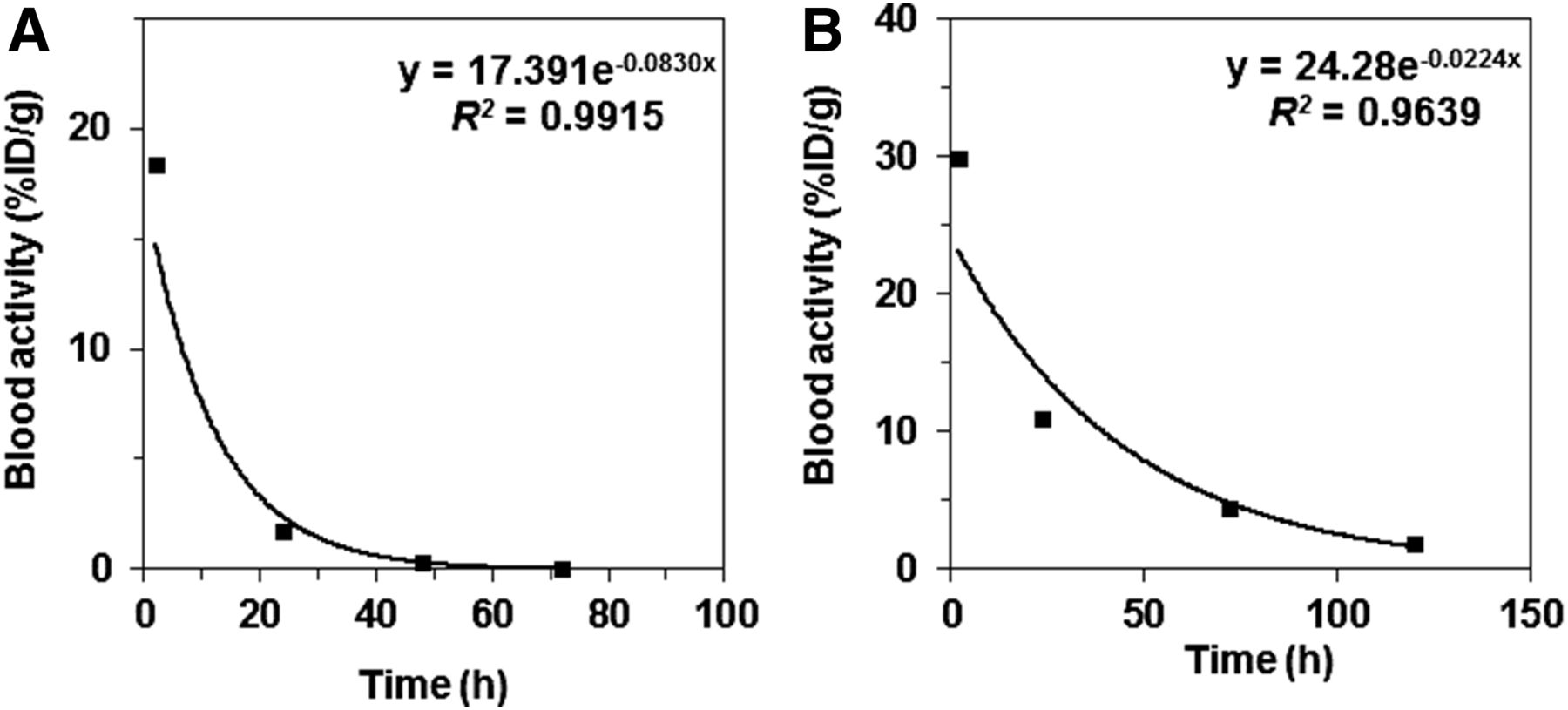
Decreasing monoexponential fitting of IF: 64Cu-cetuximab (P < 0.01) (A) and 177Lu-cetuximab (P < 0.02) (B).
AC can also be calculated from original data (after decay correction is removed) published by Song et al. for 64Cu-cetuximab and 177Lu-cetuximab in a TE-8 tumor model, respectively (Supplemental Tables 1 and 2 in Song et al. (1)). A crude estimate of AC can be obtained by trapezoidal integration and assuming a simple radioactive decay after the last data point.
RESULTS
From Song et al.’s data in a TE-8 model (Supplemental Tables 1 and 2 in Song et al. (1)), α (uncorrected for physical decay) was estimated to be 0.0830 h−1 for 64Cu-cetuximab and 0.0224 h−1 for 177Lu-cetuximab (Fig. 1, Eq. 2: R = 0.99–0.98; P < 0.01–0.02) (1). Numeric solving of Equation 3 provided the following estimate of kR: 0.0150 and 0.0030 h−1 for 64Cu- and 177Lu-cetuximab, respectively. From Equation 4, K was estimated to be 0.0566/0.0593 g⋅h−1⋅g−1 for 64Cu-/177Lu-cetuximab, respectively. Then, from Equation 1, AC was estimated to be 2.3 × 1010 and 4.1 × 1012 disintegrations per gram of TE-8 tumor, with an injected activity of 3.70 and 12.95 MBq and K/(λ + kR) ratio of 0.8 and 8.1, for 64Cu-cetuximab and 177Lu-cetuximab, respectively.
For comparison, AC obtained by trapezoidal integration of Song et al.’s TE-8 tumor data and assuming a simple radioactive decay after the last data point was estimated to be 2.5 × 1010 and 5.3 × 1012 disintegrations per gram of TE-8 tumor, for 64Cu-cetuximab and 177Lu-cetuximab, respectively.
DISCUSSION
This theoretic work aimed at providing further quantitative information, including AC, regarding the companion diagnostic/therapeutic 64Cu-/177Lu-cetuximab from recently published biodistribution data in ESCC tumor–bearing mice. A simple model derived from a published kinetic model analysis was used, allowing us to obtain estimates of K, kR, and hence AC for 64Cu-cetuximab and 177Lu-cetuximab (2,3).
The uptake rate constants of 64Cu-/177Lu-cetuximab were found to be close: K = 0.0566/0.0593 g⋅h−1⋅g−1, respectively. In other words, labeling cetuximab with either 64Cu or 177Lu does not influence its trapping in TE-8 tumors. K actually represents the probability that a 64Cu-/177Lu-cetuximab molecule is trapped in the tissue of interest as the result of an antibody–antigen linking. It does not give any information about its further fate, such as internalization. The release rate constants of 64Cu-/177Lu-cetuximab were found to be low in comparison to K: kR = 0.0150/0.0030 h−1, respectively. kR actually represents the probability that a 64Cu-/177Lu-cetuximab molecule trapped in the tissue of interest is released from its target and returns back to blood. This probability should, additionally, take into account a possible internalization of the antibody–antigen complex that lowers it. Furthermore, we suggest that the 5-fold difference in kR reported for 64Cu-cetuximab versus 177Lu-cetuximab may be related to the fact that kR was estimated using peak time values assessed with a 24- to 48-h time of resolution for 64Cu-/177Lu-cetuximab, respectively (Eq. 3). This large time of resolution very likely introduces some uncertainty measurement for kR, especially because it is derived from a logarithmic equation (Eq. 3).
AC for 177Lu-cetuximab was found to be much greater than that for 64Cu-cetuximab: 4.1 × 1012 versus 2.3 × 1010 disintegrations per gram of TE-8 tumor. This result is strengthened by the crude estimates for AC provided by trapezoidal integration of Song et al.’s original data and assuming a simple radioactive decay after the last data point: AC = 5.3 × 1012 versus 2.5 × 1010 disintegrations per gram of TE-8 tumor, for 177Lu-cetuximab versus 64Cu-cetuximab, respectively. Note that the injected activity was greater for 177Lu-cetuximab than for 64Cu-cetuximab: 12.95 versus 3.70 MBq. However, the difference in AC may also be explained from Equation 1, showing that for close values of K and kR, the lower the value of α and λ the greater that of AC. It does emphasize the efficiency of radioimmunotherapy with 177Lu-cetuximab investigated in ESCC tumor–bearing mice, and we suggest that the reliable IF fitting as a monoexponential decreasing function (Fig. 1B; R = 0.98; P < 0.02) is particularly relevant for assessing its dosimetry (Eq. 1). Furthermore, one may argue that Equation 1 does not take into account the part of free tracer in blood and interstitial volume (F) in the AC calculation (3). However, we suggest that this part, and hence the related AC underestimation, is negligible: F is indeed mandatorily much lower than 1, which has to be compared with the ratio K/(λ + kR) whose value is 8.1 for 177Lu-cetuximab.
Regarding the issue of determining whether 64Cu-cetuximab imaging might predict177Lu-cetuximab AC, and hence its dosimetry, in real clinical situations, the current study showed that AC for 64Cu-cetuximab may be obtained from the computed value of kR at uptake peak and the corresponding uptake value (Eqs. 1, 3, and 4). Thus, theoretically, if an average AC ratio between 64Cu-cetuximab and 177Lu-cetuximab has been obtained from previous experiments (with arbitrary injected activities), an estimate for 177Lu-cetuximab AC may be obtained from a single quantitative imaging session with 64Cu-cetuximab. However, a main concern about this line of argument must be underlined, which is related to performing PET imaging at uptake peak of 64Cu-cetuximab (Eq. 3). Indeed, even if the 64Cu-cetuximab IF is known in each individual (i.e., the value of α in Eq. 3), the relevant time delay between 64Cu-cetuximab injection and PET acquisition cannot be predicted in each individual, because, precisely, kR is unknown. Therefore, we suggest that additional experiments, involving lower times of resolution than those reported by Song et al., are required for knowledge of the kR range in a large series of individuals that can also provide the range of the AC ratio between 64Cu-cetuximab and 177Lu-cetuximab (for arbitrary injected activities). If kR is found to vary within narrow limits for 64Cu-cetuximab, the uptake-peak timing might be approximately predicted in each individual and, even, an average kR value might be used for 64Cu-cetuximab AC calculation. Furthermore, the AC ratio between 64Cu-cetuximab and 177Lu-cetuximab should also vary within narrow limits for deriving 177Lu-cetuximab AC. In other words, additional experiments are required to determine whether the measurement uncertainty of the 177Lu-cetuximab AC is acceptable or not. Finally, whatever results obtained in a preclinical model, some adjustment is required in humans.
CONCLUSION
The study of Song et al. showed that the companion diagnostic/therapeutic radiopharmaceutical, namely 64Cu-/177Lu-cetuximab, may be useful as a diagnostic tool for patient selection as well as a potent radioimmunotherapy agent (1). As further evidence, although complexation and catabolism of copper and lutetium may be quite different, the current study showed that the uptake rate constants of 64Cu-cetuximab and 177Lu-cetuximab are close, and their release rate constants are low in comparison with the uptake rate constants. Moreover, because of a longer physical half-life of 177Lu than 64Cu, a longer IF life time of 177Lu-cetuximab than 64Cu-cetuximab, and a greater injected activity of 177Lu-cetuximab than 64Cu-cetuximab (12.95 vs. 3.70 MBq in Song et al.’s experiments), AC of 177Lu-cetuximab was found to be much greater (2 orders of magnitude in the current framework) than that of 64Cu-cetuximab. However, the current study may be considered as a step for determining whether 64Cu-cetuximab imaging might reliably predict dosimetry with 177Lu-cetuximab in real clinical situations. This major issue requires additional experiments in preclinical models, of which results should be then tested in humans.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 12, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
- Received for publication July 1, 2016.
- Accepted for publication October 31, 2016.





{kind=link}