


This supplement to The Journal of Nuclear Medicine on breast cancer imaging comprehensively addresses the current status of both PET and single-photon imaging of the breast and of localized and metastatic breast cancer. I was asked to introduce the supplement with a commentary that not only looks backward at history but—far more important—looks forward at opportunities and challenges.
HISTORICAL REVIEW
My interest in imaging breast cancer with PET began in the late 1980s with my, and many others’, gradual recognition that the radiotracer 18F-FDG, originally designed for brain imaging, was actually a promising visceral tumor imaging agent (1–3). The early contributions of the late Ludwig Strauss to colorectal cancer imaging with PET were quite informative at that time (4). Although at that stage of my career I was interested in applying monoclonal antibodies to tumor imaging, the target-to-background ratios achieved with 18F-FDG in a variety of animal studies of multiple tumor types were often higher and occurred sooner after radiotracer injection than when targeting with more specific monoclonal antibodies was used. With access to early-generation whole-body PET imaging in the late 1980s at the University of Michigan, the quickest approach to finding out whether 18F-FDG worked in women with breast cancer was to secure human-use approval and conduct the human studies. The answer was, basically, yes, 18F-FDG PET works, with limitations.
While we began to use 18F-FDG with PET, pioneering studies were being performed in the late 1980s in Finland by Heikki Minn et al., who introduced 18F-FDG for breast cancer imaging by a planar, non-PET, technique in 1989 (5). Using a specially collimated nontomographic γ-camera, they studied 17 patients with breast cancer and were able to detect the tumor in 14 (82%), including 6 of 8 known lymph node metastases. 18F-FDG was also able to detect bone metastases and was more sensitive in detecting lytic or mixed lesions than in detecting purely sclerotic lesions. In the assessment of treatment response in 10 patients, increased 18F-FDG uptake was consistently associated with disease progression, whereas decreased uptake was often, but not invariably, associated with resolving or stable disease. However, planar imaging is an insensitive technique, and images are limited by low resolution and sensitivity and are certainly not quantitative.
Case studies, including ours, reported the feasibility of imaging breast cancer using PET with 18F-FDG in several patients (3,4,6). Subsequently, we systematically evaluated the feasibility of using 18F-FDG PET to image the primary tumor and regional and systemic metastases (7). The 18F-FDG PET method detected 25 of 25 known foci of breast cancer, including primary lesions (10/10), soft-tissue lesions (5/5), and bone metastases (10/10). Four additional nodal lesions that had not previously been identified were also detected. Several of the primary cancers were detected in women with radiographically dense breasts, though these tumors were relatively large (>2 cm). That point is of particular interest in view of the current issues surrounding breast cancer detection in women with radiographically dense breasts.
In the early 1990s, we determined that although 18F-FDG uptake in breast cancer was multifactorial, uptake often correlated with overexpression of glucose transporter 1 in viable breast cancer cells (8). A general relationship between viable cell number and degree of 18F-FDG uptake was seen in vivo in animals and humans, suggesting that uptake might be used as a metric of treatment response. With breast cancer being located near the heart, it was possible to perform dynamic PET studies of breast cancer and of the great vessels, allowing for noninvasive dynamic, quantitative assessment of treatment-related changes in 18F-FDG uptake in cancerous and normal tissues. In these studies, uptake could be quantified (unlike what could be achieved with planar imaging) and, with noninvasive imaging of the great vessels, could be analyzed by SUV, compartmental analysis, and Patlak–Gjedde analyses. These imaging tools, combined with a growing interest in neoadjuvant chemotherapy (i.e., in situ chemotherapy of the primary tumor in order to provide treatment sooner and have a biomarker of response) as opposed to chemotherapy after mastectomy or lumpectomy, allowed us to test whether quantitative 18F-FDG PET could serve as an early biomarker of response. In brief, this prospective study showed that multiagent systemic therapy caused a rapid and significant decline in breast cancer 18F-FDG uptake, k3 kinetic rate constants, and Ki (or influx constants) for 18F-FDG as early as 8 d after treatment initiation. Further declines in uptake were apparent after 21, 42, and 63 d of treatment in patients who went on to have a complete or partial response, whereas no significant decline in uptake was seen in nonresponding patients (n = 3) when examined at 63 d after initiation of treatment. This study also showed that metabolic changes antedated anatomic changes and that the substantial declines in tumor glucose metabolism were apparent in responding patients despite no change in tumor size (9). Follow-up studies reviewed elsewhere in this supplement have supported the general validity of this metabolic monitoring approach (10). For example, in the Translational Breast Cancer Research Consortium study of neoadjuvant therapy, the change in 18F-FDG uptake from day 0 to day 15 had an area under the curve of 0.76 in a group of more than 50 patients. This indicates good, but not perfect, accuracy in separating responders from nonresponders (11). Higher accuracies were reported more recently by Groheux et al. (12). Methods of analysis of quantitative 18F-FDG PET data have been reviewed (13). It may be possible for 18F-FDG PET to predict a noncomplete pathologic response with reasonable reliability.
We also had the opportunity to determine the reliability of 18F-FDG for staging lymph node metastases of breast cancer after diagnosis. This approach had good diagnostic accuracy but, in a large prospective multicenter study, had an accuracy too low (area under the curve, 0.76) to be truly useful in most breast cancer patients and was subsequently supplanted by sentinel node surgical procedures. High 18F-FDG uptake by SUV and multiple tumor foci in the axilla were highly predictive of the presence of tumor (14). Since the introduction of 18F-FDG PET in breast cancer, there have been about 3,000 articles (PubMed) evaluating a wide range of applications of PET imaging in breast cancer, many reviewed by experts in this supplement.
THE CURRENT STATE OF THE ART
18F-FDG PET Breast Imaging
Although the current state of the art of molecular breast imaging has been updated well in the individual components of this supplement, it is probably fitting to briefly summarize that of specifically 18F-FDG PET more than a quarter century after its initial introduction in humans.
Breast cancers accumulate 18F-FDG relatively avidly, and 18F-FDG is the main PET tracer used to image breast cancer. A variety of other positron-emitting labeled metabolic tracers to image breast cancer have also been explored. Uptake of 18F-FDG is somewhat lower in breast cancers, particularly lobular breast cancer, than in other common visceral cancers and is typically higher in more aggressive cancers, particularly triple-negative breast cancers, reflecting the biologic signature from 18F-FDG PET. With conventional whole-body PET/CT scanners, primary tumors smaller than 1 cm in diameter commonly escape detection. Evolving higher-resolution dedicated breast PET imaging devices (positron emission mammography) may be more capable of detecting these small lesions. Nonetheless, many primary breast cancers can be imaged, and intense focal uptake in the breast that is incidentally detected on PET or PET/CT warrants careful evaluation for possible cancer. PET/CT can detect breast cancer metastatic to axillary lymph nodes and internal mammary nodes, but the sensitivity is typically about 75%–85%, less than that of either axillary dissection or sentinel node sampling for axillary metastases. Nevertheless, the positive predictive value of intense or multiple foci of 18F-FDG uptake in nodes is high for the presence of cancer.
18F-FDG PET is excellent for detecting soft-tissue and systemic metastatic disease, including lytic and invisible (presumably bone marrow) bone metastases but can be falsely negative in blastic bone metastases. Although results vary somewhat by organ involvement, higher values of the quantitative parameters of SUV, metabolic tumor volume, and tumor lesion glycolysis on 18F-FDG PET are generally linked to less favorable survival outcomes (15,16). Sodium fluoride PET can detect both lytic and blastic metastases and may have greater sensitivity than 18F-FDG PET for blastic metastases. The ability of 18F-FDG PET/CT to monitor treatment response is attractive and allows individualization of therapy. The glycolytic metabolic rate of breast cancers falls rapidly with effective chemotherapy, at a rate considerably faster than the decline in tumor size with treatment. In both primary and metastatic breast cancers, a lack of decline or a minimal decline in 18F-FDG uptake with treatment suggests that the treatment is not effective.
At present, PET/CT is used most commonly to determine the extent of systemic disease and to quickly monitor the response of primary and metastatic cancers to treatment. PET/CT generally is preferred to PET alone, as the former appears to be somewhat more accurate and provides superior diagnostic certainty. Because the cost of PET is reimbursed by the Centers for Medicare and Medicaid Services in a variety of settings, it is quite widely available in the United States (17).
Single-Photon Molecular Breast Imaging
The performance characteristics of single-photon molecular breast imaging using 99mTc-sestamibi are discussed elsewhere in this supplement, but the method is showing reasonable sensitivity and specificity for detecting breast cancers, nearly as sensitive as MRI. Recently, the sensitivity for detecting invasive ductal breast cancer (86.1%) was found to be higher than that for detecting invasive lobular breast cancer (56.7%) using molecular breast imaging. This finding suggests that a subset of cancers will fail to be detected by molecular breast imaging (18).
With both the PET and the single-photon methods, a dose of radiation is delivered to the whole body—a limitation of radionuclide approaches. By contrast, mammography and tomosynthesis deliver, mainly to the breast, a low radiation dose. MRI methods have been considered safe and do not include ionizing radiation, but it is clear that gadolinium-based contrast agents can be associated with nephrogenic systemic fibrosis in patients with diminished renal function, and dose-dependent gadolinium deposits can be detected in the brains of healthy patients (of uncertain significance) (19).
Although PET and single-photon molecular breast imaging have been around for some years, the decreased sensitivity of these methods versus mammography for detecting small cancers, combined with a desire to detect all cancers, has limited their extensive use. By contrast, PET with 18F-FDG of the whole body is used quite commonly for systemic staging and treatment response monitoring. Radionuclide injection into breast lesions to help guide surgical procedures is growing in importance as well, as an alternative or complement to wire localization studies (20).
THE QUESTION OF WHETHER MOLECULAR BREAST IMAGING IS NEEDED
Shortfalls of Anatomic Imaging
Anatomically based breast imaging faces multiple challenges and opportunities. Failure to detect breast cancer on screening can result in litigation, more intensive treatment of cancer diagnosed at a later stage, and loss of life (21). Failure to detect cancer in women with dense breasts is not uncommon with mammography. Similarly, there is the problem of overdiagnosis, meaning that finding small, indolent cancers potentially may not be in the patient’s best interest. Digital mammography is ill-equipped to solve the challenge of improving accuracy and detecting only clinically relevant cancer. Digital breast tomosynthesis shows promise to improve cancer detection and may preferentially detect invasive cancer rather than ductal carcinoma in situ (DCIS) and thereby partly mitigate problems with overdiagnosis (22–24). MRI has potential in this domain but suffers from specificity limitations.
Although screening mammography saves lives (14%–32% reduction in breast cancer mortality in the screened groups in randomized controlled trials), a cumulative estimate of 42% and 62% of women screened biennially and annually (respectively) over a period of 10 y is expected to have a false-positive mammogram-detected abnormality (25,26). These false-positives are estimated to cost the health-care industry up to 4 billion dollars yearly in biopsy, pathology, and radiology costs, in addition to causing patients unneeded distress (27). Women currently accept these false-positives and the transient distress as the price of detecting meaningful early-stage cancers, removal of which can save their lives. Can nuclear medicine breast imaging help in this group of patients?
So-called overdiagnosis is the detection of a tumor through screening that would not have become clinically relevant in the absence of screening. Many of these cancers are indolent ductal carcinomas in situ, though some may be invasive. Unadjusted estimates of breast cancer overdiagnosis from screening mammography range from 0% to 52%. When adjusted for lead-time bias and breast cancer risk, overdiagnosis of breast cancer most likely is in the 1%–10% range (28). If overdiagnosis occurs 1%–5% of the time, it is probably not a major problem. If more than 10%, it is a growing concern.
It is hard to know with certainty which cancers are overdiagnosed, and the reductions in mortality demonstrated with mammography have required comprehensive treatment for all cancers. Thus, some cancers might be overdiagnosed and others, once detected, overtreated in an effort to be cautious. When a screening-detected abnormality is confirmed to be cancer, what often follows is a combination of surgery, radiation, and systemic therapy. Although such treatment is appropriate for aggressive cancers, some mammogram-detected cancers are biologically indolent and overtreatment can occur. To combat both sets of costs (i.e., false-positive findings and overtreatment of biologically indolent disease), alternative strategies for disease detection and stratification are increasingly necessary.
Perhaps 25% of breast cancers detected by screening mammography are ductal carcinomas in situ. A recent review of a decade of data from the Surveillance, Epidemiology, and End Results (SEER) Program showed that the mortality rates of women with DCIS (the kind with calcifications often detected by mammography) have been low over 20 y, at about 3%, and in the range of the death rate seen in the general population of women (29). Perhaps 25% of breast cancers detected with screening mammography fall into this class of malignancy. This finding suggests that less aggressive approaches to treatment of these tiny, mammographically detected cancers, at least in older Caucasian women (African American and younger women appear to have a poorer prognosis), might be needed or explored and that we need to continue to rethink our traditional approach to breast cancer diagnosis and treatment. In the SEER patients with DCIS, radiation therapy did not appear to save lives (albeit the data are retrospective). It is of interest that pathologists, like radiologists, do not agree unanimously on which breast lesions are malignant. In a JAMA study of pathologists in which diagnostic interpretation was based on a single breast biopsy slide, overall agreement between the individual pathologists’ interpretations and the expert consensus–derived reference diagnoses was 75.3%, with the highest level of concordance being for invasive carcinoma and levels being lower for DCIS and atypia (84% concordance for DCIS).
There is active discussion over whether some breast cancers, such as some DCIS, are overdiagnosed or overtreated. For example, in older women with other health risk factors, DCIS is unlikely to cause the death of a patient. Esserman et al., in an editorial entitled “Rethinking the Standard for Ductal Carcinoma in Situ Treatment,” pointed out that resection of 50,000 or more cases of DCIS per year has not substantially reduced the frequency of invasive ductal breast cancers. Esserman posits that “Much of ductal carcinoma in situ should be considered a ‘risk factor’ for invasive breast cancer and an opportunity for targeted prevention.” Further, she suggests that “Low- and intermediate-grade ductal carcinoma in situ do not need to be a target for screening or early detection” but also suggests that “We should continue to improve our understanding of the biology of the highest-risk ductal carcinoma in situ (large, high-grade, hormone receptor-negative, HER2-positive disease, especially in very young and African American women) and test targeted approaches to reduce death from breast cancer.” (30).
Clearly, we need better tools to assess the biologic relevance of cancers. What are some possibilities for the evolution of PET and molecular breast imaging?
Opportunities for Nuclear Imaging
With nuclear breast imaging, we may have an opportunity to play a role in assessing the biologic relevance of breast cancers. The 18F-FDG signal is typically greater in more aggressive breast cancers (31,32). Perhaps the treatment of breast cancer will become more like the treatment of prostate cancer, for which less aggressive cancers are sometimes followed by active surveillance as opposed to prostatectomy when the risks of the surgery may be viewed as too extreme relative to the benefit. One can envision managing women with DCIS in a more personalized fashion. In such an approach, women with biologically indolent disease could benefit from an active surveillance protocol similar to that currently used in managing low-risk prostate cancer. The concept would involve the partial or total removal of a small DCIS, after or through the biopsy. Perhaps sequential mammograms or tomosynthesis, augmented by positron emission mammography or molecular breast imaging and MRI, could be used to follow such lesions while placing patients on a trial of observation or hormone-blocking (risk-reducing/prevention) treatment as opposed to more aggressive approaches that include radiation. Reasonably good performance for several positron emission mammography approaches has been described by Berg et al., including in DCIS (33,34). Active surveillance could be considered for surgery-averse women who are willing to be part of carefully controlled studies. The goal of using high-resolution nuclear imaging methods to assess the volume of tumor and the biologic phenotype may, although speculative, be reasonable as part of a more comprehensive, though still anatomically based, breast imaging strategy. If so, the contribution of nuclear breast imaging to primary tumor management, in comparison with conventional anatomic imaging–based management, may have a greater impact than we thought possible. We are a long way from this goal, but a start is in place in CALGB 40903: Phase II Single-Arm Study of Neoadjuvant Letrozole for ER(+) Postmenopausal DCIS. In this trial, led by Dr. Hwang from Duke, the goal is to move toward avoiding overtreatment of DCIS. The trial evaluates the response to neoadjuvant letrozole of estrogen receptor–positive DCIS with 1- to 5-cm calcifications as seen on MRI. It is possible that this sort of approach, informed by nuclear breast imaging, may move us to decrease the intensity of breast cancer treatment and perhaps decrease the overdiagnosis/overtreatment continuum.
A commentary by Joann Elmore in JAMA Internal Medicine clearly states the clinical conundrum faced by those caring for women with breast cancer: “Women will increasingly approach their physicians with questions and concerns about overdiagnosis, and we have no clear answers to provide. We do not know the actual percentage of overdiagnosed cases among women screened, and we are not able to identify which women with newly diagnosed DCIS or invasive cancer are overdiagnosed. Many screening guidelines now mandate shared and informed decision making in the patient-physician relationship, but this is not an easy task.” (35).
It is possible that anatomic screening methods may be detecting too many cancers and that we may not yet know how to make our treatments less aggressive. One could envision an imaging approach in which our goal is not to detect all cancers, something at which current breast imaging molecular approaches perform somewhat poorly, but to detect the cancers that truly matter and need more aggressive treatment. Movement in this direction would require a prospective randomized trial in which nuclear medicine breast imaging negative for cancer might be used in a follow-up setting after biopsy.
Dense Breasts
Mammography performs less well in women with dense breasts because of the high glandular density relative to tumor density. Breast density itself is also a risk factor for cancer. How women with dense breasts are best screened by imaging remains unclear. Ultrasound, radionuclide imaging, and MRI have all been considered. The anatomic methods have rather high false-positive rates.
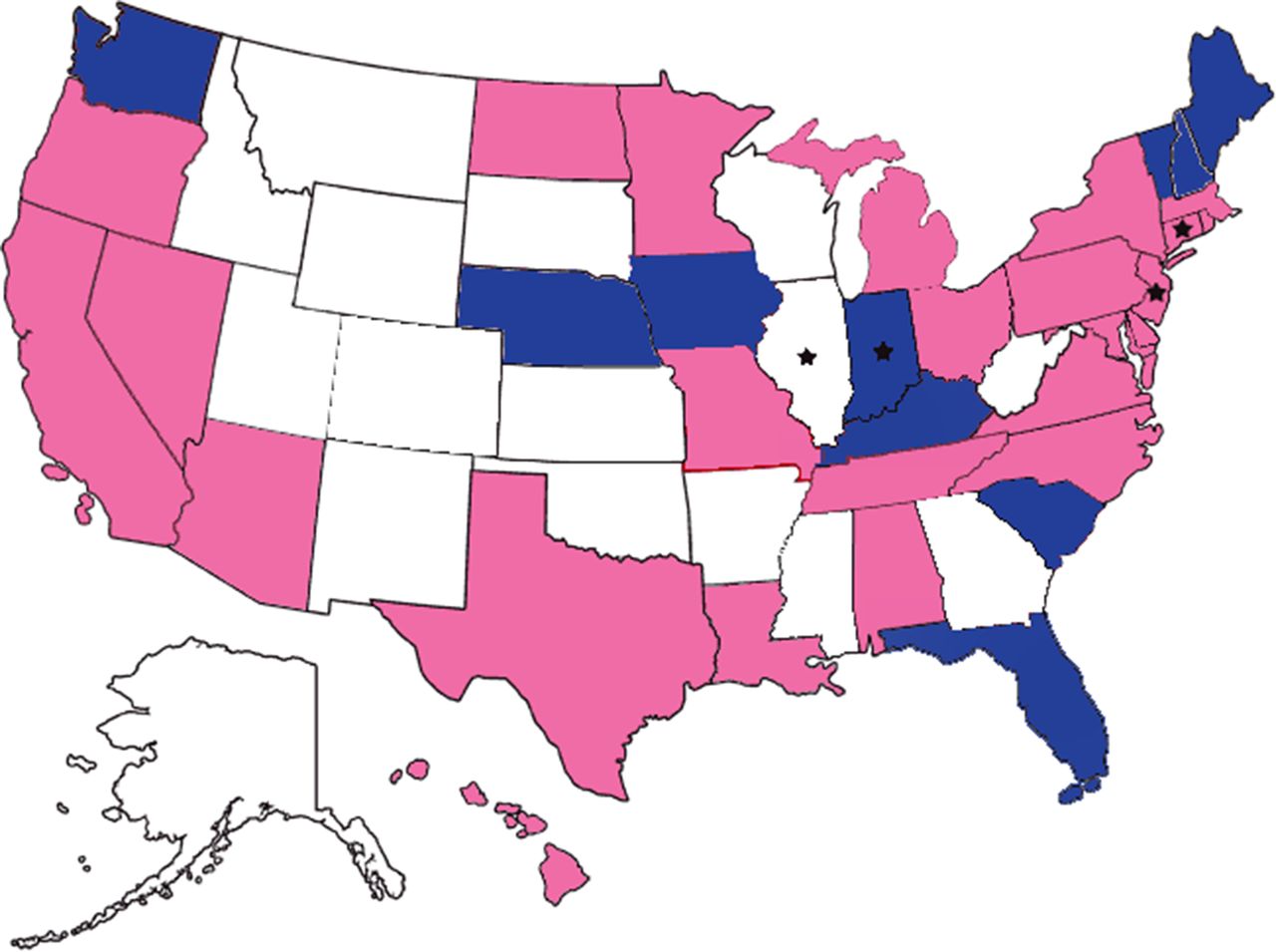
Consider the politics of dense breasts. Are You Dense Advocacy, Inc., is the government relations affiliate of Are You Dense, Inc. Per the organization’s website: “Our Mission [is]…To ensure that women with dense breast tissue have access to an early breast cancer diagnosis. To that end, women need to be informed of their breast density, the limitations of mammography to find cancer in dense breast tissue and the increased risk factor of dense breast tissue.” The organization’s goal is to advocate for and support state and federal legislative and regulatory efforts to standardize the communication of dense breasts to women and provide these women with access to reliable breast screening technologies. The organization’s website shows a U.S. map depicting states in which dense-breast legislation has been enacted or is being considered (Fig. 1). The map indicates that many women are being notified—because of legislation—that they have dense breasts and that their mammograms may not be adequate for diagnosis (36). What are these women’s options? The extent to which digital breast tomosynthesis may improve cancer diagnosis in this subgroup remains to be proven.

Map of United States showing states in which dense breast legislation has been enacted or is being considered. Pink = enacted law; blue = working on bill; ★ = insurance coverage law. (Reprinted with permission of (36).)
Adjunctive screening with breast sonography (handheld or automated) and breast MRI has been performed. Breast MRI screening may be warranted in women at significantly elevated risk of breast cancer (above that dictated by breast density). Screening with breast sonography is effective in increasing cancer detection but suffers from false-positives (37). Concerns about overdiagnosis with ultrasound have been raised, as well as about increased costs per cancer diagnosed and increased cancer (38,39). Tomosynthesis may be cost-effective in this group if the additional cost is reasonably low (40).
It is thus possible that either PET or molecular breast imaging could have a growing and important role in serving these 40% of women with dense breasts undergoing screening. Studies from over a quarter of a century ago and the more recent work of Berg et al. showed that in some of these women 18F-FDG PET could detect invasive cancers that were invisible on mammography. Pilot study data have shown that 99mTc-sestamibi breast imaging can detect cancers in women with dense breasts (41).
Breast ultrasound approaches are also an alternative, as is MR imaging of the breast. Unfortunately, in the absence of data, self-pay issues may prevent patients in most states from having access to other imaging methods. The high false-positive rate (positive predictive value, ∼9%) with sonography and other methods is also a limitation (42). Although MRI is a valuable tool for breast imaging, there are increasing concerns about intracranial gadolinium deposition, and it is not clear whether years of screening with gadolinium infusions is the best thing for younger women (19). The days of the National Science Foundation are behind us, we hope, but some caution is likely in order regarding the repeated use of “safe” MRI methods when the contrast agent may be retained for years in the brain. The biologically based methods of PET and molecular breast imaging are a compelling opportunity to shift the diagnostic receiver-operating-characteristic curve upward from its current anatomically based position in women with dense breasts but will deliver an additional radiation dose to these patients. Determining how nuclear methods can fit into this space represents a great opportunity for prospective study.
Screening and Diagnosis
Thoughts about primary breast cancer detection are quite disparate at present. On the one hand, there is a strong advocacy position recognizing that women with dense breasts are not well screened by mammography, but the optimal tool for them is not completely clear. On the other hand, there is a vocal discussion that existing screening programs for all women should be restricted to a more limited subset of patients, those over 50 and under 74, performed every other year (U.S. Public Health Service task force recommendation) versus annually (American Cancer Society and the American College of Gynecology recommendation), and that we may be detecting too many indolent breast cancers or overtreating them. We need prospective data that include nuclear imaging methods. We also could benefit from more widespread deployment and validation of radionuclide-based lesion localization.
Nodal Disease
Radionuclide lymphoscintigraphy with sentinel node identification is a technique superior to PET for detecting the presence of metastases to regional lymph nodes in the axilla. PET is unlikely to replace radionuclide lymphoscintigraphy. However, it is worth considering some specific settings in which PET may be valuable. For example, in the setting of neoadjuvant chemotherapy, 18F-FDG PET before treatment administration would ideally be explored in a prospective study to determine whether outcomes are improved by the diagnostic information provided. Such imaging data can help guide radiation therapy planning. Women with extensive nodal disease or distant metastases, or with internal mammary disease from medial breast cancers, are at a higher risk of death. Assessing the nodes after chemotherapy can be less informative, as the nodes can become histologically negative. Similarly, precise staging information may help inform patients about the best choices and timing as related to reconstructive surgery, for example. Most would agree that women with stage IV breast cancers are not optimal candidates for aggressive breast reconstructive surgery. Similarly, quantification of nodal SUV may be useful by virtue of its having a high positive predictive value for detecting axillary nodal metastases.
Therapy Monitoring
The literature on monitoring neoadjuvant therapy of breast cancer has continued to grow and lends itself to review and metaanalysis. Fifteen studies with 745 patients were assessed. The pooled sensitivity and specificity of 18F-FDG PET or PET/CT were 80.5% and 78.8%, respectively, and the positive and negative predictive values were 79.8% and 79.5%, respectively. After 1 and 2 courses of chemotherapy, the pooled sensitivities were 78.2% and 82.4%, respectively. These data, across a range of breast cancer histologies and therapeutic approaches, support the role of 18F-FDG PET for early and quite accurate assessment of the response to treatment (43).
We have a good but imperfect test for monitoring treatment response. It is time for us to begin to use sequential PET imaging to adjust treatment. For example, patients who fail to respond to neoadjuvant therapy with at least a 45% drop in SUV after 15 d could be changed to an alternative therapy, as they are unlikely to have a suitable pathologic complete response at the end of treatment. By contrast, it is possible that therapy could be deintensified in exceptional responders, reducing the number of cycles from 6 to 4, for example, to determine whether patients could be spared the toxicity and cost of therapy and still have a good outcome. PET with 18F-FDG can also lead to a more informed approach to monitoring systemic disease response. Clinical trials will help us in this space. Chemotherapy is not free, and giving more than is needed is not an optimal use of health-care resources.
These are preliminary steps, but we must begin to incorporate the readout data from our quantitative PET imaging into trial designs for breast cancer, just as we have done for lymphoma. A simple reduction of chemotherapy by 2 cycles could be beneficial to patients and society, potentially allowing resources to be reallocated.
Monitoring treatment of systemic disease is also assuming increasing importance as the therapeutic options for breast cancer continue to expand, now including more effective therapies for estrogen-receptor–positive neoplasms, more effective chemotherapy, and emerging immunotherapies. The known heterogeneity of tumors may be better probed using PET with 18F-FDG and other tracers than using other methods.
Surveillance
The current guidelines of the American Society of Clinical Oncology suggest no systemic imaging follow-up for patients with seemingly cured breast cancer. This very measured approach was based on the concern that false-positive studies were common and that treatments for metastatic breast cancer were not expected to be very effective—thus, there being little reason to find disease earlier. Such may have been the case, but treatments for breast cancer have improved greatly, and it is possible that outcomes may be better for patients with metastatic disease when it is recognized earlier. This possibility could likely be proven only in women with a higher probability of relapse from cancer, but as treatments improve we should not be limited to the historical immutability of the rapid demise of patients with metastatic breast cancer. Preventing pathologic fractures as the first sign of recurrence of disease is a desirable end, but there currently are not sufficient data to inform the use of PET in a surveillance setting. Thus, more intensive imaging-monitoring of patients at high risk of breast cancer recurrence should be considered in the modern era of improved treatments (44).
Alternative Tracers
18F-16α-fluoroestradiol (18F-FES), 3′-deoxy-3′-18F-fluorothymidine (18F-FLT), and agents imaging progesterone receptors are among several that have been investigated in breast cancer imaging but have not been fully evaluated or Food and Drug Administration–approved. However, as the use of hormonal therapies and phenotyping/prevention increases, it is possible these agents will have greater application and warrant definitive study (45–47). When used in difficult clinical cases of metastatic breast cancer, information obtained from 18F-FES PET changed management in nearly half of patients with metastatic breast cancer (47). Using 18F-FDG as a pharmacodynamic marker of estrogen receptor function may also be complementary in such a setting when phenotyping can be performed noninvasively (through estrogen stimulation) (48). A recent multicenter trial of 18F-FLT monitoring of neoadjuvant chemotherapy in 43 patients treated with a range of agents showed a drop in SUV to have some ability to predict the probability of achieving a pathologic complete response (49).
CONCLUSION
In the past 25-plus years, PET and single-photon methods have increasingly been deployed in breast cancer imaging. Anatomic methods such as digital mammography, tomosynthesis, and MRI have continued to improve and have advanced the field of primary breast cancer screening and diagnosis more than radionuclide methods have. As the whole approach to breast cancer screening, diagnosis, and therapy is being bombarded by concerns about overdiagnosis, underdiagnosis, and failure to detect cancers in women with radiographically dense breasts, it is important not to lose sight of how effective mammography has been in improving the outcomes of women in screened and diagnosed populations. That said, it is incumbent on investigators in breast imaging and investigators in nuclear medicine to come together and rationally and carefully evaluate the role of nuclear imaging in scientific investigations to benefit women (and the rare man) with or at risk of breast cancer.
The role of nuclear methods in primary breast cancer has not grown rapidly, in part because of the limited image resolution, unfavorable radiation dosimetry, and lack of evidence-based clarity on the best specific uses. The breast imaging community has had many new tools at its disposal and has made considerable progress by growing the use of digital mammography, tomosynthesis, MRI, ultrasound, and contrast mammography.
Nuclear methods may help in the screening of the large population of higher-risk women with dense breasts in a way not possible with anatomic methods. Nuclear molecular imaging approaches may ultimately help us identify the cancers that truly matter and guide their treatment, both locally and systemically, with maximal efficiency while minimizing morbidity and resource use. Although careful prospective studies are required, it is possible that the practice of breast imaging may be constructively disrupted through the use of more biologically relevant nuclear imaging, hopefully to the benefit of our patients. It was not many years ago that radical mastectomy was the norm—a procedure that has now virtually disappeared. It is quite possible that, informed by data, the approaches to imaging breast cancer will change just as substantially over the coming years and that radionuclide molecular imaging will play an important and growing role as we move toward precision imaging for detecting breast cancer and guiding its treatment.
DISCLOSURE
This work was supported in part by NCI U01 CA140204. No other potential conflict of interest relevant to this article was reported.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.





{kind=link}