


Abstract
Patients with suspected recurrence from differentiated thyroid carcinoma, based on an increased thyroglobulin (Tg) level and negative neck ultrasound (US), pose a clinical dilemma. Because standard imaging has a low yield identifying potential recurrence, blind 131I treatment is often applied. However, a tumor-negative 131I whole-body scintigraphy (WBS) prevails in 38%–50% of patients. We performed a prospective multicenter observational cohort study to test the hypothesis that 124I PET/CT can identify the patients with a tumor-negative posttherapy 131I WBS. Methods: Our study was designed to include 100 patients with detectable Tg and a negative neck US, who were planned for blind 131I therapy. All patients underwent 124I PET/CT after administration of recombinant human thyroid-stimulating hormone. Subsequently, after 4–6 wk of thyroid hormone withdrawal patients were treated with 5.5–7.4 GBq of 131I, followed by WBS a week later. The primary endpoint was the number of 131I therapies that could have been omitted using the predicted outcome of the 124I PET/CT, operationalized as the concordance of tumor detection by 124I PET/CT, using post-131I therapy WBS as the reference test. The study would be terminated if 3 patients had a negative 124I PET/CT and a positive posttherapy 131I scan. Results: After inclusion of 17 patients, we terminated the study preliminarily because the stopping rule had been met. Median Tg level at 131I therapy was 28 μg/L (interquartile range, 129). Eight posttherapy WBS were negative (47%), all of which were correctly predicted by negative 124I PET/CT. Nine posttherapy WBS showed iodine-avid tumor, of which 4 also had positive 124I PET/CT findings. Sensitivity, specificity, negative predictive value, and positive predictive value of 124I PET/CT were 44% (confidence interval [CI], 14%–79%), 100% (CI, 63%–100%), 62% (CI, 32%–86%), and 100% (CI, 40%–100%), respectively. Implementation of 124I PET in this setting would have led to 47% (8/17) less futile 131I treatments, but 29% of patients (5/17) would have been denied potentially effective therapy. Conclusion: In patients with biochemical evidence of recurrent differentiated thyroid carcinoma and a tumor-negative neck US, the high false-negative rate of 124I PET/CT after recombinant human thyroid-stimulating hormone 124I PET/CT as implemented in this study precludes its use as a scouting procedure to prevent futile blind 131I therapy.
Differentiated thyroid cancer (DTC) incidence is rising, and it is the most prevalent endocrine cancer. Although patients have an excellent 10-y survival rate of higher than 95% (1,2), up to 25% of patients will face recurrent locoregional disease or distant metastasis (3). Prognosis is less favorable when recurrences and metastases occur (1). When recurrence is suspected based on serum thyroglobulin (Tg) levels, without clinical evidence of locoregional metastasis, patients are treated empirically with high-dose 131I (4,5). However, this blind therapy can be considered as futile in the 38%–50% of patients with a tumor-negative posttherapeutic whole-body scintigraphy (WBS) (6–9). On top of that, 131I therapy induces substantial short- and long-term morbidity due to hormone withdrawal–associated hypothyroidism and early and late sialoadenitis in up to 30%, which can lead to xerostomia, dental cariës, and stomatitis (10,11). Moreover, societal costs are considerable because of productivity loss (12,13). Therefore, there is a need for a diagnostic modality to predict which patients are likely to benefit from high-dose 131I therapy. The yield of low-dose 131I and of 123I WBS in this setting is low so that they are no longer recommended (14–17).
124I PET/CT has been investigated in DTC patients for several years (18–20). Apart from the superior imaging characteristics of PET (compared with SPECT), 124I PET/CT offers lower radiation exposure for the patient in comparison to blind 131I therapy, and it may be a tool for pretherapeutic dosimetry (8,18,21). Taken together, 124I PET/CT potentially allows for accurate restaging of DTC, prediction of 131I therapy outcome, and better selection of patients for 131I treatment. However, prospective studies with clear eligibility criteria and standardized procedures, comparing 124I PET/CT outcomes with posttherapy 131I WBS in patients treated blind with 131I, are lacking.
Iodine uptake in metastases can be stimulated exogenously, using recombinant human thyroid-stimulating hormone (rhTSH) (Thyrogen; Genzyme Corp.) or endogenously by thyroid hormone withdrawal (THW). Because the latter induces morbidity associated with severe hypothyroidism and may stimulate tumor growth, pretherapeutic scanning, aiming to predict uptake on 131I WBS (and potential therapy efficacy), is preferably done after rhTSH stimulation. However, it is unclear whether and to which extent patient preparation with rhTSH rather than THW affects the diagnostic accuracy of 124I PET/CT.
The clinical research question of this study was to determine whether futile 131I treatment could be prevented by pretherapeutic imaging with 124I PET/CT in patients with biochemical suspicion of recurrence without clinical evidence of locoregional metastases. Furthermore, we aimed to investigate the effect of the thyroid-stimulating hormone (TSH) method on diagnostic performance of 124I PET/CT in this clinical setting.
MATERIALS AND METHODS
Study Design
The THYROPET study was designed as a prospective nationwide multicenter diagnostic cohort study (Clinicaltrials.gov identifier: NCT01641679) (22). The study was approved by the institutional review board of The Netherlands Cancer Institute and by the local institutional review boards of the 17 participating centers. This study was investigator-initiated and conducted in accordance with the principles of the Declaration of Helsinki and good clinical practice guidelines. All participants provided written informed consent.
Patients
Adult patients with biochemical suspicion of recurrence of previously treated DTC (serum Tg > 2 ng/mL), without evidence of locoregional recurrence (negative ultrasound of the neck), who were planned for blind treatment with high-dose 131I were eligible for inclusion (Table 1). Main exclusion criteria were recent 131I therapy (<12 mo before inclusion) and any indication for another treatment modality (e.g., surgery).
Inclusion and Exclusion Criteria of THYROPET Study
Procedures
Pretherapeutic Phase
Patients received rhTSH (0.9 mg) intramuscularly on 2 consecutive days, 1 d after the second rhTSH administration; 74 MBq of 124I were administered intravenously, followed by 124I PET/CT 24 and 96 h later.
Therapeutic Phase
Patients were requested to keep a 1-wk low-iodine diet before 131I therapy. When TSH was 25 mIU/L or more or after at least 4 wk of THW, patients were admitted for 131I therapy (5.5 or 7.4 GBq). In centers in which local radiation safety regulations allowed such, patients underwent repeated 124I PET/CT during 131I treatment: a second dose of 124I was intravenously injected directly after the administration of 131I, and PET/CT was performed after 24 and 96 h. One week after 131I, all patients underwent posttherapy WBS or SPECT/CT. In addition (data not presented here), all patients underwent 18F-FDG PET/CT in the pretherapeutic phase and 18F-FDG and 124I PET/CT 6 mo after therapy (22).
Image Acquisition
PET/CT scanners of participating centers were calibrated for 124I to ensure adequate image quality (23). All 124I PET/CT scans were obtained according to the scan protocol associated to this study, which included an administered dose of 74 MBq and optimized settings for 124I. Scan trajectories (PET and WBS) covered perineum-skull vertex, for a scan time of 30 min. A standard energy window was applied for all PET acquisitions. European Association of Nuclear Medicine Research Ltd. reconstruction parameters were used (24). If available, time-of-flight acquisition and reconstruction were performed. WBS was performed as planar scintigraphy, combined with SPECT/CT according to standard local procedures.
Image Interpretation
An expert panel of 3 independent experienced nuclear medicine physicians reviewed all PET/CT scans, blinded to the 131I WBS results. The posttherapy 131I WBS were assessed separately by 2 other experienced nuclear medicine physicians. All scans were scored as malignant, equivocal, or nonsuspicious. Any disagreement between reviewers was discussed to reach consensus. If a scan was scored as equivocal it was considered malignant in the analysis to obtain maximal sensitivity.
Quantitative analysis of 124I PET/CT was performed using manually drawn volumes of interest, measuring the total activity (kBq) within the lesion, corrected with the calibration factor determined for that scanner at calibration (23).
Outcomes
The primary endpoint of this study was the accuracy of 124I PET/CT to predict, at a patient level, the posttherapy 131I WBS test result, as an operationalization of the impact of the implementation of 124I PET/CT as a scouting procedure to set the indication for 131I therapy. The secondary endpoint was a quantitative and visual comparison between 124I PET/CT performed after rhTSH stimulation (rhTSH-124I PET/CT) and after thyroid hormone withdrawal combined with low-iodine diet (THW-124I PET/CT).
Statistical Methods
The study was designed to define the accuracy of 124I PET/CT to predict the result of post-high-dose 131I WBS. The power calculation was based on the (conservative) assumption of 40% futile blind 131I treatments (6,7). With a sample size of 100 evaluable patients, a 2-sided 95.0% confidence interval (CI) for a single proportion using the Pearson–Clopper method for constructing the CI (exact binomial CI) would extend 10% from the observed proportion for an expected proportion of 40%.
Because wrongfully withholding potentially curative treatment for these patients is unacceptable, we decided to preleminary terminate the study if 3 patients had 124I PET/CT scans that turned out false-negative (1-sided 95% CI upper limit, 12%). There was continuous monitoring of false-negative 124I PET/CTs by the local study coordinators, followed by central adjudication by the central expert panel.
Patient demographic data, tumor characteristics, and data derived from the scans are described in frequency tables. Accuracy measures such as sensitivity, specificity, positive predictive value, and negative predictive value were calculated using the per-patient result of 124I PET/CT and 131I WBS as index and reference test, respectively.
RESULTS
The study was open for inclusion from December 2012 to May 2014. In May 2014, a third false-negative 124I PET/CT (vs. 131I WBS) was reported to the study coordinators, and when this finding was confirmed at central review, the study was preliminarily terminated according to the predetermined stopping rule. Because safety was not compromised, study procedures were completed in all 19 patients included until then. All patients underwent rhTSH-124I PET/CT in the pretherapeutic phase, and 5 patients underwent additional THW-124I PET/CT in the therapeutic phase.
Of these 19 patients, 2 were excluded from the 124I PET/CT versus 131I WBS comparison. One patient was excluded because other imaging, performed due to clinical signs and symptoms, had shown numerous distant metastases, among which were vertebral metastases threatening the spinal cord. In agreement with an escape rule in the protocol (i.e., allowing the attending physician to withdraw a subject from the study for urgent medical reasons), it was decided to refrain from 131I therapy and to start immediate palliative radiotherapy on the spinal metastases. Another patient was excluded because the elevated Tg level at the time of inclusion was not reproduced at an additional assessment during the study before 131I therapy.
The baseline characteristics of the 17 evaluable patients are listed in Table 2. Nine patients had previously received more than 1 131I treatment, with a mean interval between last 131I treatment and inclusion of 5.6 y; the median serum Tg level at 131I therapy was 28 μg/L (interquartile range, 129).
Baseline Characteristics of Subjects at Time of Inclusion (n = 17)
Patient-based analysis showed that 9 of 17 posttherapy 131I scans were tumor-positive (53%; CI, 28%–77%). 124I PET/CT scans showed uptake compatible with tumor activity in 4 of 17 scans (Table 3). In these 4 patients with a positive 124I PET/CT finding, the posttherapy 131I WBS was concordant (patients 2, 3, 7, and 16). In the 8 patients with negative posttherapy 131I scans, 124I PET/CT scans were also negative. However, of the 13 124I PET/CT scans with no pathologic uptake, 5 were false-negative (Figs. 1 and 2). One 124I-positive lymph node was surgically removed before the 131I therapy (i.e., protocol violation); this lesion was not included in the analysis (patient 14). At a patient level, the sensitivity, specificity, negative predictive value, and positive predictive value of 124I PET/CT (vs. 131I WBS) were 44% (CI, 14%–79%), 100% (CI, 63%–100%), 62% (CI, 32%–86%), and 100% (CI, 40%–100%), respectively (Table 4).
Overview of Included Patients

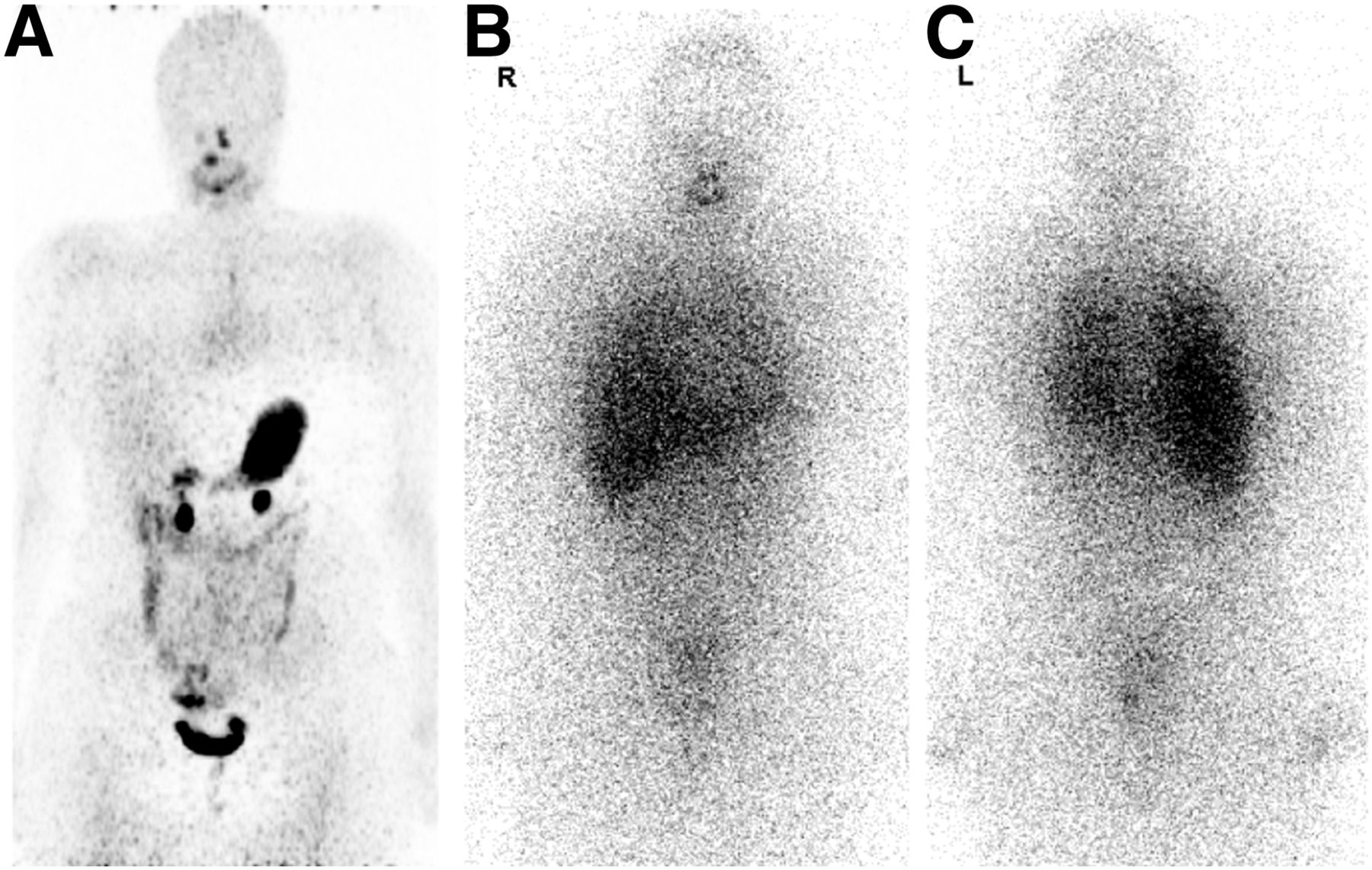
Patient 5 with negative 124I PET/CT (A) with disseminated lung metastases on 131I WBS (anterior [B] and posterior [C]).

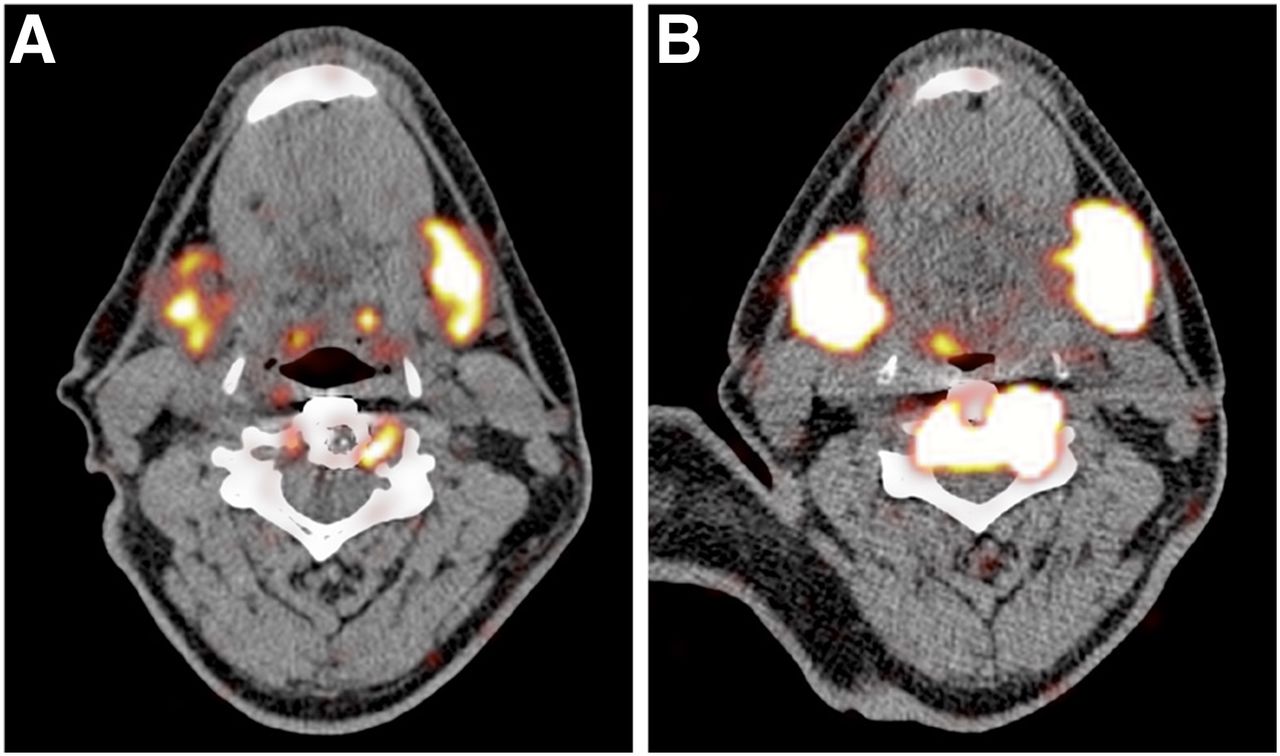
Patient 12 without pathologic uptake of 124I on PET/CT, only physiologic uptake in esophagus (A) and a positive 131I SPECT/CT finding, showing uptake in retroclavicular lymph node, which was confirmed as metastasis after surgical removal (B).
Patient-Based Analysis of Outcome of 124I PET/CT and 131I WBS
Lesion-based analysis showed that the posttherapy 131I WBS revealed 14 lesions versus 8 on 124I PET/CT (miliary lung metastases in patient 5 were counted as 1 lesion). The size of 3 of 7 lesions, false-negative at 124I PET/CT, could not be determined because no anatomic substrate was seen on CT (patients 5, 9, and 16). The other false-negative lesions measured 5, 5, and 7 mm (all lung lesions, patient 11) and 12 mm in diameter (retroclavicular lymph node, patient 12).
The 124I PET/CT scans after 24 and 96 h were on the patient level concordant in all but 2 patients (patients 3 and 14). In those patients, the lesions could not be depicted above the background noise after 96 h. No additional lesions were seen after 96 h.
Five patients underwent 124I PET/CT after rhTSH stimulation as well as THW during 131I therapy. No additional lesions were seen on THW-124I PET/CT in comparison to the rhTSH-124I PET/CT. Two of these patients (patients 2 and 3) showed pathologic 124I uptake on either scan. Patient 2 showed enhanced uptake (residual disease) around an orthopedic cage placed in vertebra C4 after resection of a DTC metastasis (Fig. 3). At 24 h after 124I administration, lesional tracer uptake was 13 kBq after rhTSH stimulation (0.02% of injected dose 124I) versus 332 kBq after THW (0.56% of injected dose 124I).
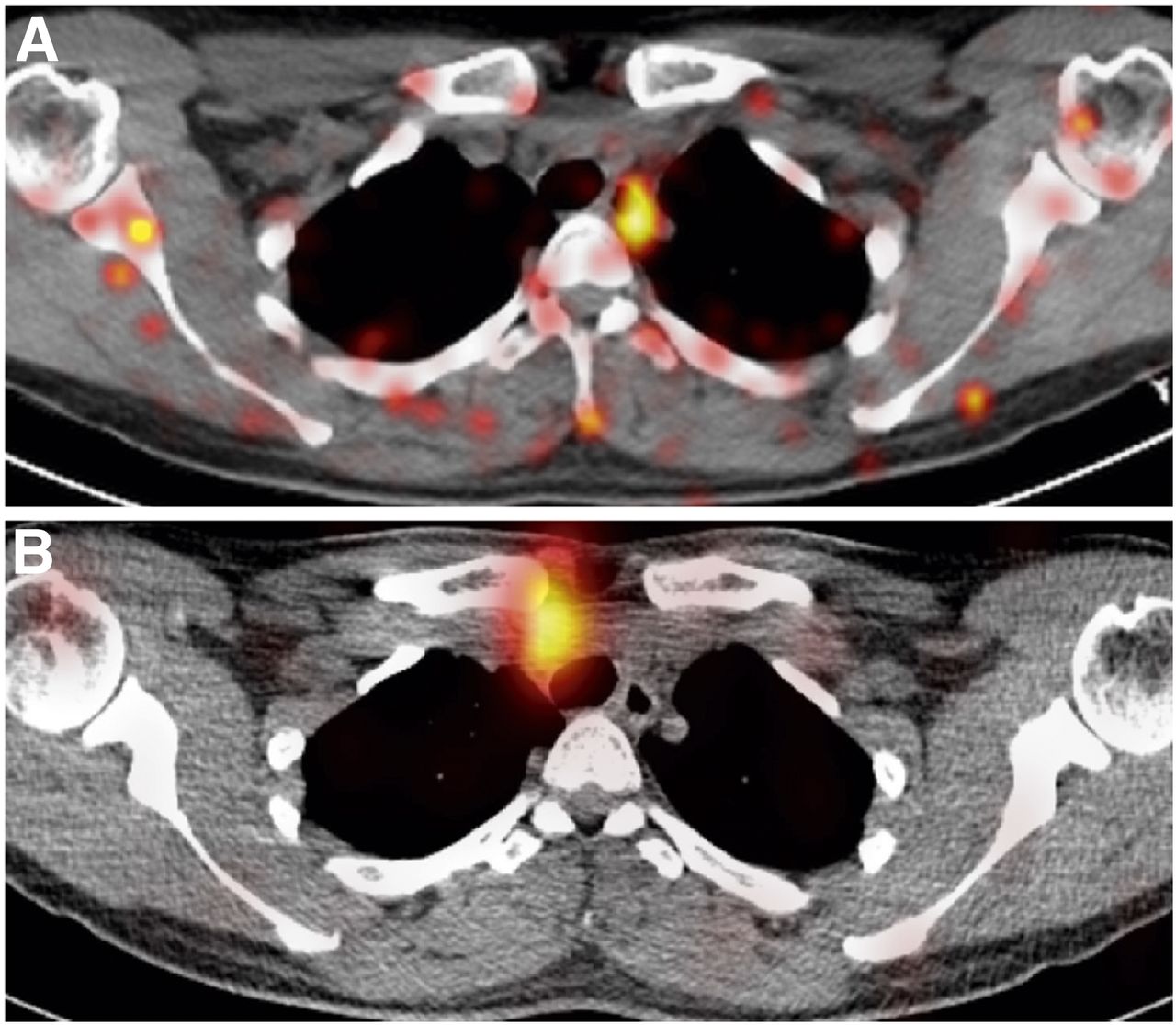
124I PET/CT of patient 2 with increased uptake of 124I in metastatic lesion in C4 after THW (B) compared with rhTSH (A).
The positive lesion in patient 3 was located in the mediastinum and was thought to represent a lymph node metastasis (corresponding with a 3- to 4-mm node at CT). 18F-FDG PET/CT had identified another suggestive mediastinal lymph node, negative on either iodine scan. At subsequent resection of this focus, the iodine-positive lesion was also removed. Histopathology revealed thymic tissue. 124I uptake in this lesion was below 2 kBq, both after THW and after rhTSH, precluding reliable quantification.
DISCUSSION
Our results demonstrated that rhTSH-stimulated 124I PET/CT as applied in this study was not suited to avoid futile blind 131I therapy, because of its high false-negativity rate (38%; 5/13). If 124I PET/CT results would have been used to guide therapy, potentially beneficial 131I therapy would have been withheld in 5 of 17 (29%). To our knowledge, this is the first prospective study performing a head-to-head comparison of pretherapeutic 124I PET/CT with posttherapy 131I WBS in a well-defined cohort of patients planned for blind 131I therapy. The high rate of futile therapies in our study, 47% (8/17), is consistent with published data, corroborating the need for better pretherapeutic diagnostic modalities (6,7).
Several publications described comparisons of 124I PET/CT and 131I WBS in thyroid cancer patients, but the results are inconsistent and difficult to compare with the results of the current study, because of variable clinical settings, study aims and inclusion criteria (8,19,25–29), methodologic design (28,30), different 131I dosages (8,29), diagnostic 131I WBS (27,28), and nonstandardized or variable patient preparation methods (8,25,27,28,30). Of these studies, the recent study by Khorjekar et al. is of interest because it specifically describes a cohort of 12 patients with suggestion of metastatic DTC, selected from different databases, in which a negative 124I PET/CT finding was followed by a posttherapeutic 131I WBS (30). In 10 patients, the 131I WBS revealed pathologic uptake. Another study of interest reported that, similarly to patient 5 in our cohort (Fig. 1), 124I PET can be false-negative in the case of disseminated lung metastases (31).
Biologic as well as technical issues may have caused 124I PET/CT scans to be false-negative. First, the method of TSH stimulation by rhTSH, instead of by THW in combination with a low-iodine diet, might have compromised the sensitivity of 124I PET/CT. This hypothesis seems to be supported by the observation in patient 2, in whom after THW and a low-iodine diet the 124I uptake was 23 times higher than after rhTSH stimulation (Fig. 3). Quantification of 124I might be affected by concurrent presence of 131I. However, a recently published phantom study showed that 131I did not affect the accuracy of 124I quantification (32). One other study has reported that significantly more foci were detected on both 124I PET and 131I WBS after THW stimulation in comparison to rhTSH stimulation (28). However, in that study interpatient comparisons were used rather than the head-to-head comparison in our study. Only a few cases with intrapatient comparisons of imaging after both THW and rhTSH have been described in previous studies. Freudenberg et al. described 1 case in which both an adrenal and a lymph node metastasis were seen only on 124I PET/CT after THW and not after rhTSH stimulation (33). Another study described 4 cases with 10 metastatic DTC lesions showing a 9%–62% higher iodine uptake after THW than rhTSH stimulation (34). Additionally, a dosimetric analysis of 3 patients with 22 metastatic lesions revealed an increased absorbed dose after THW in comparison to rhTSH in all but 2 lesions (35). Considering these results from previous studies and our findings, it might very well be that rhTSH patient preparation for 124I PET/CT may lead to false-negative 124I PET/CT scans; however, future studies with head-to-head comparisons are warranted to confirm this.
Second, we can only speculate whether the 74-MBq 124I dosage in our study contributed to the observed false negativity. Even though this dosage is higher than in most published studies (23–64 MBq) (25,27,30,31,36–38), Ho et al. recently reported the use of 222 MBq of 124I in patients with metastatic DTC refractory to radioiodine (39). Additionally, it is unclear whether improved PET scan technology (scanner design (40) or 124I reconstruction protocols) will improve 124I PET performance to a clinically relevant extent in this context. If in vitro data support the notion that detectability significantly improves by such innovations or higher 124I dosages, the current study should be repeated.
In our opinion, a scouting procedure using 124I PET/CT still remains the most rational strategy to reduce futile 131I therapies, but optimization is clearly required.
CONCLUSION
In patients with biochemical recurrence of DTC and a negative ultrasound of the neck, 124I PET/CT after rhTSH stimulation before blind 131I therapy, as applied in this study, does correctly predict tumor-positive uptake on posttherapeutic 131I WBS. Because of the high false-negative rate of 124I PET/CT, 131I should not be omitted based on a negative 124I PET/CT.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. Research support was provided by the Dutch Cancer Society (NKI 2011-5024). BV Cyclotron VU (Amsterdam, the Netherlands) provided 124I as an unrestricted study grant. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We acknowledge all the efforts of the participating centers. Furthermore, we thank the members of the independent review committee (Sakar Abdul-Fatah, Marnix Lam, and Pieter Raijmakers). The other members of the THYROPET Study group are John M.H. de Klerk, Meander Medical Center Amersfoort; Harm van Tinteren, Netherlands Cancer Institute; Jan Paul de Boer, Netherlands Cancer Institute; Hans Morreau, Leiden University Medical Center; Marc C. Huisman, VU University Medical Center; Eef G.W.M. Lentjes, University Medical Center Utrecht; Thera P. Links, University Medical Center Groningen; Jan W.A. Smit, Radboudumc; Jules Lavalaye, St. Antonius Hospital Nieuwegein; Piet L. de Jager, Isala Clinics; Corneline J. Hoekstra, Medical Center Jeroen Bosch; Martin Gotthardt, Radboudumc; Vanessa J.R. Schelfhout, Rijnstate Hospital; Wieger I. de Bruin, Medisch Spectrum Twente; Ferida Sivro, OLVG; Judit A. Adam, Amsterdam Medical Center; Ha T.T. Phan, Medical Center Leeuwarden; Gerrit W. Sloof, Groene Hart Hospital; and Nils R.L. Wagenaar, ZGT.
Footnotes
Published online Nov. 25, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 13, 2015.
- Accepted for publication November 11, 2015.





{kind=link}
{kind=link}
{kind=link}