


Abstract
This study sought to answer the calls that have been made for the European Association of Nuclear Medicine to restore its surveys of reported adverse reactions. We assessed all reports of adverse reactions to radiopharmaceuticals that were submitted to the British Nuclear Medicine Society (BNMS) online database (Radiopharmaceutical Adverse Events and Product Defects) from January 2007 to December 2016. Methods: This investigation was a pharmacovigilance-based, nonexperimental, cross-sectional study aimed at finding the prevalence of, and association between, radiopharmaceuticals and adverse reactions. Results: During the study period, there were 204 reports of radiopharmaceutical adverse reactions, of which 13 were considered invalid, primarily because of incomplete entries or because a causal relationship between the radiopharmaceutical and the adverse reaction could not be determined. Tetrofosmin (34 reports) and oxidronate (32 reports) had the highest prevalence, followed by medronate (21 reports) and then sestamibi and nanocolloid (14 reports each). Rash (84 reports), itching (46 reports), and vomiting (30 reports) were the 3 most frequently occurring adverse reactions. Most reports (96.8%) were for diagnostic radiopharmaceuticals. Conclusion: The prevalence of adverse reactions to radiopharmaceuticals reported in the BNMS database remains low, with a frequency of 3.1 reports per 100,000 administrations in 2013 and 2.5 per 100,000 administrations in 2015. In our review spanning 10 years, we did not find any particular concern about the use of radiopharmaceuticals.
According to statistics released by the National Health Service in England, approximately 560,000 imaging examinations with radioisotopes were performed in the country from April 1, 2015, to March 31, 2016. The Diagnostic Imaging Dataset collection, which was first instituted in 2012/2013, states that approximately 520,000 similar procedures were performed in that year (1).
As nuclear medicine procedures have become more widespread, numerous studies have been performed to highlight the prevalence of adverse reactions to radiopharmaceuticals. In 2002, the European Association of Nuclear Medicine published a survey of the nature and frequency of reports submitted to the British Nuclear Medicine Society (BNMS) online database (Radiopharmaceutical Adverse Reactions and Product Defects) in 2000. In that year, there were 62 reports of adverse reactions to radiopharmaceuticals (2). No subsequent survey of reports to the BNMS database has been published.
However, some of the countries that participate in the BNMS database have surveyed the adverse reactions that have been reported within their own country. For example, Laroche et al. identified 304 reports to the French Pharmacovigilance Database from 1989 to 2013. The annual incidence of reported adverse reactions to radiopharmaceuticals for that period ranged from 1.2 to 3.4 per 100,000 diagnostic administrations. The frequency of adverse reactions to radiopharmaceuticals was 6.2 × 10−4 times that of reports from other classes of drugs (3).
This investigation, a nonexperimental, cross-sectional study aimed at learning the prevalence of, and association between, radiopharmaceuticals and adverse reactions, sought to answer the calls that have been made for the European Association of Nuclear Medicine to restore its surveys of reported adverse reactions (4,5). Our objective was to provide additional information for nuclear medicine practitioners globally, as well as to identify signals for uncommon and unexpected adverse reactions. We assessed, categorized, and analyzed all reports of radiopharmaceutical adverse reactions that were submitted to the BNMS database from January 2007 to December 2016, thus taking a retrospective look at that 10-year period.
MATERIALS AND METHODS
The study protocol was registered as a clinical audit with the Audit Department of the Royal Liverpool and Broadgreen University Hospitals National Health Service Trust before the commencement of the study. The Clinical Audit Committee ruled this study exempt from Institutional Review Board review and from obtaining informed consent as it dealt with fully anonymized data. The data, provided by the BNMS, included age, sex, and clinical information only.
For each report, the algorithm of Silberstein et al. was used to determine the probability of a causal relationship between the radiopharmaceutical and the adverse reaction, as suggested by the Pharmacopeia Committee of the Society of Nuclear Medicine and Molecular Imaging (6,8). A causal relationship was classified as probable, possible, or unlikely. Statistical analysis was performed with the Statistical Package for Social Sciences software program (version 24.0) and Excel 2010 (Microsoft). The results were expressed in terms of mean, median, SD, interquartile range, or percentage frequency, as appropriate.
All events were routinely reviewed by a senior medical practitioner, with a view toward identifying any trends in the use of radiopharmaceuticals in particular clinical settings and toward defining the clinical context of any such trends.
RESULTS
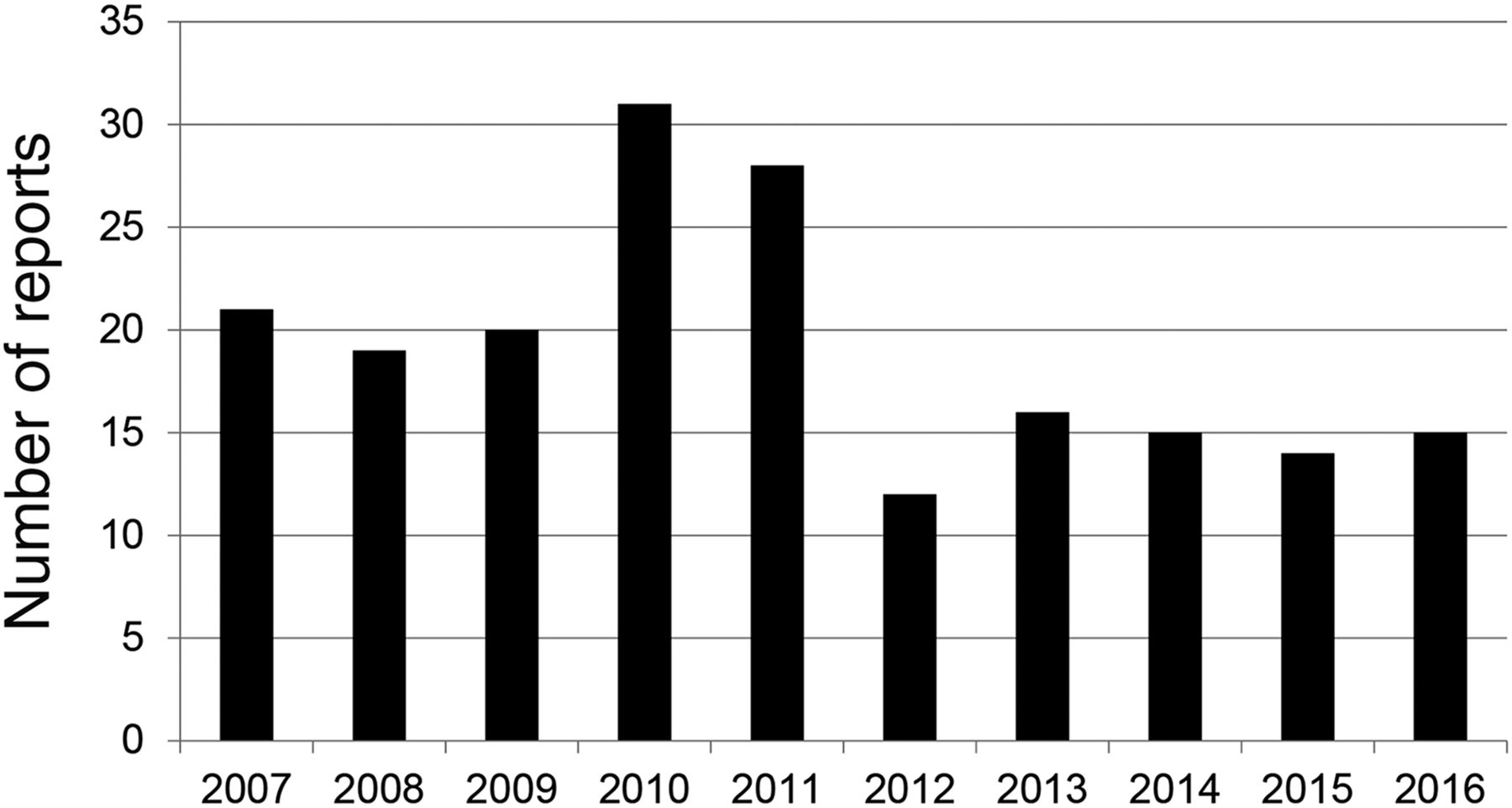
During the study period, 204 reports of adverse reactions were submitted to the BNMS database. Of these reports, 13 were considered to be invalid because of incomplete entries or because a causal relationship could not be determined. Of the remaining 191 reports, the greatest number, 31, occurred in 2010 and the fewest, 12, were in 2012 (Fig. 1). The reports were submitted primarily by the United Kingdom, with one report each from Italy and Germany.
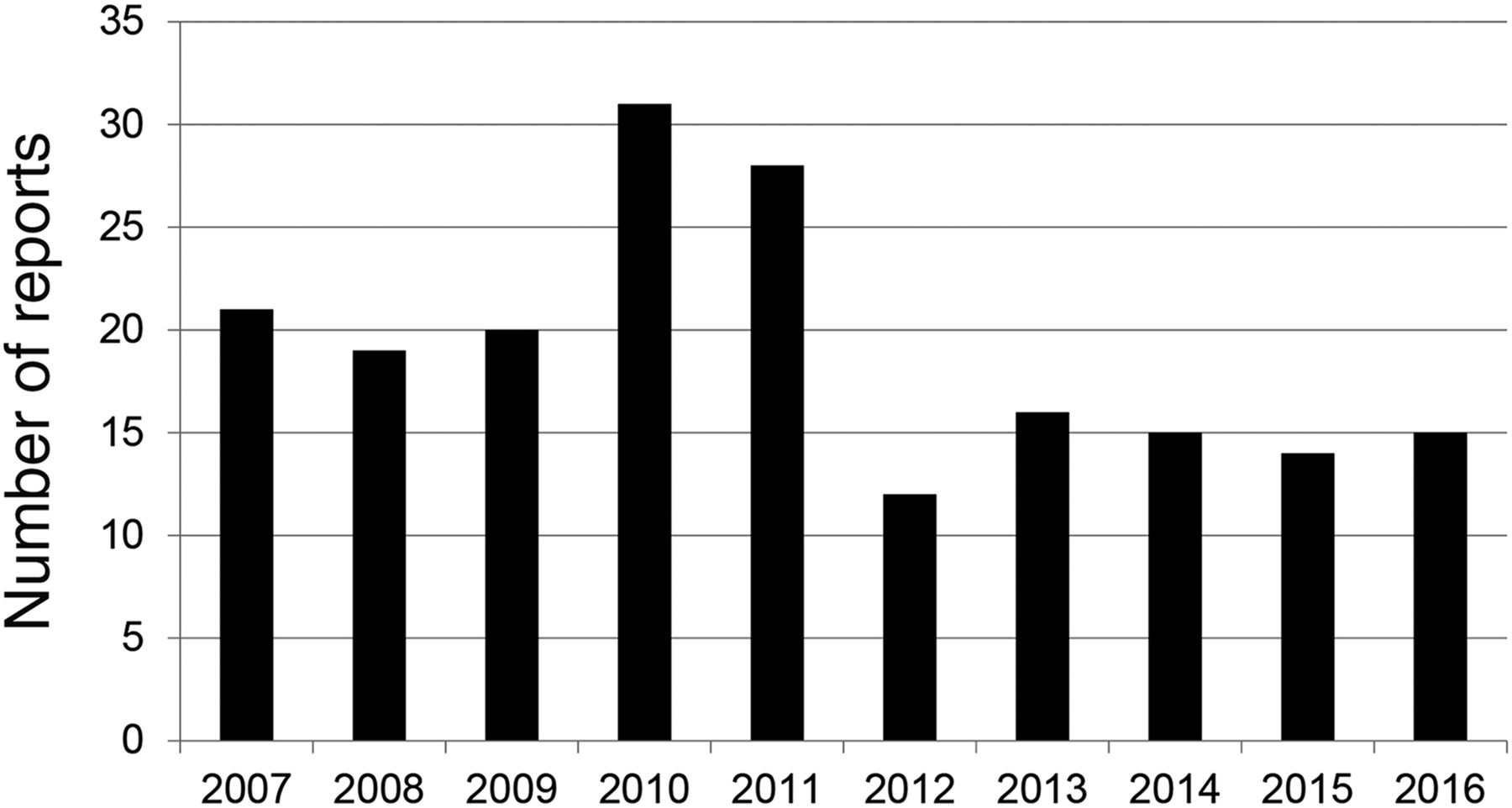
Number of reports of adverse reactions to radiopharmaceuticals each year from 2007 through 2016.
Eleven (5.8%) of the 191 reports did not record the age of the patient. The mean age (±SD) of the remaining 180 patients was 47 ± 23 y (range, 1–93 y), and the median age was 52 y. Patients 60 y old or older made up the largest proportion of the study population (31.9%), whereas those 12–19 y old made up the smallest (3.7%). The study population included 128 women (67.0%) and 57 men (29.8%), with the sex being unidentified in 6 reports (3.2%).
Twenty-nine radiopharmaceuticals were reported. Sixteen (55%) were 99mTc-labeled products, and 13 (45%) were nontechnetium products. 18F-FDG and 68Ga-DOTANOC were the only PET radiopharmaceuticals among the agents. All except 131I-NaI and 223Ra-dichloride (Xofigo; Bayer) were diagnostic agents.
A causal relationship was classified as probable for 109 reports (57.1%), possible for 67 (35.1%), and unlikely for 15 (7.9%). No fatalities due to radiopharmaceutical administration were reported. However, 15 patients were hospitalized, 33 were admitted to the accident or emergency department of their hospital, and 34 sought medical attention from their general practitioner. Of the 15 patients who were hospitalized, 7 had experienced anaphylactic reactions; 6 of these patients were treated with intravenous hydrocortisone, and 3 with intravenous chlorpheniramine. In total, 9 patients overall were treated with oxygen, 3 received adrenaline, 4 were nebulized with salbutamol, and 4 received intravenous fluids. Eighty patients did not receive pharmacologic intervention for the relief of symptoms, and 37 reports provided no information on treatment.
DISCUSSION
Most of the reported adverse reactions were included in the Summary of Product Characteristics for the radiopharmaceutical. There were, however, a few exceptions. This study found some adverse reactions to 75Se-tauroselcholic acid that, to our knowledge, were previously unreported. The use of 75Se-tauroselcholic acid capsules for the detection of bile acid malabsorption was first authorized in January 2002, with the only side effect reported in the Summary of Product Characteristics being hypersensitivity reactions (of an unknown frequency) (7). Although 2 of 7 reports were of side effects anaphylactic in nature (rash, itching, dyspnea, throat constriction), there were also reports of dizziness, nausea, a burning sensation, and pain. The onset of hypersensitivity reaction (rash and itching) ranged from immediately after ingestion of the capsule to 24 h after ingestion.
Silberstein (8) found 15 reports of flushing of the face and trunk within minutes of 18F-FDG administration from 15 nuclear medicine facilities in the United States between 2007 and 2011 (8), whereas Laroche et al. found that 27 cases of adverse reactions to 18F-FDG, involving mainly the skin, were reported to the French Pharmacovigilance Database between 1989 and 2013 (3). The current study, however, found a report of sweating, nausea, vomiting, and uncontrollable diarrhea within 90 min of injection, for which the patient was kept overnight for observation.
Other adverse reactions that, to our knowledge, are being reported for the first time occurred with 111In-octreotide, 51Cr-ethylenediamine tetraacetic acid, 68Ga-DOTANOC, 99mTc-mercaptoacetyltriglycine, 99mTc-tetrofosmin, and 99mTc-labeled carbon (Technegas; Cyclomedica) (Table 1).
Previously Unreported Adverse Reactions and Probability of a Causal Relationship with the Radiopharmaceutical
Consistent with the findings of previous studies on adverse reactions, the most common adverse reactions found in this study were rash and itching (3,8). The use of intravenous and oral antihistamines, as well as corticosteroids, continues to be the mainstay for treatment of these reactions.
Coadministration of pharmacologic agents as a part of a nuclear medicine procedure, such as in a myocardial perfusion (stress) test, may create uncertainty about which agent caused an adverse reaction. One patient reported impaired function when attempting to drive home after a myocardial perfusion stress test with 99mTc-tetrofosmin. He reported a lack of appropriate reactions to normal driving conditions, and the impairment persisted on the following day. When the patient returned for the rest scan there was no adverse event, leading the reporting practitioner to suspect that the reaction might have been due to the administered stress agent, regadenoson. However, the Summary of Product Characteristics for regadenoson states that it is expected to have little to no influence on the ability to drive or use machines once treatment has been completed. Another patient experienced swelling and redness of the face, as well as vomiting, after the rest test, and the stress test was therefore cancelled. The uncertainty experienced in the former case was not present in the latter, as a pharmacologic agent was not administered during the rest test.
The presence of comorbidities in patients presenting for nuclear medicine imaging also has implications for the use of pharmacologic agents. Although the reporting system of the BNMS makes provision for identification of other known medications, only 127 of the 191 reports utilized this function, 46 of which stated that the patients were on no other medications. Absence of information on coadministered medications in the other 64 reports is therefore a limitation to the findings of this study.
A feedback mechanism, such as the reporting system currently offered by the BNMS, is beneficial to the nuclear medicine community: patients, health care professionals in the field, and the pharmaceutical companies that manufacture and distribute radiopharmaceuticals (9). Although the prevalence of adverse reactions remains stable (8), reports provide health-care professionals with knowledge of possible, probable, and unlikely adverse reactions.
As was stated in an editorial by Hesse et al. (4), the unique growth and expansion of nuclear medicine procedures and the corresponding use of radiopharmaceuticals will undoubtedly lead to an increase in the frequency of adverse reactions. Although reporting is voluntary, it is therefore recommended that nuclear medicine departments report all suspected adverse reactions. The first reported occurrence of an adverse reaction to a particular drug may be categorized as unlikely, but continuous reporting provides an avenue for the identification of associated trends.
CONCLUSION
The reporting of adverse reactions to the BNMS database between 2007 and 2016 was well within the expected levels. Our review did not identify any particular areas of concern about the use of radiopharmaceuticals for certain clinical conditions.
DISCLOSURE
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank the United Kingdom Radiopharmacy Group for its vision and consistent effort in promoting pharmacovigilance in the field of nuclear medicine across Europe. The efforts of Professor Marvin Reid from the University of the West Indies, Mona Campus, Jamaica; the International Atomic Energy Agency; and the Royal Liverpool and Broadgreen University Hospitals Trust to enable the collaboration between these institutions in facilitating the training of nuclear medicine practitioners is also appreciated.
Footnotes
Published online May 18, 2017.
- © 2017 by the Society of Nuclear Medicine and Molecular Imaging.
REFERENCES
- Received for publication March 28, 2017.
- Accepted for publication May 9, 2017.





{kind=link}