


Abstract
The optimal management of radioactive iodine (RAI) treatment in patients with metastatic thyroid cancer (TC) is still a matter of debate. Methods: We retrospectively analyzed 352 patients with RAI-avid metastatic well-differentiated TC treated with 131I by an empiric fixed activity of 3.7 GBq at Gustave Roussy (GR, n = 231) or by personalized activity (2.7–18.6 GBq) based on whole-body/-blood clearance (WB/BC) dosimetry at Memorial Sloan Kettering Cancer Center (MSKCC, n = 121). The primary endpoint was to compare overall survival (OS) in the 2 groups of patients by log-rank test. Results: Patients received a median cumulative activity of 14.8 GBq at GR and 24.2 GBq at MSKCC (P < 0.0001). The median follow-up after the diagnosis of metastases was 7.2 y (0.4−31 y). Five-year OS was 86.8% and 78.8% for patients treated at GR and at MSKCC, respectively (P < 0.01). However, there was no statistical difference in OS after correction for sex, age at the diagnosis of distant metastases, metastases site, and metastases extension between the 2 centers (P = 0.16). OS at 5 y was 96% and 96% for patients younger than 40 y with micrometastases, 70% and 65% for patients older than 40 y with macrometastases or multiple metastases, and 92% and 87% for younger patients with macrometastases or older patients with micrometastases treated at GR and MSKCC, respectively (P = not significant). Conclusion: Routine use of WB/BC dosimetry without lesional dosimetry provided no OS advantage when compared with empiric fixed RAI activity in the management of thyroid cancer patients with RAI-avid distant metastases.
See a commentary on this article on page 697.
Radioactive iodine (RAI; 131I) has been used since the late 1940s for the treatment of patients with distant metastases from differentiated thyroid cancer (1). The optimal management in terms of administered 131I activity, number of treatment courses, and their frequency remains unclear.
For RAI to have a therapeutic effect, it is necessary to deliver a tumoricidal radiation dose to the metastatic foci (2–5). On the basis of the assumption that higher administered activities (>9.25 GBq) of RAI would be more likely to deliver therapeutic lesional radiation doses, many centers use whole-body/-blood clearance (WB/BC) dosimetry to define the maximum tolerated activity (MTA) that can be safely administered (6). Others use empiric fixed activities (3.7–9.25 GBq) to treat metastatic disease based on the assumption that any increase in lesional radiation dose achieved with larger administered activities is unlikely to confer therapeutic benefit (7,8). Finally, studies on lesional dosimetry support the concept that tumoral lesion–absorbed dose can predict the response to RAI treatment (5,9).
While acknowledging the theoretic advantages of dosimetry, the American Thyroid Association guideline taskforce found insufficient evidence in the literature to recommend a preferred approach (10). The effectiveness of RAI therapy is associated with many clinicopathologic features. In a previous study of 444 differentiated thyroid cancer patients with distant metastases, 3 distinct groups with markedly different overall survivals (OS) have been defined. Young patients (<40 y of age) with disease that was not visible on radiologic imaging demonstrated a 10-y survival rate of 95%, whereas older patients with macroscopic pulmonary metastases (>1 cm) or multiple bone metastases showed a 10-y survival of only 14%. An intermediate 10-y survival of 64% was seen in young patients with macroscopic disease and older patients with subcentimeter pulmonary nodules (8).
Therefore, the aim of this study was to compare OS within the 3 previously described outcome groups in patients with RAI-avid distant metastases from a differentiated thyroid cancer treated by RAI according either to an empiric approach at Gustave Roussy (GR) or to a WB/BC dosimetric approach at Memorial Sloan Kettering Cancer Center (MSKCC).
MATERIALS AND METHODS
We retrospectively evaluated the medical records of patients with distant metastases from differentiated thyroid cancer who were treated either at GR (empiric approach) or at MSKCC (WB/BC dosimetric approach) from 1980 to 2010. The institutional review board of both centers approved this retrospective study, and the requirement to obtain informed consent was waived. A common electronic medical database was created and the key clinical variables entered. All patients with the following criteria were included: histologically confirmed well-differentiated thyroid cancer, RAI-avid metastatic lesions on the 131I WB scan after a therapeutic activity of 131I, and at least 1 administration of 131I for treatment of metastases. Patients with no demonstrated 131I-avid metastases or with metastases from a poorly differentiated thyroid cancer were excluded from the analysis. The extent of metastasis was classified as previously described: category 1 = metastases detectable on 131I WB scan but normal radiologic imaging (x-rays or CT scan); category 2 = micronodular (<1 cm) lung metastases or single bone metastasis identified radiologically; and category 3 = macronodular lung metastases or multiple bone metastases or both bone and lung metastases (1,7,8).
The primary endpoint was to compare OS in the 2 centers.
OS was analyzed within 3 predetermined patient groups based on the 2 previously described prognostic indicators for survival: age of 40 y at the time of metastases diagnosis and the above-mentioned metastases category (8). Group 1 included patients younger than 40 y with no visible disease on radiologic imaging (category 1), micronodular lung metastases, or single bone lesion (category2). Group 2 included patients younger than 40 y with either macrometastases (category 3) or patients older than 40 y with micrometastases (categories 1 and 2). Finally, Group 3 included patients older than 40 y with lung macrometastases or multiple bone metastases (category 3) (8).
Primary Tumor Treatment
As an initial treatment of primary tumor, all included patients underwent a total thyroidectomy with or without lymph node dissection, based on local practice patterns.
RAI Treatment
Empiric Approach
Each 131I treatment course in adult patients consisted of the administration of a standard activity of 3.7 GBq of 131I after thyroid hormone withdrawal (THW) for 4–6 wk (thyroid-stimulating hormone [TSH] > 30 mUI/L). Low iodine diet was not recommended, but contrast product injection was avoided within the 2 mo before RAI treatment. In children, an activity of 37 MBq/kg of body weight and in patients with renal failure a fixed activity ranging between 1.1 and 2.2 GBq was administered at each treatment. Posttherapeutic WB scanning was performed 3–5 d after each 131I treatment course. Anterior and posterior images were obtained with a double-head γ-camera equipped with high-energy collimators and thick crystals (AXIS; GE Healthcare). In the case of 131I-avid distant metastases on the posttherapy scan, another 131I treatment was administered 3–9 mo later for 2 y and then once a year, until the disappearance of any significant uptake on the posttherapy WB scan. No diagnostic 131I WB scan was obtained before any 131I treatment course. There was no fixed limit to the cumulative activity of 131I administered.
Dosimetric Approach
The MTA calculation at each 131I treatment course was based on sequential 131I body retention measurements, on diagnostic 131I WB scan and blood 131I clearance studies as previously described (6,11). Before 1999, all 131I treatments were administered after THW for 6 wk and in the case of TSH greater than 30 mUI/L. After 1999, 131I was usually administered after recombinant human TSH (rhTSH) (Thyrogen; Genzyme Corp.) administration (12). In all patients, RAI was administered after 7–10 d of a low-iodine diet. WB images and counts and blood samples were obtained at 0, 2, 4, 24, 72, and 96 h after administration of a tracer activity of 131I (37–185 MBq) for the THW patients and at 0, 2, 4, 24, 48, 72, and 120 h for the rhTSH patients. At each time interval, blood was drawn, and the fractional blood clearance was determined. Total-body clearance curves were generated, and the activity was calculated with the constraint of 200 cGy to the blood or 2.96 GBq of WB retention at 48 h in the case of diffuse lung uptake, as previously described (6,11,12). For the rhTSH protocol, 0.9 mg of intramuscular rhTSH was administered on 2 consecutive days during week 1 for dosimetry and then 2 additional rhTSH doses were given in week 2 in preparation for the therapeutic administration of RAI. Calculated activity according to MTA was administered the day after the second rhTSH injection. For the diagnostic WB scan, anterior and posterior projections were obtained using a dual-head Genesys EPIC imaging system (ADAC Corp.). WB images in anterior and posterior views associated with the anterior, posterior, and lateral spot of the neck and the thorax were acquired 4–7 d after 131I administration in all treated patients.
The timing between additional treatment courses ranged from 6 mo to 2 y (or longer) and was based on individual clinical characteristics such as the volume of metastatic lesions, their RAI avidity, the effectiveness of previous therapies, the trend in serum thyroglobulin levels, and the side effect profile of previous treatments.
Other Treatments for Metastatic Disease
During RAI treatment, patients received surgery in 27.3% and 24% of cases, radiation therapy in 28.1% and 34.7% of cases, and cytotoxic chemotherapy for progression after RAI treatment in 4.3% and 10.8% of cases at GR and MSKCC, respectively (Supplemental Table 1; supplemental materials are available at http://jnm.snmjournals.org).
Statistical Analysis
A descriptive analysis was performed for the 2 groups of patients. χ2 and Mann–Whitney–Wilcoxon tests were performed to identify differences in the 2 groups for qualitative and quantitative variables, respectively.
OS was estimated from the time of the diagnosis of the metastases until patient last follow-up or death by the Kaplan–Meier method. OS in the 2 groups was first compared using the log-rank test. A Cox proportional hazards model was then used for the evaluation of the risk of death. Key factors possibly contributing to OS were explored, including age at diagnosis of distant metastases, sex, tumor histology, extent of metastases, and location. These were first tested individually (univariate analysis). Multivariate analysis was then performed to compare the OS between the 2 groups, taking into account the aforementioned variables that were significant in the univariate analysis (significance level, P < 0.05) and the year of diagnosis of the metastases. For all analyses, 2-sided t tests and the 0.05 level of significance were used. Ninety-five percent confidence intervals (95% CIs) were calculated for the relative risks (RRs) in the Cox model analysis. Statistical analysis was performed using SAS software (version 9.4; SAS Institute, Inc.).
RESULTS
Patient Population
A total of 701 and 155 medical records of patients with distant metastases of differentiated thyroid cancer were evaluated at GR and MSKCC, respectively. At GR, 231 of 701 met inclusion criteria for the study. Four hundred seventy patients were excluded because of poorly differentiated cancer (n = 205), they were treated before 1980 (n = 104), they were not treated by RAI (n = 67), they had no RAI-avid metastases (n = 82), and they did not receive any RAI treatment at GR (n = 12). At MSKCC, 121 of 155 patients met inclusion criteria for the study. Thirty-four patients were excluded because of poorly differentiated cancer (n = 28), because they had no RAI avid metastases (n = 2), and because they did not receive any RAI treatment at MSKCC (n = 4). Finally, a total of 352 patients were analyzed. Clinical characteristics of the patients are reported in Table 1.
Clinical Characteristics of Patient Population
Patients received a median of 4 (range, 1–14) 131I treatment courses at GR and 3 (range, 1–9) at MSKCC for a median cumulative activity of 14.8 GBq (range, 1.8–52.5 GBq) at GR and 24.2 GBq (range, 2.7–112 GBq) at MSKCC (P < 0.0001). The median activity for each treatment was 3.7 GBq (1.1–11.1) at GR and 9.3 GBq (2.7–18.6) at MSKCC (P < 0.0001) (Supplemental Table 1). At GR, 19 patients received an 131I activity lower than 3.7 GBq because of younger age (n = 14), renal failure (n = 1), older age (n = 1), or brain metastases (n = 1). Three patients received more than 3.7 GBq (5.2, 8.7, and 11.1 GBq) at their first treatment course in other centers and then were referred to GR for further treatments. At MSKCC, only 17% of patients received all treatments exclusively after THW. Of the remaining 83%, more than three fourths of treatments were administered after rhTSH stimulation.
The median number of treatments, the median administered activity, and the median cumulative activity according to patient group (groups 1, 2, and 3) are summarized in Table 2.
Median Number of 131I Treatments, Median Administered Activity, and Median Cumulative Activity (GBq) According to Patient Group
OS for Entire Cohort
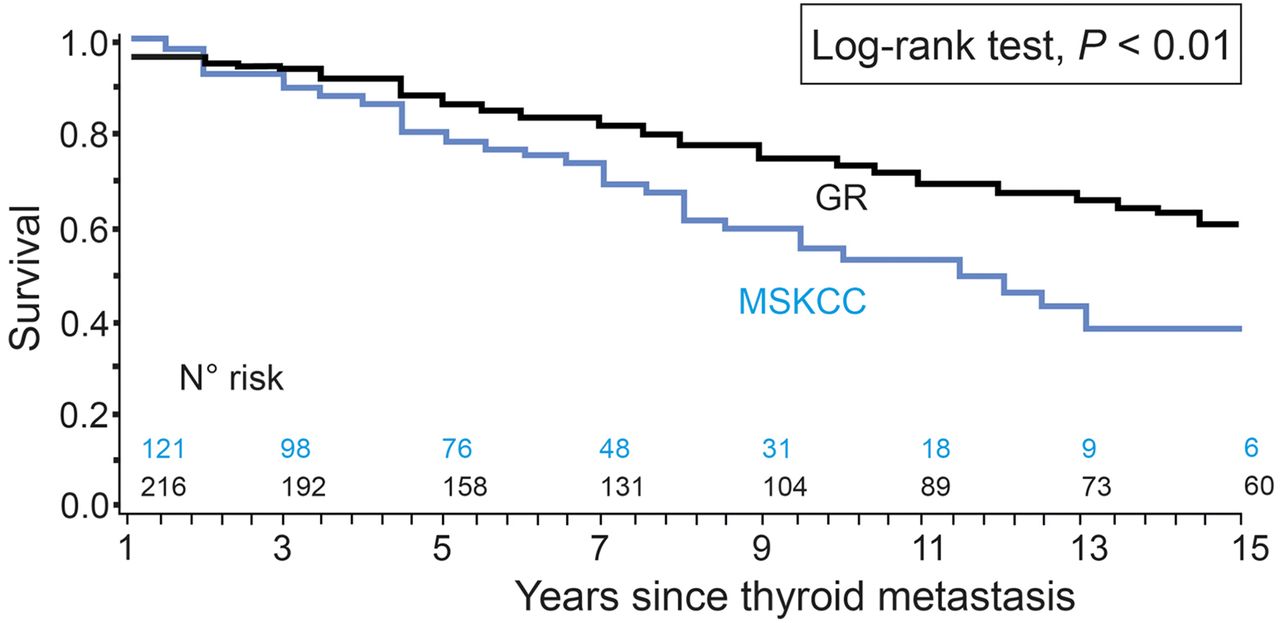
After a median follow-up of 7.2 y (range, 0.4−31 y) (8 y [range, 0.4−31 y] for patients treated at GR and 6.4 y [range, 1–25.6 y] for patients treated at MSKCC [P < 0.001], respectively), 68.2% of the patients were still alive (70.6% vs. 63.6% at GR and MSKCC, respectively). Thyroid cancer was the cause of death in 69.7% of the patients. Death related to a second cancer was reported in 7.4% (5/68) and 9.1% (4/44) of cases at GR and MSKCC, respectively. OS at 5 y was 86.8% and 78.8%, and at 10 y it was 73.2% and 53.1% at GR and MSKCC, respectively (P < 0.01) (Fig. 1).

OS estimated from time of diagnosis of metastases until patient last follow-up or death.
In univariate analysis, male sex, age over 40 y at the diagnosis of distant metastases, follicular histology, macro- or multiple metastases, and the presence of both lung and bone metastases had a negative impact on OS (Table 3). In multivariate analysis, male sex, age over 40 y at the diagnosis of distant metastases, and metastases extension were prognostic factors. Despite differences between the patient cohorts at the 2 centers, when statistically corrected for these factors, OS did not differ in the 2 centers (RR, 1.41 for MSKCC patients, P = 0.16) (Table 3).
Univariate and Multivariate Analyses of Factors Predicting OS
OS Within Predefined Patient Groups
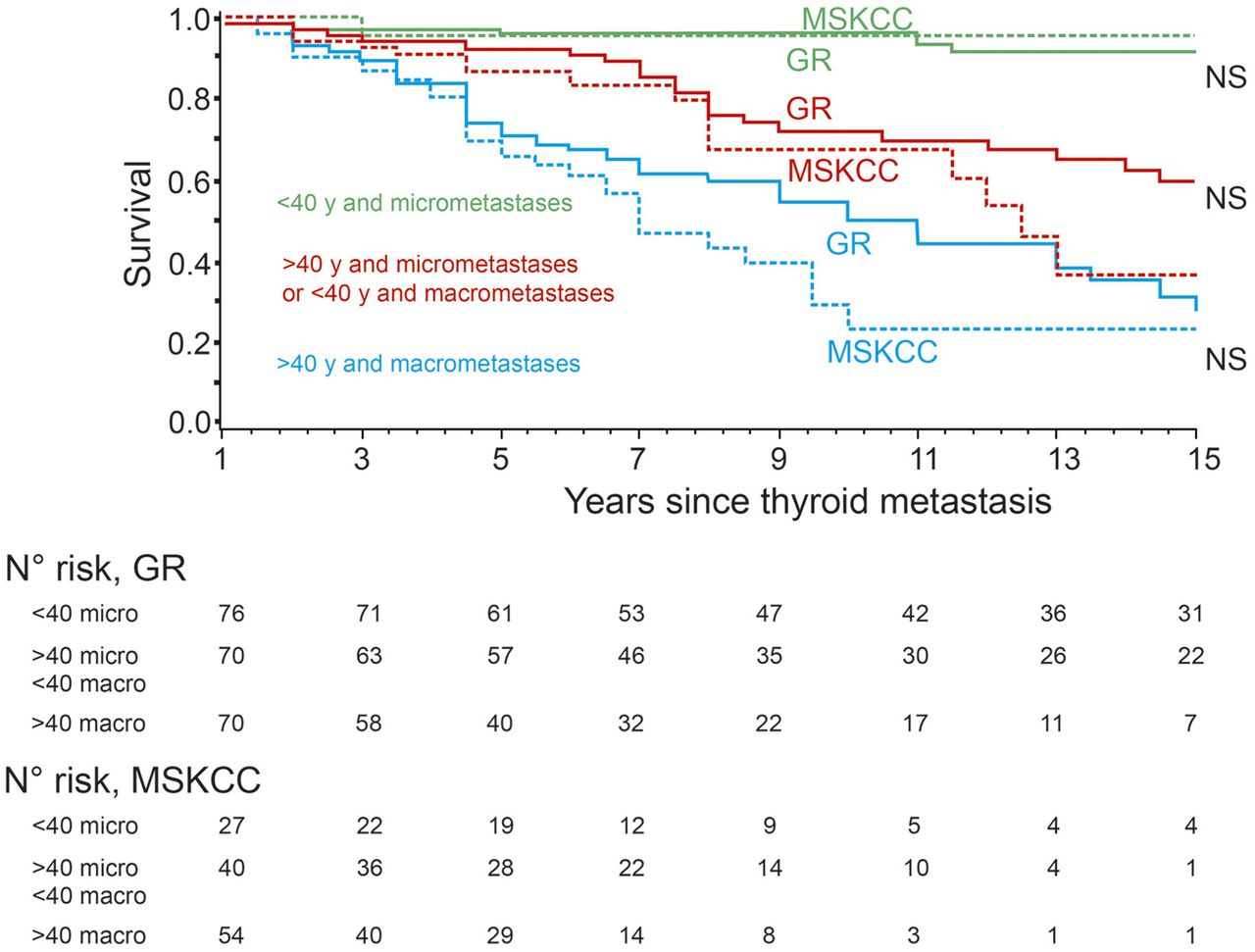
To further control for the differences between the patient characteristics between GR and MSKCC, OS was evaluated in the patient groups matched by age, size, and site of distant metastases (Fig. 2). The best OS was seen in group 1, with no difference between the 2 centers. Five- and 10-y OS was 96% (95% CI, 0.73–0.99) and 96% (95% CI, 0.73–0.99) for MSKCC and 96% (95% CI, 0.88–0.99) and 96% (95% CI, 0.88–0.99) for GR, respectively (P = not significant). The poorest OS was seen in group 3 for both MSKCC and GR patients. Five- and 10-y OS was 65% (95% CI, 0.50–0.77) and 23% (95% CI, 0.09–0.41) for MSKCC and 70% (95% CI, 0.58–0.80) and 49% (95% CI, 0.35–0.62) for GR, respectively (P = not significant). Group 2 demonstrated intermediate outcomes. Five- and 10-y OS was 87% (95% CI, 0.71–0.94) and 67% (95% CI, 0.46–0.81) for MSKCC and 92% (95% CI, 0.83–0.97) and 72% (95% CI, 0.58–0.82) for GR, respectively (P = not significant).

OS according to age and extent of metastases estimated from time of diagnosis of metastases until patient last follow-up or death.
DISCUSSION
This is the largest study comparing patients with RAI-avid distant metastases from well-differentiated thyroid cancer treated with RAI either with fixed activities at GR or with WB/BC-determined activities at MSKCC. The MSKCC cohort received higher median RAI administered activities per treatment course (9.3 vs. 3.7 GBq), higher cumulative RAI activities (24.2 vs. 14.8 GBq), were older (median age, 53 vs. 42 y, P = 0.01), were more likely to have macroscopic lung metastases (36% vs. 22%, P = 0.02), were less likely to have small-volume RAI-avid pulmonary metastases (12% vs. 30%, P < 0.001), and were more likely to receive RAI therapy after rhTSH (83% vs. 0%, P < 10−10). However, when adjusted in a multivariate analysis for the prognostically important differences between the centers (age at the discovery of distant metastases, metastases extension, sex, and histology), OS did not significantly differ between the 2 institutions. In addition, 5- and 10-y OS did not differ between the 2 institutions when considering predefined matched patient cohorts (groups 1, 2, and 3).
Therefore, it does not appear that routine use of the MSKCC WB/BC dosimetry management approach without lesional dosimetry provides a significant survival advantage over the GR empiric dosing approach. While not demonstrating differences in progression-free survival, one previous retrospective study of 87 patients did demonstrate a clinical benefit from a dosimetry-based approach (compared with empiric dosing) with respect both to increasing the likelihood of complete response and to decreasing the odds of progression by a factor of 0.29, particularly in patients with locally advanced differentiated thyroid cancer (13). In these patients, higher activities may be more efficient at controlling the disease than lower fractionated activities.
In previous GR series, most patients younger than 40 y with small metastases were cured with a cumulative administered activity of less than 22 GBq, and their life expectancy was close to that of the normal population, with a 5-y OS of 98% (7,8). Small bone metastases without abnormalities on morphologic imaging are most likely to be cured with few RAI treatments especially in young patients (14,15). On the other hand, in these previous studies only a few patients with large and multiple metastases were cured with 131I, and the 5-y OS in these patients was 60%, in accordance with the present study (8). In these selected patients, higher activities might be more beneficial and lesional dosimetry could be critical for decision making and to define the optimal administered activity that would be predicted to achieve a therapeutic tumoricidal dose. Some authors showed that 124I PET–guided lesional dosimetry can predict absorbed lesion doses and can help to calculate the safest and the most effective 131I activity to be administered (4,9,16–18). The possibility of a modern quantification procedure by SPECT/CT could also allow the calculation of absorbed dose in normal organs and tumoral lesions (19). Finally, approaches to reprogram the biology of metastatic thyroid cancer cells by restoring expression of genes required for iodide uptake and accumulation are under study to improve RAI efficacy (20). Concerning patient stimulation, the efficacy of 131I administrated either after thyroid hormone withdrawal or after rhTSH is another matter of debate. Even if absorbed dose in tumoral lesions may be higher after THW than after rhTSH administration, in a previous study no difference in OS was found in metastatic patients treated after either THW or rhTSH stimulation, with a 5-y OS at 75%–80% in both groups of patients and with a median OS of 12.5 y for patients with micrometastases and 4.4 y in patients with macrometastases (12,21,22).
Concerning toxicity, empiric high activity can be above the MTA. Tuttle et al. reported that an empiric activity of 7.4 GBq exceeded the MTA in 8%–15% of patients younger than 70 y and in 22%–38% of patients older than 70 y, and an empiric activity of 9.25 GBq exceeded the MTA in 22% of patients younger than 70 y and in 50% of patients older than 70 y (23). However, no serious acute adverse event has been reported for an empiric activity of 3.7 GBq (24).
This study presents the following limits. First, safety data are not available because of the retrospective nature of the study and several missing data in medical reports. Only data on death from second cancers have been reported, and this does not differ between the 2 centers. We cannot conclude on a long-term safety profile of the 2 different approaches. The study of Klubo-Gwiezdzinska et al. showed a similar safety profile on dosimetric approach compared with empiric approach (13). Second, we cannot compare the remission rate with each of the 2 approaches, because the follow-up was not standardized. Third, even if OS does not differ in patients treated with an empiric or a dosimetric approach, the populations in the 2 centers are not perfectly matched and the effect of rhTSH versus THW preparation on 131I efficacy still remains unknown.
CONCLUSION
This is the first study comparing OS in a large number of patients with RAI-avid distant metastases of thyroid cancer treated either with the empiric or with the WB/BC dosimetric approach. These data indicate that using a WB/BC dosimetric approach without lesional dosimetry to safely administer higher RAI activities was not associated with an improvement in OS. A standard activity of 3.7 GBq can be considered efficient and certainly safe in treating patients with distant metastases. However, future studies that use accurate measurements of lesional dosimetry are likely to define a subset of patients in whom WB and blood dosimetry studies may be required to ensure that the administered activity necessary for therapeutic efficacy does not exceed safety limits, for example, in patients in whom empiric dosing may be associated with an increased risk of toxicity (renal failure, diffuse miliary lung metastases). Finally, approaches to reprogram the biology of metastatic thyroid cancer cells may be coupled to WB/BC as well as lesional dosimetry to optimize both safety and efficacy.
DISCLOSURE
Martin Schumberger has received grant/research support from Genzyme, and R. Michael Tuttle is a consultant for Genzyme. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 13, 2016.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication June 15, 2016.
- Accepted for publication September 19, 2016.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer
- Treatment of refractory thyroid cancer
- Reply: Fixed 3.7-GBq 131I Activity for Metastatic Thyroid Cancer Therapy Ignores Science and History
- Fixed 3.7-GBq 131I Activity for Metastatic Thyroid Cancer Therapy Ignores Science and History
- Comparison of Empiric Versus Dosimetry-Guided Radioiodine Therapy: The Devil Is in the Details
- Prescribed Activity of 131I Therapy in Differentiated Thyroid Cancer
- Reply: Comparison of Empiric Versus Dosimetry-Guided Radioiodine Therapy: The Devil Is in the Details