


Abstract
Metabolic and molecular imaging continues to advance our understanding of vascular disease pathophysiology. At present, 18F-FDG PET imaging is the most widely used clinical tool for metabolic and molecular imaging of atherosclerosis. However, novel nuclear tracers and intravascular optical near-infrared fluorescence imaging catheters are emerging to assess new biologic targets in vivo and in coronary arteries. This review highlights current metabolic and molecular imaging clinical and near-clinical applications within atherosclerosis and venous thromboembolism, and explores the potential for metabolic and molecular imaging to affect patient-level risk prediction and disease treatment.
Prediction is very difficult, especially if it's about the future.
—Niels Bohr
In this focused review, we showcase state-of-the-art molecular imaging applications to atherosclerosis and venous thromboembolism (VTE). Clinical or near-clinical applications will be highlighted, illuminating how molecular imaging can provide insights into disease pathophysiology, risk prediction, and management.
ATHEROSCLEROSIS
Background
Atherosclerosis is the primary cause of heart attack, stroke, and limb ischemia and remains a leading cause of death worldwide. Clinical atherosclerosis imaging traditionally assesses anatomic measures such as luminal stenosis. However, imaging of structural features provides limited insights into the pathobiology central to atherosclerosis disease progression, which is a biologic consequence of accumulated inflammatory cells and oxidized lipids within the vessel wall. Molecular imaging is a complementary approach that provides new insights into mechanisms of atherosclerosis progression and complications. For larger arteries (carotid, iliac, aorta), 18F-FDG PET imaging currently predominates to detect plaque inflammatory cells (macrophages). In the smaller-sized coronary arteries, 18F-sodium fluoride (18F-NaF) PET and high-resolution intravascular near-infrared fluorescence (NIRF) molecular imaging are emerging new approaches to image plaque mineralization and inflammation (e.g., protease activity), respectively.
18F-FDG PET
In atherosclerosis, the most widely used PET tracer is 18F-FDG, a glucose analog consumed by metabolically active cells. 18F-FDG possesses a 110-min half-life and maximum 2.4-mm positron range. After phosphorylation, trapped intracellular 18F-FDG-6-phosphate cannot proceed down glycolytic pathways and accumulates in direct relation to the degree of cellular glycolysis, substantially reflecting plaque macrophage content.
Association with Cardiovascular Risk Factors and Prediction of Cardiovascular Events
Atherosclerosis 18F-FDG PET metabolic imaging is positioned to improve risk prediction beyond structural imaging measures, by predicting atheroma progression and subsequent clinical events, and to tailor atheroma pharmacotherapies.
Risk factors (e.g., smoking, diabetes mellitus, hyperlipidemia, hypertension) are established predictors of cardiovascular events on a population-based level. To assess relationships between cardiac risk factors and 18F-FDG PET, Noh et al. measured 18F-FDG carotid plaque uptake in 1,181 asymptomatic subjects, and correlated the results with 10-y Framingham risk score (FRS) (mean ± SD, 12.3% ± 8.7%, indicating intermediate risk) (1). The authors determined that an elevated carotid plaque 18F-FDG uptake (mean target-to-background ratio ≥ 1.7) increased the chance of having an elevated FRS of 10% or more (odds ratio, 1.9). 18F-FDG uptake has also been associated with other risk factors. One study explored the relationship between plaque inflammation (by 18F PET) and atherogenic lipoprotein(a) (Lp(a)), a proinflammatory oxidized phospholipid transporter associated with accelerated arterial inflammation. Compared with 30 matched subjects with normal Lp(a) levels, those with elevated Lp(a) manifested greater arterial inflammation (2).
Beyond risk factors, imaging arterial inflammation may provide direct insights into atherosclerosis progression. Cho et al. recently observed that aortic 18F-FDG PET uptake predicted the progression of coronary calcification at 1 y (3). In 96 subjects without known coronary disease or statin use, elevated aortic 18F-FDG uptake significantly associated with incident coronary calcification (odds ratio, 4.39; P = 0.007). Similarly, Abdelbaky et al. demonstrated that local 18F-FDG uptake predicts incident calcium deposition in the underlying atheroma (4).
More importantly, several retrospective studies have shown that aortic 18F-FDG uptake independently predicts cardiovascular disease (CVD) risk above the FRS (5), and evolving data support prospective 18F-FDG PET imaging. 18F-FDG PET carotid arterial inflammation independently predicted recurrent ipsilateral cerebrovascular events in 60 patients with recent stroke (6). Accordingly, 18F-FDG PET/CT arterial imaging may provide additive prognostic information beyond risk factor assessment and structural imaging data.
18F-FDG PET imaging has yielded insights into how adipose tissue, particularly visceral adiposity, associates with heightened cardiovascular risk. Figueroa et al. evaluated CT adipose tissue, 18F-FDG PET arterial inflammation, and cardiovascular events in 415 asymptomatic patients (mean body mass index, 26.4 kg/m2) (7). Visceral fat volume correlated positively with 18F-FDG inflammation (r = 0.290, P < 0.001). Over 4 y, the visceral fat volume associated with increased cardiovascular event risk (hazard ratio, 1.15, and P < 0.001; hazard ratio, 3.60, and P < 0.001, respectively). In a separate 443-patient study, 18F-FDG PET signal in plaques and brown adipose tissue, a metabolically active tissue present in childhood that regresses with age, demonstrated that brown fat 18F-FDG activity correlated negatively with 18F-FDG arterial inflammation (r = −0.147, P < 0.01) (8). Brown fat 18F-FDG uptake was further associated with improved cardiac event–free survival (P = 0.048). These data support the notion that visceral fat spurs arterial inflammation and subsequent events and that brown fat may be protective.
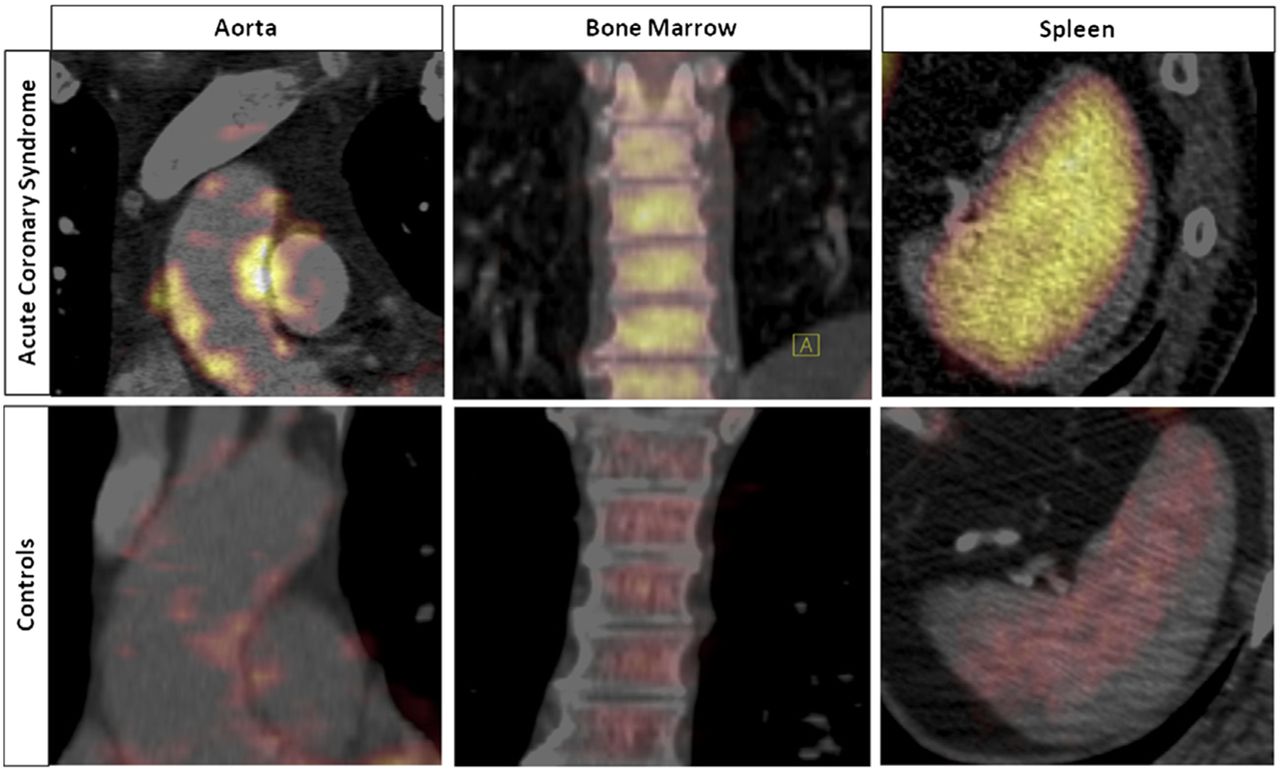
Patients with acute coronary syndrome (ACS) harbor a heightened risk of repeated cardiovascular events. Pathophysiologically, recent preclinical mechanistic studies support splenic and bone marrow (the cardiospenic axis) activation as mediators of activated leukocyte trafficking and subsequent atheroma progression. Emami et al. imaged 22 ACS patients, demonstrating increased 18F-FDG spleen uptake compared with non-ACS controls (Fig. 1; SUV, 2.6 ± 0.6 vs. 2.1 ± 0.3; P = 0.03) (9). A 464-patient substudy revealed that subjects with increased 18F-FDG splenic activity experienced more cardiac events (hazard ratio, 3.3; P = 0.003), even after adjustment for CVD risk factors. These results support the clinical importance of the cardiosplenic axis in humans, and motivate CVD preventative strategies against proinflammatory leukocyte emigration.

Evidence of cardiosplenic axis in ACS patients. 18F-FDG uptake is significantly increased in aortic wall (left), bone marrow (middle), and spleen (right) in ACS patients compared with controls. (Reprinted with permission of Emami et al. (9).)
New Clinical Disease Insights in Atherosclerosis
Plaque inflammation drives atherosclerosis progression and clinical events, as evidenced by heightened CVD in patients with inflammatory rheumatologic diseases. To examine this association, Naik et al. performed 18F-FDG PET in 60 psoriasis patients without known CVD and found that aortic 18F-FDG uptake increased proportionately to psoriasis disease severity, even after adjustment for age, sex, and calculated FRS (β = 0.41, P = 0.001) (10). A separate study of 38 familial hypercholesterolemia subjects who underwent serial 18F-FDG PET imaging at baseline (Fig. 2) and then 3 d later after lipoprotein apheresis was performed (11). Apheresis-based low-density lipoprotein reduction (284 ± 118 vs. 127 ± 50 mg/dL, P < 0.001) rapidly lowered arterial 18F-FDG activity (target-to-background ratio, 2.05 ± 0.31 before vs. 1.91 ± 0.33 after; P < 0.02). This intriguing data inform that atherogenic lipoprotein-induced arterial inflammation may be quickly reversible, supporting potent lipid therapy use in ACS.
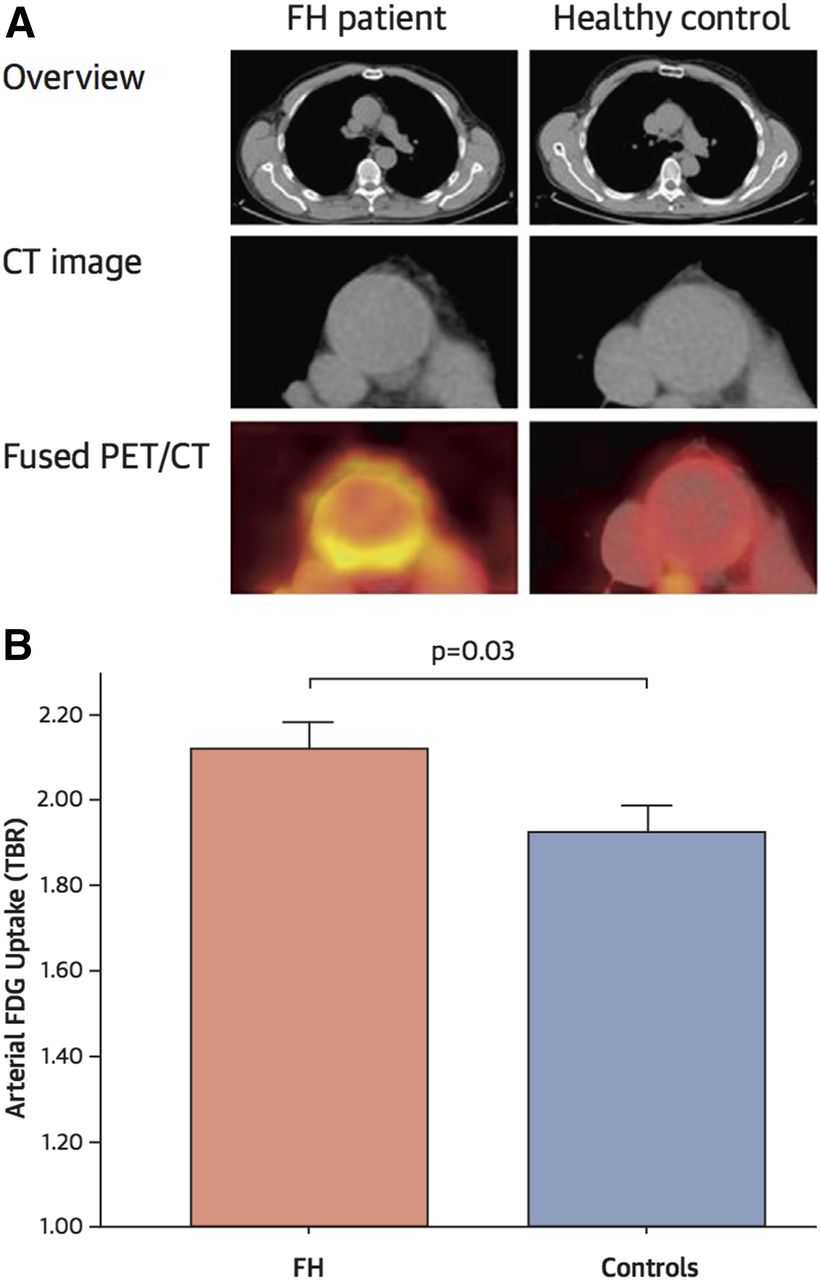
18F-FDG PET/CT inflammation imaging in familial hypercholesterolemia patients. (A) 18F-FDG uptake is elevated in the aorta of familial hypercholesterolemia subjects (left) compared with controls (right), as quantified by significantly higher mean arterial target-to-background ratio. FH = familial hypercholesterolemia; TBR = target-to-background ratio. (Reprinted with permission from van Wijk et al. (11).)
Evaluation of Antiatherosclerosis Pharmacotherapies
Because arterial inflammation remains an important pharmacotherapeutic target, several studies have recently harnessed 18F-FDG PET to assess the in vivo antiinflammatory effects of novel atherosclerosis pharmacotherapies. Thus far, there exist 5 compound classes where both clinical endpoint and PET imaging data are available. For 2 of these 5 drug classes (statins and thiazolidinediones), imaging and clinical endpoint trial results have been concordantly positive (12,13). On the other hand, for 3 of 5 drug classes (cholesteryl ester transfer protein inhibitor, lipoprotein-associated phospholipase A2 inhibitor, and P38 MAP kinase inhibitors), imaging and clinical endpoint trials have been concordantly neutral (14–18). Hence, thus far there appears to be concordance between directional changes in arterial imaging and clinical efficacy. Furthermore, 18F-FDG PET/CT trials are typically small (roughly 35–60 subjects per group) and fast (3- to 6-mo treatment intervals), and thus have the potential to presage pharmacotherapeutic efficacy in considerably longer and more expensive outcomes trials of several thousand individuals.
Intravascular NIRF Molecular Imaging
Intravascular NIRF is an emerging optical molecular imaging approach designed for high-resolution coronary arterial imaging. NIRF imaging uses injectable fluorescent imaging agents that target key cellular and molecular processes in vivo. Not only does near-infrared light (∼700–900 nm excitation) offer greater tissue penetration and reduced autofluorescence compared with visible light, but also NIRF imaging can be performed via coronary arterial-compatible catheters, and through blood without flushing. These attributes support intravascular NIRF as a viable coronary arterial molecular imaging method.
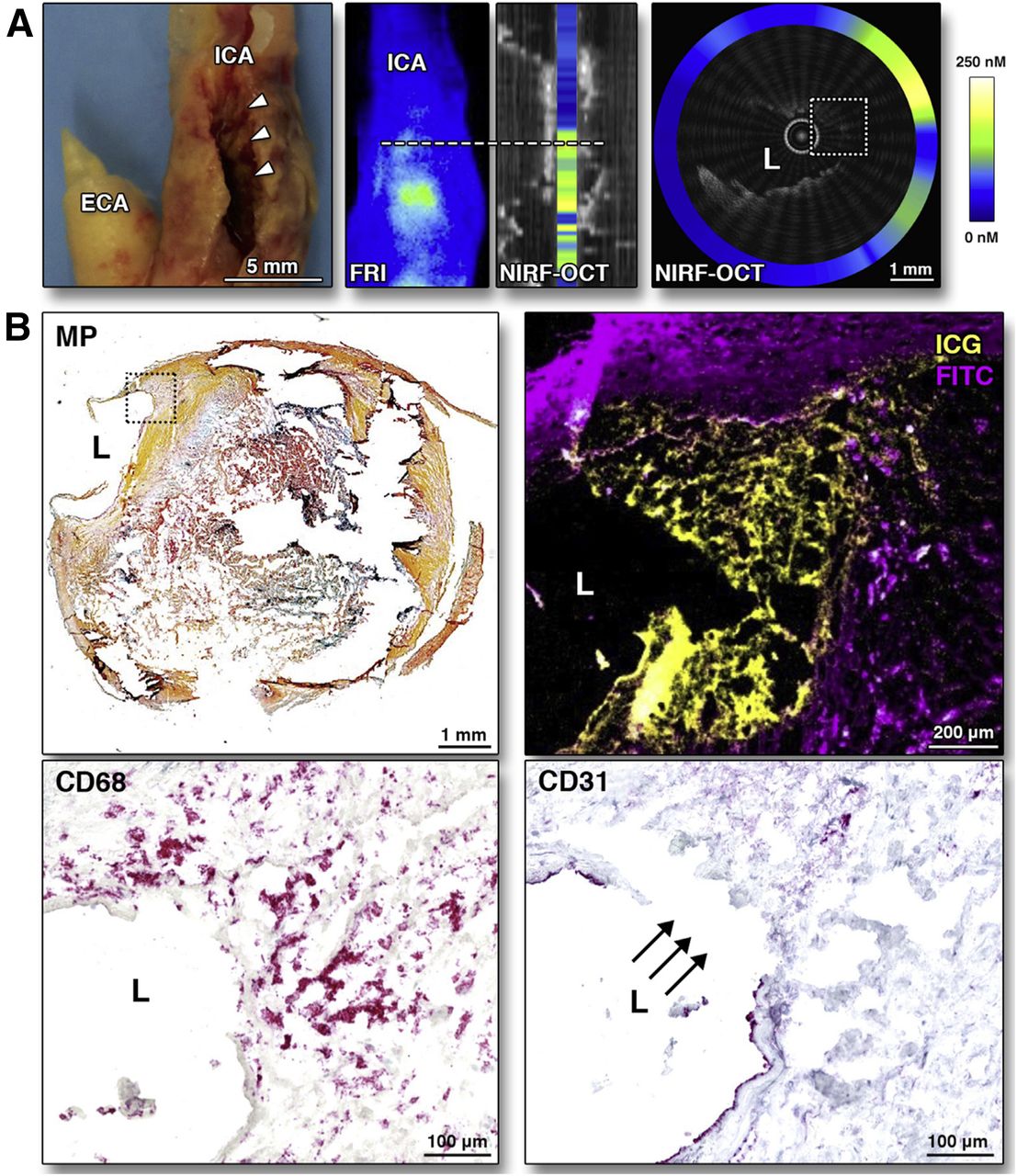
Jaffer et al. engineered and tested a fully automated rotational 2-dimensional NIRF imaging catheter in rabbit atheroma to detect NIRF inflammatory cysteine protease activity with nanomolar sensitivity (19). Stent-induced inflammatory vascular injury was also demonstrated, suggesting the potential to understand how inflammation may predict restenosis in living subjects. Translationally, indocyanine green (ICG), a Food and Drug Administration–approved NIRF imaging agent, has shown promise for intravascular NIRF imaging (20). A clinical ICG study recently reported that ICG serves as a human in vivo plaque imaging agent in carotid endarterectomy specimens (21). ICG was reliably detected by ex vivo NIRF imaging and near-infrared fluorescence microscopy, and was found to report on endothelial barrier compromise, and deposited in adjacent areas of macrophage infiltration and plaque hemorrhage (Fig. 3).
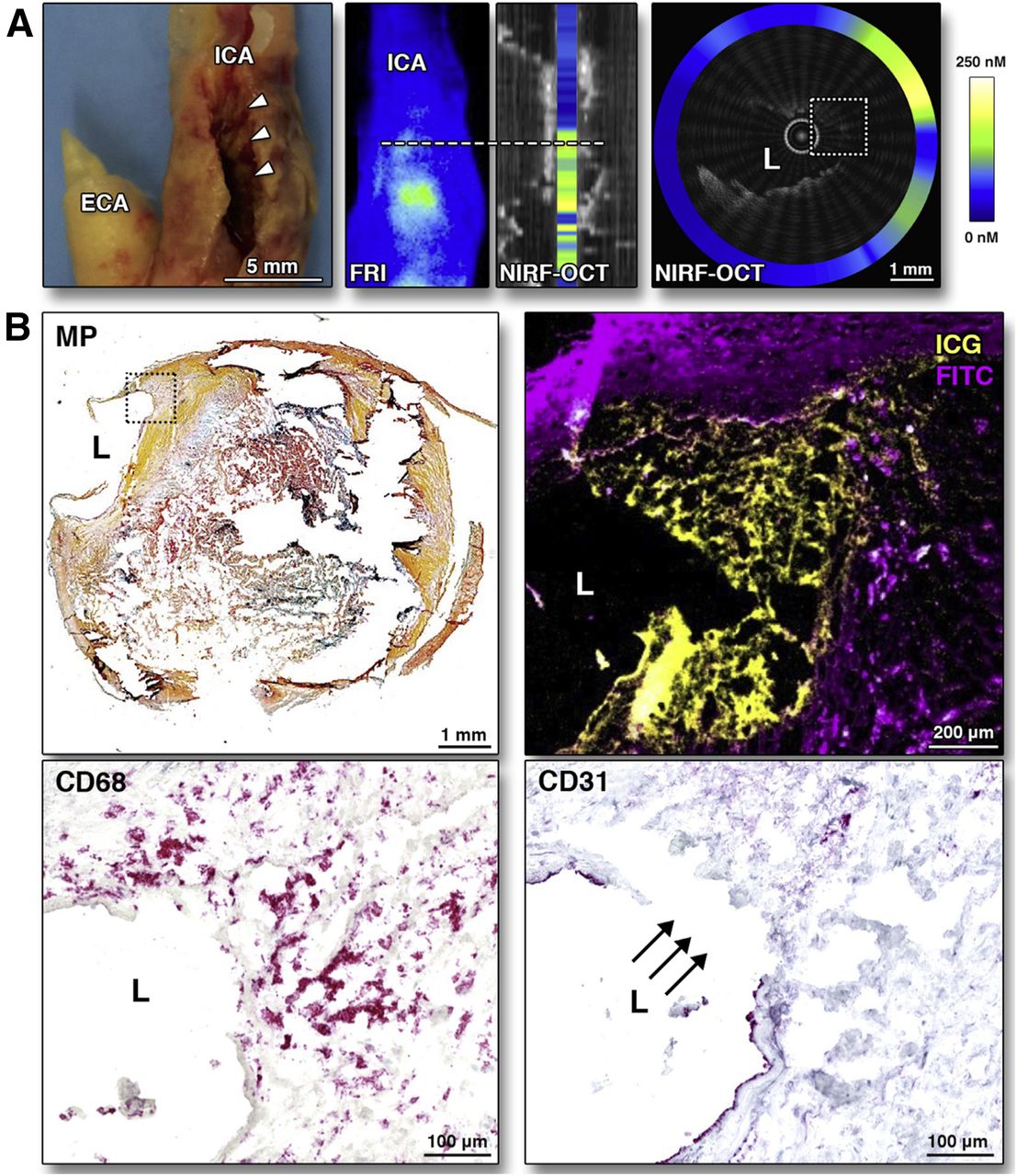
NIRF imaging of ICG deposition in human atheroma. (A) Aligned photo, fluorescence reflectance image (FRI), and long-view NIRF OCT fusion image of resected human carotid atheroma. Ninety minutes after intravenous ICG administration, elevated ICG signal (green-yellow) presents area of severe stenosis (arrowheads). NIRF OCT cross-sectional image at white dotted line shows thinned/absent fibrous cap (white dotted box), with corresponding high NIRF ICG signal. (B) High-magnification histology reveals complex plaque (top left, Movat’s Pentachrome [MP]) and surface ICG NIRF uptake (yellow, top right; fluorescein isothiocyanate [FITC autofluorescence (purple)]). ICG NIRF–positive areas demonstrate endothelial barrier disruption (CD31; arrows) and macrophage infiltration (CD68). ICA = internal carotid artery; L = lumen. (Reprinted with permission from Verjans et al. (21).)
Because standalone NIRF imaging is limited by a lack of anatomic information, a next-generation intravascular NIRF imaging system incorporating coregistered optical coherence tomography (OCT) structural imaging was constructed (22). Integrated NIRF OCT imaging combines high-sensitivity NIRF detection with exquisite 10- to 20-μm OCT spatial resolution and can illuminate inflammatory plaque protease activity in experimental atherosclerosis, as well as fibrin deposition on clinical-grade coronary stents (23). Recently, first-in-human intracoronary NIRF OCT imaging was successfully performed to image NIR autofluorescence in 12 patients (24). With additional development, including integrating NIRF with intravascular ultrasound (25), intravascular NIRF imaging is positioned to transform clinical molecular imaging of coronary atherosclerosis and stents.
VTE
Background
Deep venous thrombosis (DVT) and pulmonary embolism (PE), collectively known as VTE, remain leading causes of morbidity and mortality worldwide. Diagnostically, compression ultrasonography and CT pulmonary angiography are the primary clinical imaging modalities for assessing DVT and PE, respectively. Although ultrasound and CT pulmonary angiography are well validated for diagnosing VTE, they have limited ability to diagnose recurrent VTE, predict the efficacy of fibrinolytic therapy for PE, or predict debilitating complications such as the DVT-induced postthrombotic syndrome, or PE-induced chronic thromboembolic pulmonary hypertension.
VTE is an intertwined thrombotic and inflammatory process, consisting of an initial neutrophil infiltrate followed by a monocyte–macrophage influx. These cells coordinate to promote endogenous fibrinolysis, thrombus stabilization, and ensuing VTE resolution. Several thrombus-targeted imaging agents have been developed for PET or SPECT imaging (Table 1) but have not yet demonstrated diagnostic advantages over anatomic ultrasound or CT imaging. However, VTE inflammation as an imaging target has undergone limited evaluation. Recently, 18F-FDG PET/CT imaging of VTE has been used in humans to assess DVT age. Future studies are needed to assess this tool’s role in diagnosing recurrent DVT, a vexing clinical problem.
Selected Clinical and Translational Metabolic and Molecular Imaging Agents for Illuminating Atherosclerosis and VTE
18F-FDG PET Imaging of VTE
Primary DVT
Rondina et al. performed the first prospective study demonstrating that 18F-FDG PET/CT is a sensitive imaging tool for detecting symptomatic, proximal first-time (primary) DVT. The authors observed significantly higher 18F-FDG uptake in thrombosed vein segments over matched contralateral segments without thrombosis. 18F-FDG was accurate in diagnosing DVT with 87.5% sensitivity and 100% specificity. Although limited by a small sample size, this study demonstrated that the 18F-FDG DVT uptake diminished over time (26).
Recurrent DVT
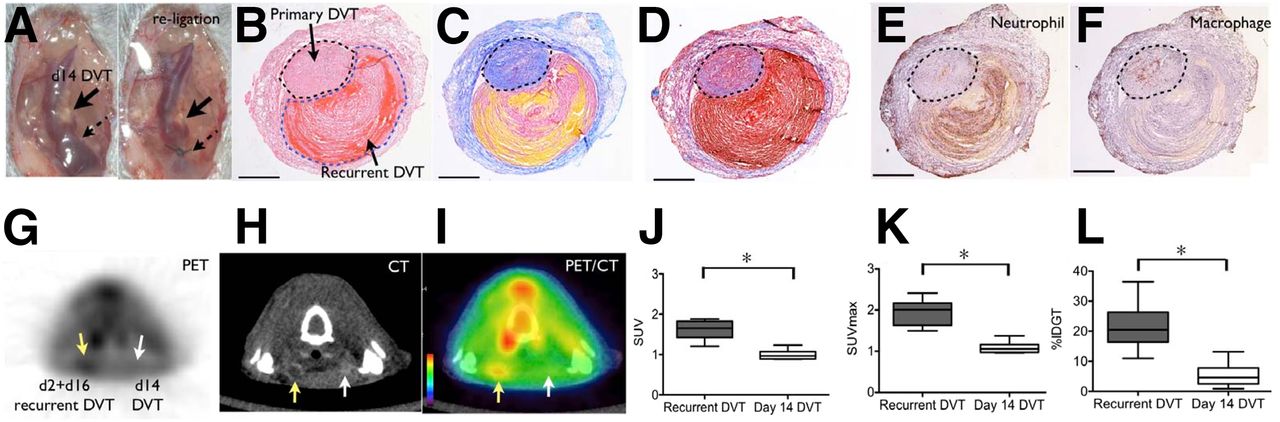
Recurrent DVT occurs up to 10% per year after an unprovoked DVT and increases the risk of postthrombotic syndrome, PE, and death (27). Although accurate diagnosis of recurrent same-site VTE is critical for justifying reinitiation of anticoagulation therapy, its diagnosis is challenging for conventional ultrasound due to residual vein wall scarring or thrombus from the initial DVT. Recognizing that 18F-FDG PET can report on DVT metabolic or inflammatory activity, and that a recurrent DVT should generate a new inflammatory response, Hara et al. leveraged 18F-FDG PET/CT to accurately diagnose recurrent DVT in mice (Fig. 4) (28). Analysis of thrombosed veins showed that most 18F-FDG uptake was in the thrombus (70%), with a minority signal in the vein wall (30%). Furthermore, they observed that inflammatory 18F-FDG DVT signal was more closely associated with neutrophils than macrophages and that 18F-FDG uptake was neutrophil-dependent and accordingly higher in early-stage, neutrophil-rich DVT. Finally, the authors demonstrated that clinical 18F-FDG uptake in DVT diminishes with increasing DVT age, extending earlier results.
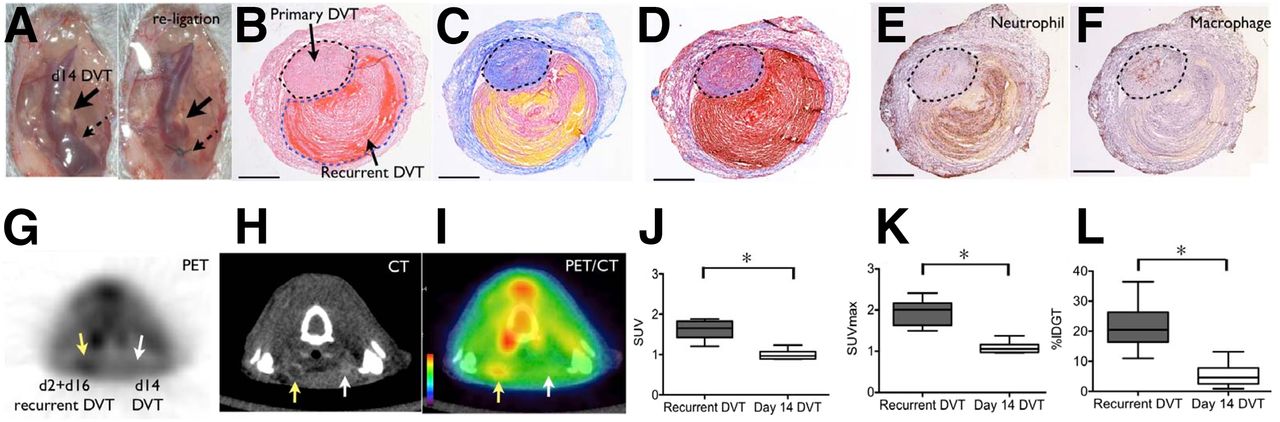
18F-FDG PET/CT imaging of recurrent VTE. (A) Mouse model illustrating day-14 DVT and religation of jugular vein to create recurrent DVT mouse model used in 18F-FDG PET imaging. Histologic staining with hematoxylin and eosin (B), Carstairs (C), and Masson’s Trichrome (D) of resected day-2 recurrent DVT (black dotted line) overlying day-16 DVT (blue dotted line) show red blood cell and fibrin-rich areas in recurrent DVT (red and yellow area in B–D) and collagen-rich zones in older primary DVT (blue areas in C and D). Immunostaining for neutrophils (E) and macrophages (F) highlight differences between recurrent DVT and older DVT. 18F-FDG PET/CT images (G–I) of recurrent and primary DVT show increased 18F-FDG uptake in recurrent DVT (J–L). Yellow arrows = recurrent DVT; white arrows = primary day 16 DVT. (Reprinted with permission from Hara et al. (28).)
PE
Case reports and retrospective studies have described 18F-FDG uptake in PE, mostly as incidental findings in whole-body cancer staging 18F-FDG PET/CT imaging sessions (29–31). As suspected, metabolically active tumors may mimic VTE 18F-FDG enhancement, increasing the chances of false-positive diagnosis (32,33). Interestingly, delayed 18F-FDG imaging (2 h after injection) may be more specific for PE and should be considered in future studies (30). Although CT pulmonary angiography is the gold standard for PE diagnosis, 18F-FDG PET might also be useful for detecting recurrent PE (28). In addition, 18F-FDG PET assessment of thrombus age could help predict the success of fibrinolytic therapies, as suggested by recent preclinical molecular imaging investigations (34,35).
SUMMARY AND FUTURE DIRECTIONS
Atherosclerosis
As showcased above, metabolic and molecular imaging approaches have the potential to better predict clinical events, tailor selection of pharmacotherapeutic and interventional therapies, and assess pharmaceutical efficacy.
Large Arterial Beds
Larger arteries, in particular the carotid artery, are well suited to noninvasive PET imaging. Therefore, we anticipate that future studies of carotid 18F-FDG PET will extend the initial insights provided by Marnane et al. (6), and better determine which carotid lesions are high risk and warrant a more intensive medical or interventional approach. This is an area of vital importance, as there remains controversy about when to intervene on asymptomatic severe interval carotid artery lesions, and whether biologic data (beyond currently available stenosis information) might help guide that decision (36). Risk-benefit of radiation exposure and cost-effectiveness will need to be further analyzed.
In addition to assessing plaque inflammation in clinical subjects, as robustly demonstrated (4,5,7–9,11,12,14,18), noninvasive carotid 18F-FDG PET/CT will continue to play a role in evaluating novel pharmacotherapy antiinflammatory effects. New tracers have an opportunity to improve the ability to sensitively and specifically detect plaque inflammation (37) but will need outcome validation to serve as a compelling challenger to 18F-FDG.
Coronary Arterial Imaging
Background cardiomyocyte metabolic signal, cardiorespiratory motion, and partial-volume effects greatly affect the reliability to detect 18F-FDG signal in coronary arteries, particularly distal to the proximal coronary segments. In contrast, 18F-Na PET does not suffer from myocardial background uptake and appears to be a reliable noninvasive option for imaging coronary plaque osteogenic activity/calcification. Future studies are needed to determine 18F-Na’s clinical value beyond widely available calcium scoring and CT angiography. There is also promise for this tracer to understand the potential effects of bisphosphonates and statins on the pathophysiology of coronary calcification.
Intravascular NIRF molecular imaging shows promise for high-resolution molecular imaging and can be integrated with intravascular ultrasound (25) or OCT (22), strengthening the ability to provide comprehensive molecular–structural imaging of atherosclerosis and stent biology. However, NIRF imaging is in its infancy for clinical translation and will require clinical outcome studies to determine its value. Given its invasive requirement, NIRF imaging will likely be used to further stratify patients already undergoing percutaneous coronary intervention for ACS or stable angina.
VTE
The ability of 18F-FDG PET to image VTE inflammation may provide a new opportunity to detect recurrent DVT and may provide a foundation for guiding anticoagulation decisions. However, outcome and safety studies are needed. In addition, 18F-FDG PET may soon provide insights into the postthrombotic syndrome, a common complication of DVT that is partly inflammation driven. For PE, new imaging tracers may help identify which thrombi are amenable to fibrinolysis, a question of particular importance given recent neutral data of fibrinolysis in patients with intermediate-risk PE (38).
CONCLUSION
Metabolic and molecular imaging with 18F-FDG PET and other modalities are providing valuable insights into atherosclerosis and VTE pathophysiology in human subjects. 18F-FDG PET and emerging metabolic/molecular imaging technologies are expected to evolve as outcomes studies emerge, and are further analyzed for cost-effectiveness and safety. Overall, these advances are expected to shed important insight into atherosclerotic disease pathophysiology, help identify novel treatment strategies, and improve clinical evaluation and management of individual patients.
DISCLOSURE
The following sources supported this study: NIH R01HL122388 (Farouc A. Jaffer), R01HL122177 (Ahmed Tawakol), and K08HL130465 (Eric A. Osborn); and MGH Hassenfeld Research Scholar Fund (Farouc A. Jaffer). Dr. Jaffer received research funding from Siemens and Canon and has a consulting agreement with Boston Scientific and Abbott Vascular. Massachusetts General Hospital has a patent licensing arrangement with Canon Corporation. Dr. Jaffer has the right to receive licensing royalties through this licensing arrangement. Dr. Osborn has consulting agreements with DynaMed and St. Jude Medical. Dr. Tawakol received research funding from Actelion, Genetech, and Takeda and has a consulting agreement with Actelion. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Apr. 27, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication December 16, 2016.
- Accepted for publication April 19, 2017.





{kind=link}
{kind=link}
{kind=link}
{kind=link}