


Abstract
18F-labeled 1-amino-3-fluorocyclobutane-1-carboxylic acid (18F-fluciclovine) is a leucine analog PET/CT radiotracer that depicts amino acid transport into cells. Amino acid transport proteins have been shown to be upregulated in breast malignancies by microarray and immunohistochemical analysis, so we hypothesized that 18F-fluciclovine may provide a novel method of visualizing breast cancer and now report a prospective clinical trial of 18F-fluciclovine PET/CT in newly diagnosed advanced local invasive ductal carcinoma (IDC) and invasive lobular carcinoma (ILC). Methods: Twenty-seven women with a new diagnosis of locally advanced IDC (n = 19) or ILC (n = 8) underwent PET/CT of the chest after intravenous administration of 370 MBq of 18F-fluciclovine. The SUVmax, SUVmean, metabolic tumor volume, and total lesion avidity were obtained for the primary breast tumor, axillary lymph nodes, and extraaxillary lymph nodes. Sites of previously unsuspected malignancy were recorded and confirmed by pathology. Results of 18F-fluciclovine PET/CT were compared with those of 18F-FDG PET/CT, when available, using the concordance correlation coefficient. Results: All locally advanced breast cancers were 18F-fluciclovine–avid. Of 21 patients with pathologically proven axillary nodal metastases, 18F-fluciclovine–avid axillary nodes were seen in 20. 18F-fluciclovine detected pathologically proven extraaxillary nodal metastases in 3 patients, including 2 previously unsuspected internal mammary nodes. Fourteen patients underwent 18F-FDG PET/CT for comparison with 18F-fluciclovine. Concordance for metabolic tumor volume between 18F-fluciclovine and 18F-FDG was strong (concordance correlation coefficient, 0.89; 95% confidence interval, 0.73–0.96), but concordance for SUVmax was weak (concordance correlation coefficient, 0.04; 95% confidence interval, −0.16–0.24). In patients with both modalities available (n = 14), primary ILCs (n = 4) demonstrated 18F-fluciclovine avidity (median SUVmax, 6.1; range, 4.5–10.9) greater than 18F-FDG avidity (median SUVmax, 3.7; range, 1.8–6.0). Primary IDCs (n = 10) had a lower 18F-fluciclovine avidity (median SUVmax, 6.8; range, 3.6–9.9) than 18F-FDG avidity (median SUVmax, 10; range, 3.3–43.5). Conclusion: 18F-fluciclovine PET/CT demonstrates potential for imaging of both IDC and ILC, including the detection of unsuspected extraaxillary nodal metastases. The low concordance for SUVmax between 18F-fluciclovine and 18F-FDG suggests that these tracers measure different biologic phenomena within the tumor. The apparently higher uptake of 18F-fluciclovine in ILC requires confirmation in a larger cohort.
PET with 18F-FDG has made important advances in the care of patients with breast cancer (1); however, 18F-FDG PET has multiple limitations, including the inability to differentiate malignant from benign breast lesions (2), limited contribution to local staging of the breast and axillary nodes (3–5), and variable sensitivity for breast cancer depending on tumor and patient factors (6–8). Invasive lobular carcinoma (ILC), a subtype of breast cancer, is difficult to visualize by all known imaging modalities (9,10), including 18F-FDG PET (11–16). Thus, there is a continued need for the development of better metabolic imaging agents for breast cancer, particularly for ILC.
Amino acid transport is highly upregulated in breast cancers as compared with normal breast epithelium by microarray and immunohistochemical analysis (17), suggesting that imaging agents for breast malignancies based on amino acid metabolism may be useful. 18F-labeled 1-amino-3-fluorocyclobutane-1-carboxylic acid (18F-fluciclovine, also known as 18F-FACBC) is a leucine analog PET/CT radiotracer that depicts amino acid transport and is under investigation as a tumor-targeting agent (18–22). We hypothesized that the upregulation of genes for amino acid transport proteins in breast cancer will favor enhanced 18F-fluciclovine uptake and allow for clinically valuable imaging in this tumor type. In this article, we report our initial results of 18F-fluciclovine PET/CT from a prospective clinical trial of patients with the 2 most common subtypes of breast cancer, invasive ductal carcinoma (IDC), which accounts for approximately 75%–80% of primary breast malignancies, and ILC, which accounts for approximately 10%–15% (23).
MATERIALS AND METHODS
Study Design and Patients
This prospective clinical trial was performed with institutional review board approval and written informed consent from participants. Patients presenting for evaluation at Memorial Sloan Kettering Cancer Center with biopsy-proven locally advanced, nonmetastatic, IDC or ILC who were referred for neoadjuvant systemic therapy between August 2013 and August 2015 were invited to participate. This patient population allows for an initial evaluation of 18F-fluciclovine avidity in larger tumors. Exclusion criteria were age younger than 18 y, current pregnancy or lactation, prior malignancy other than squamous or basal skin cancers, and patients unwilling or unable to consent. There were no restrictions on sex or race. ILC patients were actively sought, which accounts for the higher prevalence of ILC in our cohort than in the overall breast cancer population. Clinical records were used to document patient age, sex, race, and presence of biopsy-proven known axillary or extraaxillary nodal metastases before 18F-fluciclovine PET/CT as well as histology, grade, and receptor status of the primary breast malignancy. Tumors were hormone receptor–positive if they stained as estrogen receptor greater than 1% or progesterone receptor greater than 1%. Tumors were human epidermal growth factor receptor 2–positive if they were immunohistochemistry 3+ or fluorescent in situ hybridization amplified with ratio of > / = 2.0.
18F-Fluciclovine Production
18F-fluciclovine was manufactured in compliance with current good manufacturing practice requirements at the Memorial Sloan Kettering Cancer Center Radiochemistry and Molecular Imaging Probes Core Facility. The FASTlab automated synthesizer, synthesizer cassettes, reagents, and materials were all supplied by GE Healthcare as previously described (24). The automated synthesis involved nucleophilic incorporation of 18F-fluoride into the 18F-fluciclovine precursor, followed by removal of protective groups using hydrolysis and terminal sterilization with a 0.22-μm sterilizing filter. The 18F-fluciclovine final drug product was formulated with 200 mM citrate buffer solution. All manufactured 18F-fluciclovinedrug product batches were quality control tested to ensure conformance with the acceptance specifications for pH, appearance, radiochemical purity, radiochemical identity, radionuclidic identity, endotoxin levels, sterilizing filter integrity, and residual solvent levels before release for patient administration.
18F-Fluciclovine PET/CT Imaging and Image Interpretation
Enrolled patients underwent 18F-fluciclovine PET/CT before initiation of therapy. There was no patient-specific preparation before 18F-fluciclovine administration, and patients were allowed to eat and drink before the PET/CT examination, in contrast to previous work in prostate cancer (21). Patients were positioned on designated research PET/CT scanners, either a Discovery STE or a GE Discovery 710 (GE Healthcare), operated in 3-dimensional mode. The 18F-fluciclovine PET studies were performed as hybrid PET/CT examinations for attenuation correction, lesion localization, and availability of additional CT data. A low-milliampere CT (60–80 mA) of the chest was acquired first. Then a bolus of 370 MBq (10 mCi) ± 10% of 18F-fluciclovine was administered intravenously in under 10 s. Dynamic PET imaging over the chest was acquired for 30 min, with data collected for each minute, then summed into 5-min intervals. 18F-fluciclovine avidity was most often greatest during the 5- to 10-min time interval, and therefore quantitative analyses of 18F-fluciclovine avidity were conducted using the data collected during this time interval. The 18F-fluciclovine PET/CT images were reconstructed using iterative reconstruction and displayed on a PET/CT workstation (PET VCAR; GE Healthcare) in multiplanar reconstructions. Areas of focal tracer uptake were localized using the companion CT and classified as lesions of the breast, axillary nodes, or extraaxillary lesions. Three-dimensional regions of interest were placed in areas of tracer uptake, and measures of 18F-fluciclovine avidity were recorded, including SUVmax (body weight), metabolic tumor volume (MTV) (cubic centimeter volume of tumor with SUV greater than 42% of SUVmax), SUVmean (within the MTV), and total lesion avidity (TLA = MTV × SUVmean).
Comparison 18F-FDG PET/CT Imaging and Image Interpretation
Although not prescribed as part of the clinical trial, some patients underwent 18F-FDG PET/CT as part of their standard clinical care before initiation of therapy. Patients fasted for at least 6 h before the 18F-FDG PET/CT scan. Each patient was injected intravenously with 444 MBq (12 mCi) of 18F-FDG when plasma glucose was less than 200 mg/dL. After 18F-FDG injection, patients rested for a scheduled 60-min uptake period, followed by image acquisition. PET/CT scans were acquired with the patient supine from the base of the skull to the mid thigh. A low-dose CT scan with oral contrast was obtained. 18F-FDG PET/CT images were reconstructed using iterative reconstruction and displayed on a PET/CT workstation (PET VCAR) in multiplanar reconstructions. Areas of focal tracer uptake were localized using the companion CT and classified as lesions of the breast, axillary nodes, or extraaxillary lesions. Three-dimensional regions of interest were placed in areas of tracer uptake, and measures of 18F-FDG avidity were recorded, including SUVmax (body weight), MTV (volume of tumor with SUV greater than 42% of SUVmax), SUVmean (within the MTV), and total lesion glycolysis (TLG = MTV × SUVmean).
Verification of Malignancy
All patients had biopsy-proven primary breast malignancy before enrollment in the clinical trial. Pathology for axillary nodes was also available for all patients. Pathologic evaluation of extraaxillary nodes was also available for the 3 patients with suspicious extraaxillary findings on 18F-fluciclovine PET/CT.
Statistical Analysis
Descriptive statistics were calculated for patient characteristics and measures of 18F-FDG avidity. Measures of 18F-FDG avidity were descriptively compared for patients with IDC and ILC and graphically demonstrated using box plots. In those with 18F-FDG scans, agreement between 18F-fluciclovine and 18F-FDG was calculated using the concordance correlation coefficient along with 95% confidence intervals. The agreement was also graphically illustrated using scatterplots with the line of perfect concordance versus the empiric least-squares model line. All analyses were performed using SAS 9.4 (The SAS Institute) and R 3.1.2 with the “epiR” package (The R Foundation).
RESULTS
Twenty-seven female patients were prospectively accrued to the institutional review board–approved protocol and underwent 18F-fluciclovine PET/CT. The median age of the cohort was 52.7 y (range, 37.3–79.1 y). The histology of the primary breast malignancy was IDC in 19 patients (70%) and ILC in the remaining 8 patients (30%). ILC patients were actively sought for inclusion into the study, which accounts for the higher prevalence of ILC in our cohort than in the overall breast cancer population. Patient and tumor characteristics are summarized in Table 1. All 27 patients underwent 18F-fluciclovine PET/CT before initiation of therapy. Physiologic 18F-fluciclovine uptake was seen in the liver, pancreas, and skeletal muscle, as previously reported (20). Uptake in presumably normal breast tissue was low in all patients, ranging from SUVmax 0.5 to 1.5. 18F-fluciclovine–avid lesions were observed in the breast, axillary nodes, and extraaxillary nodes.
Patient and Tumor Characteristics
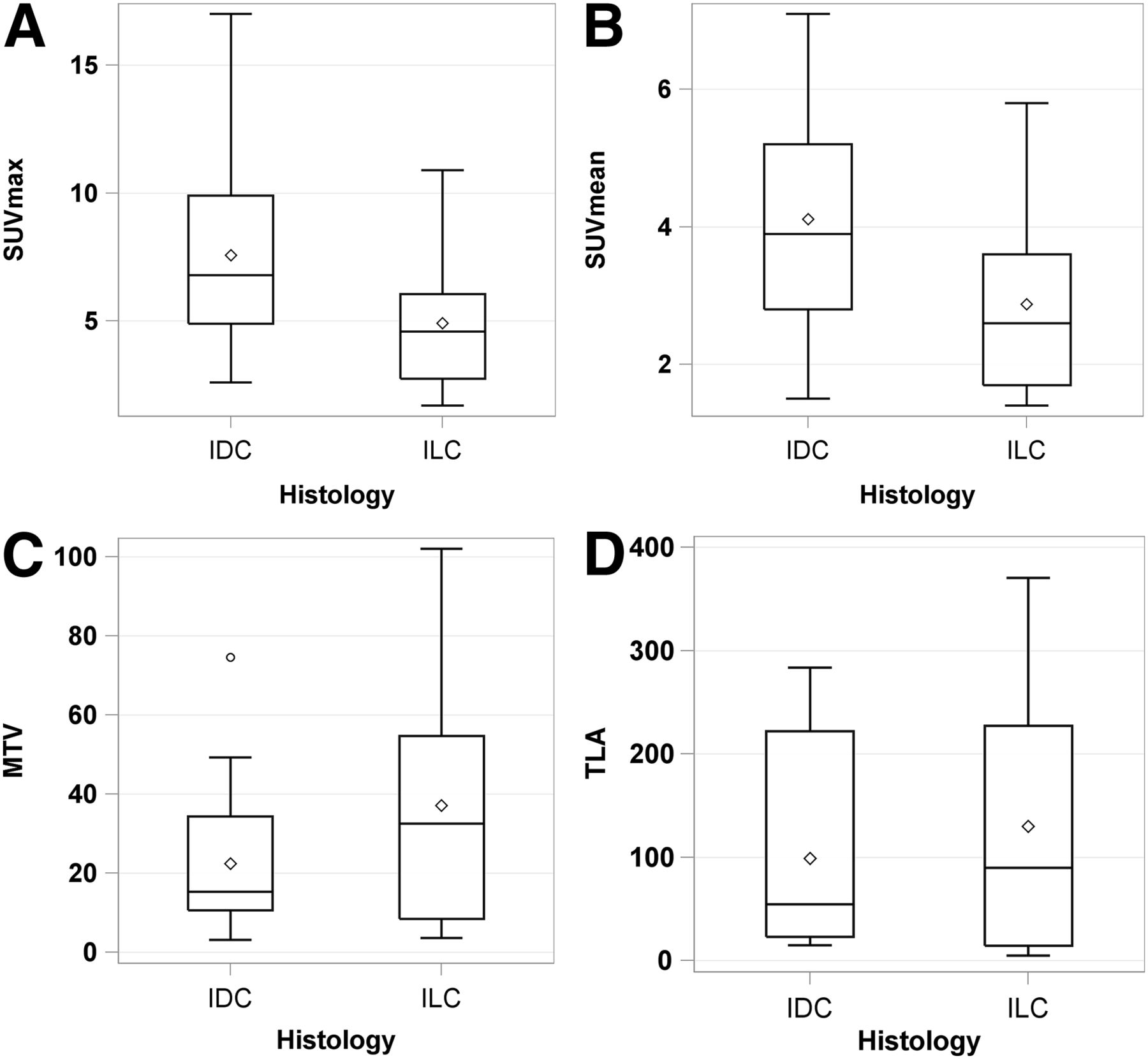
For the primary breast malignancies, all 27 locally advanced breast cancers were 18F-fluciclovine–avid above local breast background. Median SUVmax was 5.9 (range, 1.7–17.0). Values for SUVmax, SUVmean, MTV, and TLA of the primary breast malignancies for the entire cohort, as well as categorized by histology, are provided in Table 2. The distribution of these measures of 18F-fluciclovine avidity is graphically depicted in Figure 1.
Measurements of 18F-Fluciclovine Avidity in Primary Breast Malignancies, Axillary Nodes, and Extraaxillary Nodes
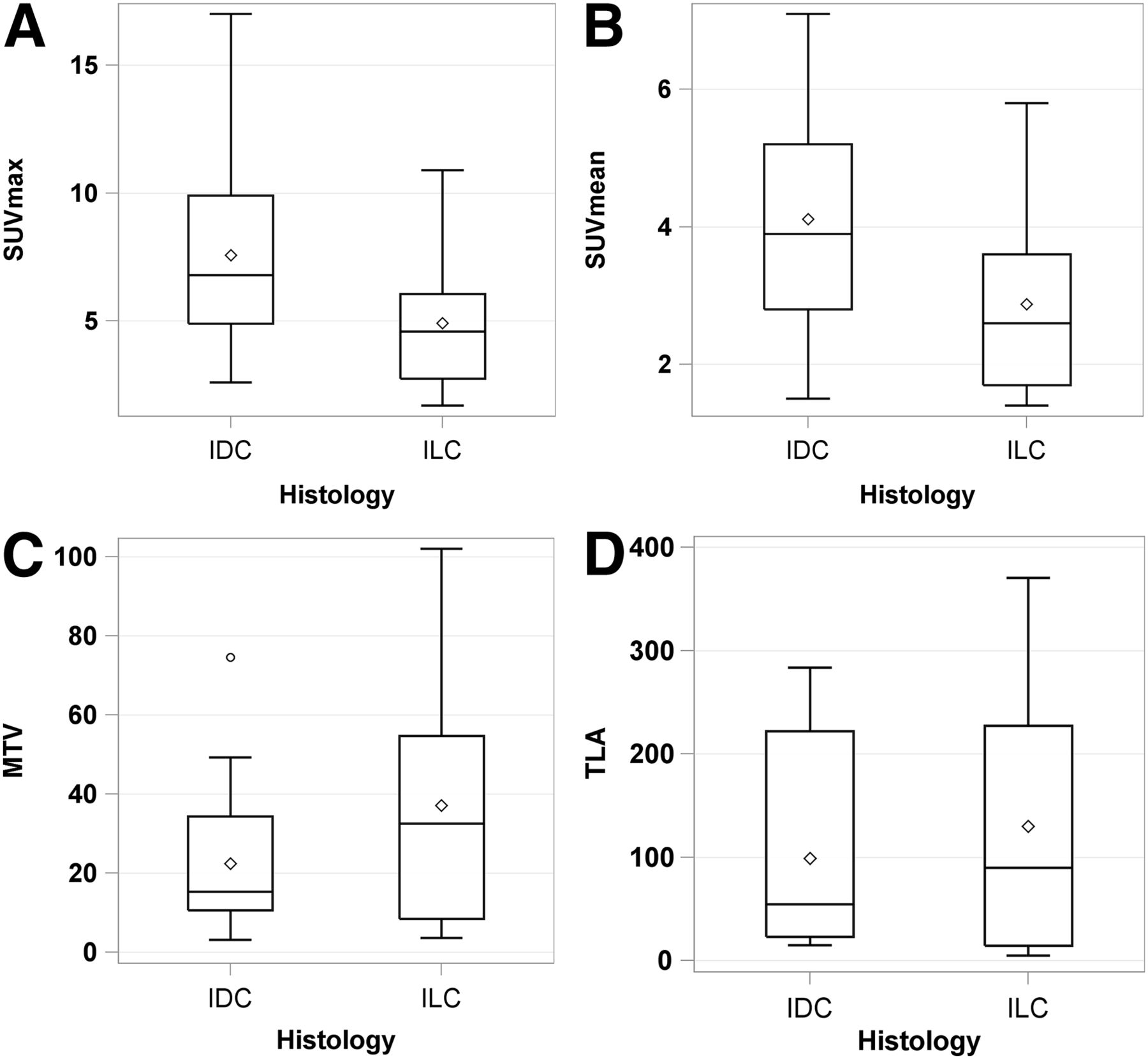
Distribution of measures of 18F-fluciclovine avidity in 27 primary breast malignancies. Tukey box and whisker plots are displayed for SUVmax (A), SUVmean (B), MTV (C), and TLA (D) for IDC and ILC histologies. These plots are a schematic for distribution of values. Ends of box represent 25th and 75th percentiles (or first and third quartiles), whereas center line and diamond represent median and mean, respectively. 75th minus 25th percentile equals interquartile range, and ends of whiskers are placed at 1.5 times interquartile range. Any values lying outside these boundaries are considered outliers (for example, circle in MTV plot).
For axillary nodal metastases, 21 of 27 patients had pathologically proven axillary nodal metastases, including 16 of 19 patients with IDC and 5 of 8 patients with ILC. 18F-fluciclovine PET/CT demonstrated axillary nodes that were 18F-fluciclovine–avid above local background in 20 of 21 patients with pathologically proven axillary nodal metastases, including all 16 patients with IDC and 4 of 5 patients with ILC. There were no 18F-fluciclovine–avid axillary nodes in patients without pathologically proven axillary nodal metastases. In patients with 18F-fluciclovine–avid nodes, the number of nodes ranged from 0 to 10 (median, 2). Values for SUVmax, SUVmean, MTV, and TLA of the axillary nodal metastases for the entire cohort, as well as categorized by histology, are provided in Table 2.
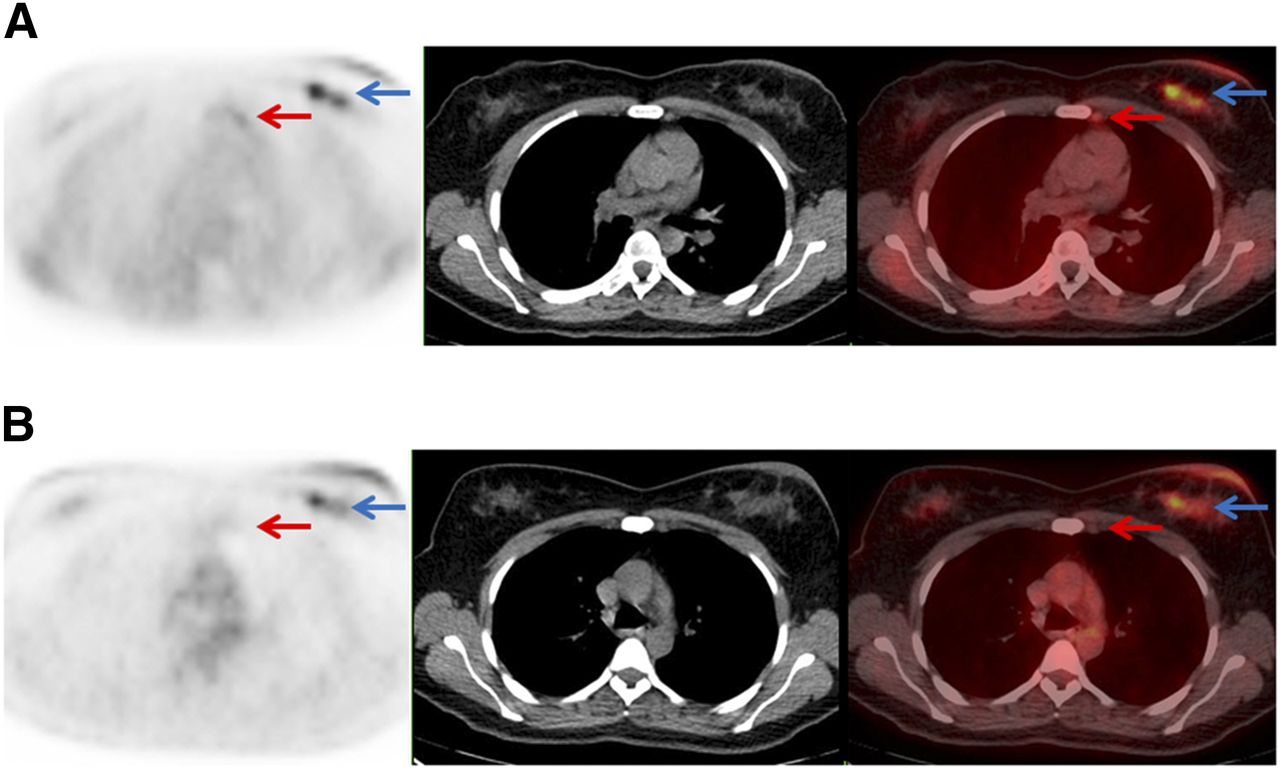
For extraaxillary nodal metastases, 3 of 27 patients had pathologically proven extraaxillary nodal metastases, and all 3 were patients with IDC. Two patients had unsuspected 18F-fluciclovine–avid internal mammary nodes, which were subjected to fine-needle aspiration, confirming malignancy in each case. An example of a patient with an internal mammary nodal metastasis first detected on 18F-fluciclovine PET/CT is shown in Figure 2. A corresponding 18F-FDG PET/CT scan, obtained before 18F-fluciclovine PET/CT in this case, did not appreciate the internal mammary nodal metastasis. Values for SUVmax, SUVmean, MTV, and TLA of the extraaxillary nodal metastases for the entire cohort, and by histology, are provided in Table 2. No distant metastases were detected on 18F-fluciclovine PET/CT.
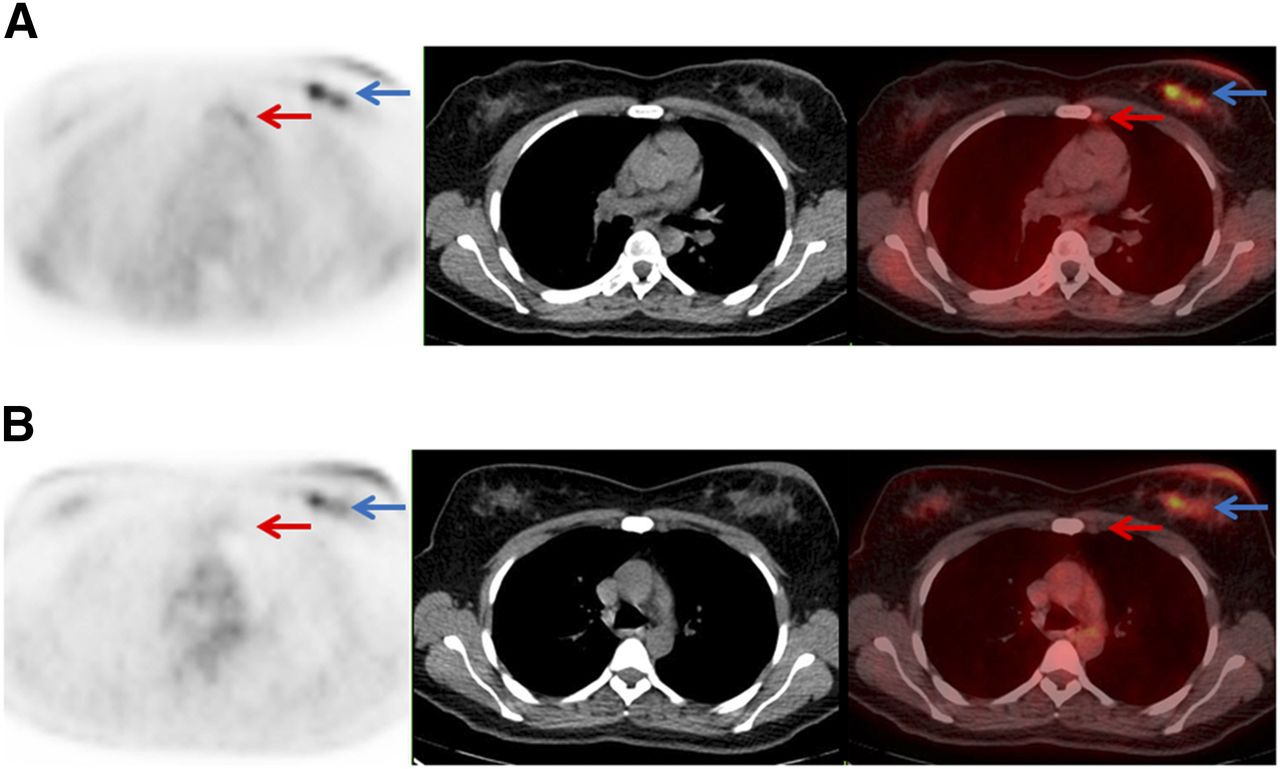
A 48-y-old woman with estrogen receptor–positive human epidermal growth factor receptor 2–negative IDC. (A) Axial 18F-fluciclovine PET, CT, and fused 18F-fluciclovine PET/CT demonstrating primary left breast malignancy (blue arrow; SUVmax, 7.5) and internal mammary nodal metastasis that was subsequently biopsy-proven (red arrow; SUVmax, 2.4). Axillary (SUVmax, 7.4) and supraclavicular (SUVmax, 4.2) nodal metastases were also detected (not shown). (B) Axial 18F-FDG, CT, and fused 18F-FDG PET/CT demonstrating primary left breast malignancy (blue arrow; SUVmax, 4.0) as well as axillary (SUVmax, 5.2) and supraclavicular (SUVmax, 2.8) nodal metastases (not shown); however, internal mammary nodal metastasis (red arrow; SUVmax, 0.7) was not appreciated on initial review of 18F-FDG PET/CT.
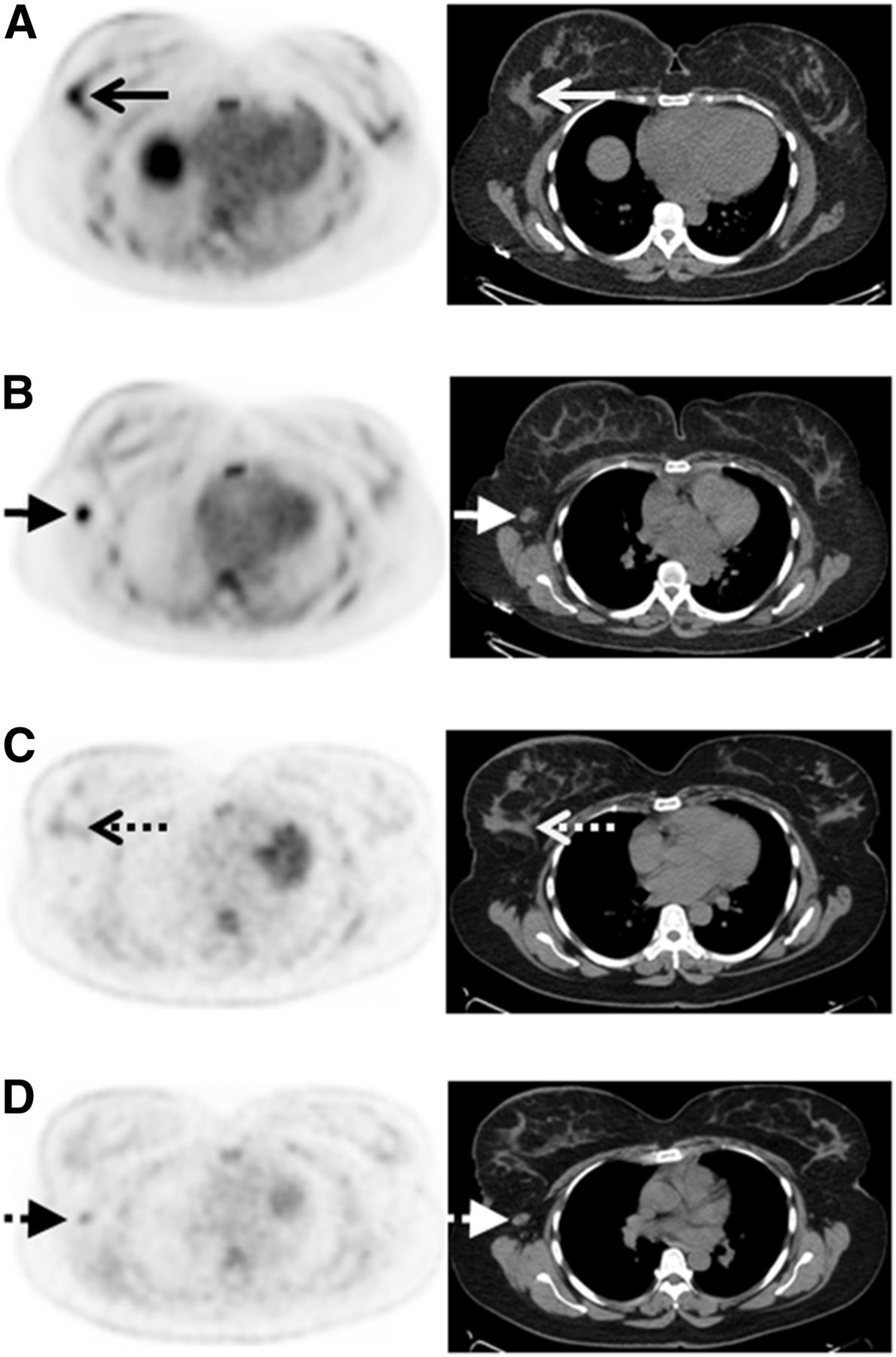
Of the 27 enrolled patients, 14 also underwent 18F-FDG PET/CT as part of their standard clinical care before initiation of therapy, enabling a comparison of measures of 18F-fluciclovine and 18F-FDG avidity in lesions identified in these cases. Values for SUVmax, SUVmean, MTV, and TLA/TLG of the primary breast malignancies, axillary nodes, and extraaxillary nodes for the 14 patients who underwent both PET/CT studies are provided in Table 3. For all 4 patients with ILC, 18F-fluciclovine avidity was greater than 18F-FDG avidity. An example of a patient with ILC with greater 18F-fluciclovine avidity than 18F-FDG avidity is shown in Figure 3. For the 10 patients with IDC, 18F-fluciclovine avidity was generally lower than 18F-FDG avidity. 18F-fluciclovine SUVmax ranged from 3.3 to 9.9 (median, 6.8), whereas 18F-FDG avidity ranged from 3.3 to 43.5 (median, 10.0).
Measurements of 18F-Fluciclovine and 18F-FDG Avidity in Primary Breast Malignancies, Axillary Nodes, and Extraaxillary Nodes of 14 Patients Who Underwent Both 18F-Fluciclovine PET/CT and 18F-FDG PET/CT

A 43-y-old woman with estrogen receptor–positive human epidermal growth factor receptor 2–negative ILC, which was more 18F-fluciclovine–avid than 18F-FDG–avid. (A) Axial 18F-fluciclovine PET/CT demonstrates 18F-fluciclovine–avid (SUV, 4.9) primary right breast malignancy (arrows). (B) Axial 18F-fluciclovine PET/CT demonstrates 18F-fluciclovine–avid (SUV, 5.8) right axillary nodal metastasis (short arrows). (C) Axial 18F-FDG PET/CT demonstrates near background 18F-FDG avidity (SUV, 1.8) in right breast malignancy (dashed arrows). (D) Axial 18F-FDG PET/CT demonstrates only mild 18F-FDG avidity (SUV, 2.8) in right axillary nodal metastasis (short dashed arrows).
The concordance between 18F-fluciclovine and 18F-FDG was extremely weak for both SUVmax and SUVmean (concordance correlation coefficient [CCC], 0.04 and 0.08, respectively; 95% confidence interval, −0.16–0.24 and −0.21–0.36, respectively). However, the concordance between 18F-FDG MTV and 18F-fluciclovine MTV was strong (CCC, 0.89; 95% confidence interval, 0.73–0.96). The concordance between 18F-FDG TLG and 18F-fluciclovine TLA was moderate (CCC, 0.57; 95% confidence interval, 0.20–0.80). Concordance plots provide a graphical depiction of the data, as shown in Figure 4. If there was perfect concordance between 18F-fluciclovine and 18F-FDG, then the least-squares regression line would approach the line of perfect concordance, and the values would congregate around these lines. For example, the least-squares regression line for 18F-fluciclovine MTV and 18F-FDG MTV approaches the line of perfect concordance, demonstrating excellent concordance in the measurement of metabolic tumor volumes.
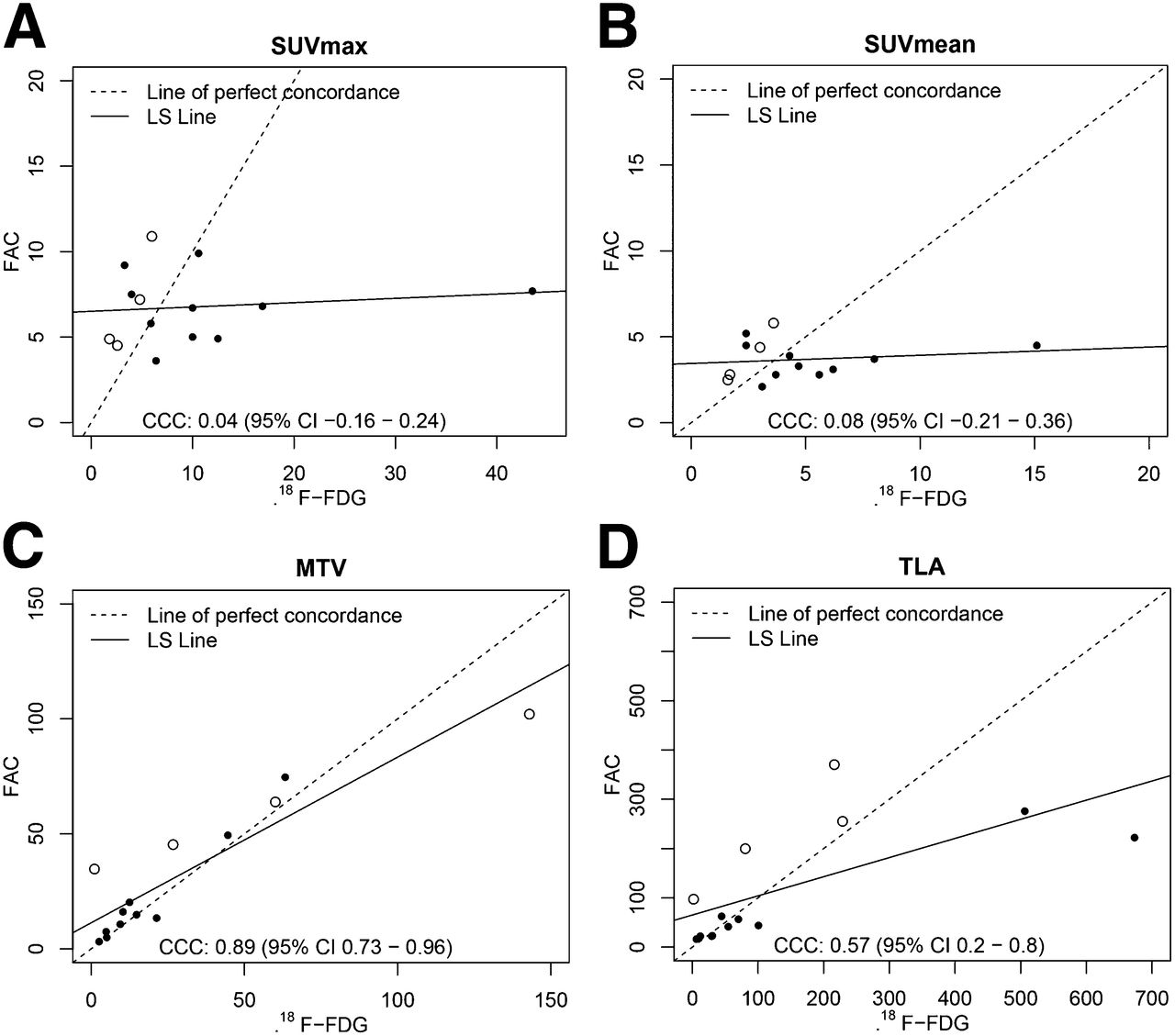
Concordance of 18F-fluciclovine and 18F-FDG SUVmax in 14 primary breast malignancies. Scatterplots for 18F-fluciclovine versus 18F-FDG, along with least-squares regression line (LS lines) and lines of perfect concordance, are displayed for SUVmax (A), SUVmean (B), MTV (C), and TLA/TLG (D). Filled in circles represent IDC histology and open circles represent ILC histology. Line of perfect concordance represents condition in which 18F-fluciclovine and 18F-FDG values are exactly equal to each other. LS line represents fit of linear regression model for F18F-DG and 18F-fluciclovine. Closer LS line is to line of perfect concordance, the stronger the agreement between 18F-fluciclovine and 18F-FDG values. CCC is measure of agreement between 18F-fluciclovine and 18F-FDG. It takes into account both correlation and accuracy between measurements. CCC values closer to zero are weak, and values closer to 1 are strong. FAC = 18F-fluciclovine.
DISCUSSION
We hypothesized that the upregulation of amino acid transport proteins in breast cancer could favor enhanced 18F-fluciclovine uptake and allow for clinically valuable imaging.
The results of the study tend to support the hypothesis but need to be confirmed in a larger series.
The locally advanced breast malignancies in this trial were all detected by 18F-fluciclovine. The larger size of these primary malignancies aided detection, but the ability to detect earlier stage breast cancer is unknown and requires additional investigation.
The ability of 18F-fluciclovine to detect axillary nodal metastases was also high in these patients with locally advanced malignancies. Detection of axillary metastases in earlier stage breast cancer requires further investigation. 18F-fluciclovine PET/CT detected internal mammary nodal metastases that were previously unsuspected. In this respect, it was similar to 18F-FDG PET/CT, which is proven to detect unsuspected extraaxillary nodal metastases in locally advanced breast malignancies (25). There was even 1 case in which 18F-fluciclovine PET/CT detected an internal mammary node, subsequently proven to be a metastasis, which was not detected on 18F-FDG PET/CT. The small sample size limits the significance of this finding.
No distant metastases were detected in this trial. The detection of distant metastases was limited by the restriction of imaging to include only the chest. 18F-fluciclovine has prominent physiologic hepatic uptake, which may make detection of liver metastases challenging, although lung, brain, and bone lesions may be readily visible.
It is interesting to compare 18F-fluciclovine avidity and 18F-FDG avidity in these breast malignancies. The concordance for MTV was strong, suggesting that the tracers identify a similar volume of metabolically active tumor; however, the concordance for SUVmax was low, suggesting that the tracers indeed measure different metabolic processes within these tumors. This raises the possibility that different subtypes of breast cancer may favor uptake of different tracers. For example, of the 4 patients with ILC who underwent both 18F-fluciclovine and 18F-FDG scans, all demonstrated 18F-fluciclovine avidity greater than 18F-FDG avidity. Future studies will be needed to understand the concordance between 18F-fluciclovine and 18F-FDG in ILC patients.
The strength of this study is its design as a prospective clinical trial, which decreases study biases and allows continued follow-up of a well-defined cohort. Its obvious weakness is its small numbers. These preliminary results are encouraging, but larger studies will be needed to further evaluate the place of 18F-fluciclovine for the PET/CT imaging of breast cancer.
CONCLUSION
18F-fluciclovine PET/CT demonstrates potential for imaging of both IDC and ILC, including the detection of unsuspected extraaxillary nodal metastases. Uptake of the amino acid analog 18F-fluciclovine does not parallel uptake of 18F-FDG and thus provides a measure of a different metabolic process. ILCs were more 18F-fluciclovine–avid than 18F-FDG–avid, an observation that merits further study in a larger cohort.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. We acknowledge financial support from the Susan G. Komen for the Cure Research grant KG110441 (GAU) and GE Healthcare as well as support from the MSKCC Biostatistics Core and Radiochemistry & Molecular Imaging Probe Core (P30 CA008748) and the MSKCC Breast Cancer Research Fund. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Dr. Penny Ward from Blue Earth Diagnostics and Dr. Eugene Teoh from Oxford University for providing helpful comments on the manuscript.
Footnotes
Published online Mar. 3, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication November 25, 2015.
- Accepted for publication February 17, 2016.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- WNT4 regulates cellular metabolism via intracellular activity at the mitochondria in breast and gynecologic cancers
- Riluzole suppresses growth and enhances response to endocrine therapy in ER+ breast cancer
- WNT4 executes estrogen regulation of cellular metabolism via intracellular activity at the mitochondria
- Detection of Additional Primary Neoplasms on 18F-Fluciclovine PET/CT in Patients with Primary Prostate Cancer
- Head-to-Head Evaluation of 18F-FES and 18F-FDG PET/CT in Metastatic Invasive Lobular Breast Cancer
- Update on 18F-Fluciclovine PET for Prostate Cancer Imaging
- Prospective Clinical Trial of 18F-Fluciclovine PET/CT for Determining the Response to Neoadjuvant Therapy in Invasive Ductal and Invasive Lobular Breast Cancers
- 18F-Fluciclovine (FACBC) and Its Potential Use for Breast Cancer Imaging