


Abstract
68Ga-DOTATATE PET/CT scanning is a widely accepted method for imaging of neuroendocrine tumors. This cross-sectional study was performed to review the first 8 y of patient data from a large 68Ga-DOTATATE PET/CT database in order to establish the impact of the modality on patient treatment and survival. Methods: Demographic data, clinical outcome, survival, and change in management after 68Ga-DOTATATE PET/CT were evaluated. Results: Between May 2005 and August 2013, 1,258 68Ga-DOTATATE PET/CT scans were obtained in 728 patients with confirmed or suspected neuroendocrine tumors. In most patients, the primary site was located in the midgut (26.4%). Analysis of NET grading in patients with known histopathologic data revealed that 35.7% had NET grade G1, 12.2% G2, and 8.7% G3. The most common indications for 68Ga-DOTATATE PET/CT were follow-up (24.4%) and initial tumor staging (23.4%). Of the 1,258 68Ga-DOTATATE PET/CT scans completed, 75.7% were positive and 24.3% negative; there were 14 false-positive and 29 false-negative scans. The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value were 97%, 95.1%, 96.6%, 98.5%, and 90.4%, respectively. In 40.9% of patients, the treatment plan was changed after the scans, owing mainly to new, unexpected findings. Statistically significant differences in survival were shown between patients with G1, G2, and G3 grade tumors (P < 0.0001) and also between patients with bone metastasis versus patients with soft-tissue metastasis (P < 0.0001). Conclusion: 68Ga-DOTATATE PET/CT scanning is safe and influences management in a large proportion of patients. Prognosis was dependent on tumor grade, and the presence of bone metastasis was associated with worse overall survival.
Neuroendocrine tumors (NETs) are characterized by the presence of somatostatin receptors (SSTRs) on the cell surface (1,2). Of the SSTR subtypes characterized to date, SSTR2 is the most frequently overexpressed (3). This feature of SSTR expression has been exploited for imaging with radiolabeled somatostatin analogs (4). Combined PET and CT, using 68Ga-labeled somatostatin analogs, is increasingly applied for the diagnosis of NETs (2). Previously, studies have evaluated the role of 68Ga-DOTATATE PET/CT in diagnosis, staging, and monitoring of treatment response and follow-up in patients with NETs (2–5). These reports all involved a small number of patients, and a large database analysis has been lacking.
Imaging with 68Ga-DOTATATE PET/CT was first used clinically at the Institute of Nuclear Medicine, University College London Hospitals (UCLH) in May 2005. The institute has served as a national referral center for imaging these patients and is open to all stakeholders in the National Health Service. A 68Ga-DOTATATE PET/CT patient database was initiated, collecting information about patients referred for imaging with this tracer. This cross-sectional study was performed to review the first 8 y of patient data from the database (to August 2013). Patient demographics, tumors’ histology, and indications for 68Ga-DOTATATE PET/CT and its influence on management decisions were evaluated. Survival data were analyzed, and the correlation with 68Ga-DOTATATE PET/CT results was also assessed.
MATERIALS AND METHODS
Patients/Study Design
68Ga-DOTATATE PET/CT records were reviewed for demographic data. The clinical indication for the scan, site of primary tumor, tumor histopathology, and imaging data were also reviewed. Finally, the clinical outcome, survival, and change in management after the scan were evaluated from the multidisciplinary team discussion and case notes. The study was approved by the institutional ethics committee (study no. 15N10051).
The tumor grade of patients was determined histopathologically using mitotic rates and the Ki-67 index according to the European Neuroendocrine Tumor Society and the World Health Organization (6). These grading systems classify NETs into 1 of 3 grades: G1 (Ki-67 ≤ 2%), G2 (Ki-67 = 3%–20%), and G3 (Ki-67 > 20%).
Information on any adverse effects linked to 68Ga-DOTATATE injection was sought on the UCLH central incident-reporting system.
Image Acquisition
Images were acquired 45–60 min after injection of about 250 MBq of 68Ga-DOTATATE. The mass quantity of DOTATATE peptide that the patients received was in the range of 10–40 μg. Radiolabeling was performed as mentioned previously (7). No prior preparation was required for tracer injection. Patients on long-acting analogs of somatostatin did not stop their treatment because the scan was usually obtained before the injection. Imaging was performed using dedicated PET/CT cameras (Discovery ST or Discovery VCT; GE Healthcare) combining a PET unit and a 16-slice (Discovery ST 16) or 64-slice (Discovery VCT 64) CT unit. The CT exposure factor for all examinations was 120 kVp, and mA modulation was used (smart, 30–300 mA; noise index, 20; rotation, 0.8 s; pitch, 1.75).
Whole-body imaging from the mid femur to the vertex was performed, with the patient supine. PET emission images were acquired for 4 min at each bed position. The 68Ga-DOTATATE PET acquisition was performed in 3 dimensions with a 9-slice overlap between consecutive bed positions. PET images were reconstructed using an ordered-subsets expectation maximization algorithm with 2 iterations and 21 subsets and with CT-based attenuation correction.
Image Review/Interpretation
The 68Ga-DOTATATE PET/CT studies were reviewed for areas of abnormally increased tracer uptake by a team of experienced nuclear medicine physicians/radiologists. For visual analysis, 68Ga-DOTATATE uptake was considered abnormal if it was located outside the normal anatomic structures or if the intensity of uptake was greater than background, that could not be identified as physiologic activity (7). A patient-based analysis of the imaging findings was performed. The scan was classified as positive when abnormal uptake was identified, as explained above, and negative when only physiologic distribution of the tracer was observed (7). The presence or absence of disease was confirmed by histopathologic examination or by follow-up with radiologic or nuclear medicine imaging methods.
68Ga-DOTATATE PET/CT scans were considered false-positive if they showed uptake in inflammatory sites and benign diseases, including physiologic variants. The scans were considered false-negative when lesions identified with other imaging modalities were negative on 68Ga-DOTATATE and histopathologically confirmed as NET.
Patient Pathway
Data from NET multidisciplinary team minutes, patient discharge summaries, and correspondence were reviewed to evaluate the influence of 68Ga-DOTATATE PET/CT scanning on the treatment plan. Patients were clinically and radiologically followed up for at least 12 mo; those lost to follow-up were also reported. In May 2015, we checked the survival status of patients through the electronic files of the referring institutions.
Statistical Analysis
SPSS software (version 22; IBM) was used for data analysis. Patient demographics, site of primary cancer, tumor grading, and frequency of positive and negative findings on the scans are given by descriptive statistics.
A Mann–Whitney U test was used to assess statistical differences in survival between patients with negative and patients with positive scans. A P value under 0.01 was taken to indicate significance, and statistical tests were 2-sided. Kaplan–Meier survival analysis was performed to assess overall survival after 68Ga-DOTATATE PET/CT scans, using time to death as the endpoint. Patients who were alive were censored at the date of last clinical contact. Further survival analysis was performed regarding the histologic grading of the tumors. To assess whether different scan findings relate to overall survival, the Kaplan–Meier product limit estimators were calculated and compared by log-rank tests. Specifically, it was tested whether soft-tissue and bone metastasis result in statistically significant differences in patient survival.
For patients who underwent more than 1 scan, we took into consideration the first scan.
RESULTS
Patient Demographics and Clinical Indication for 68Ga-DOTATATE PET/CT
Between May 25, 2005, and August 19, 2013, 1,258 68Ga-DOTATATE PET/CT scans were obtained in 728 patients with confirmed (after biopsy/surgery) or suspected (elevated levels of tumor markers, clinical or image-based suspicion) NETs. After injection of the 68Ga-DOTATATE doses, no severe adverse effects were reported by patients or their referring physicians.
The patients comprised 388 women (53.3%) and 340 men (46.7%), aged 15–86 y (median age, 57 y; mean age ± SD, 54 ± 16 y). In most patients, the primary NET was located in the midgut (192/728, 26.4%), whereas in a significant number the primary site remained unknown (160/728, 22%). The remaining sites of primary NET or sites of clinical suspicion are documented in Figure 1. The most common clinical indications are shown in Table 1.
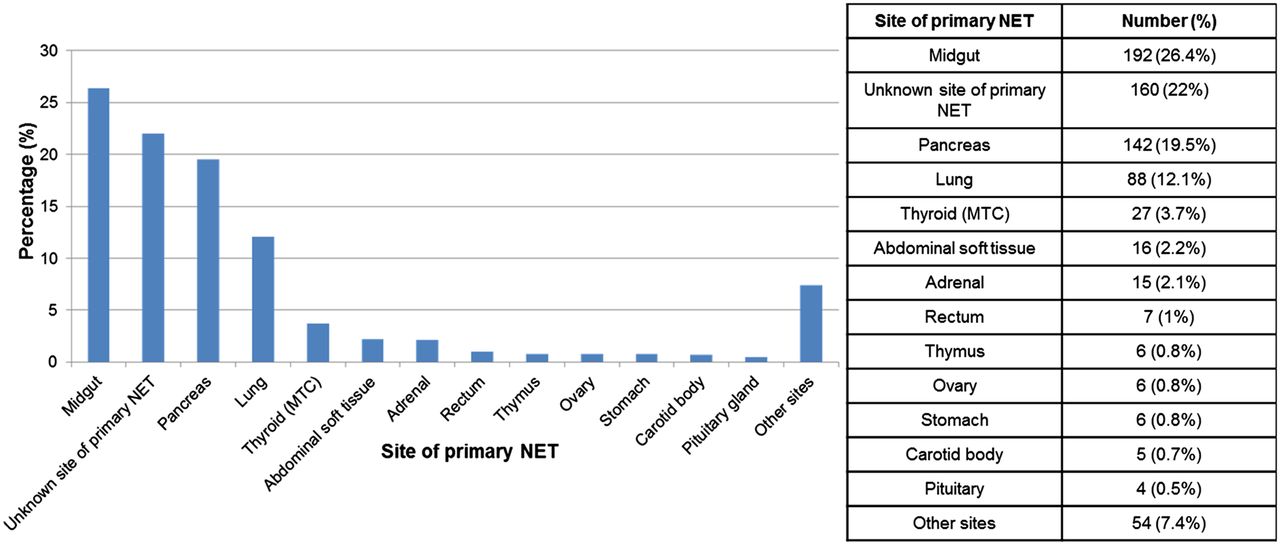
Site of primary NET or site of clinical suspicion in 728 patients at time of clinical referral. MTC = medullary thyroid cancer.
Indications for 68Ga-DOTATATE PET/CT Scanning
Tumor histologic data were available for 479 of the 728 patients (65.7%) who underwent 68Ga-DOTATATE PET/CT scanning. Of these, 260 had NET grade G1, 89 G2, and 63 G3. Of the remaining patients, 51 had proven neuroendocrine disease, mainly medullary thyroid cancer, neuroblastoma, and paraganglioma, but the histopathologic report had not used the grading system. In 16 patients, another malignancy (not neuroendocrine) was found. Eighty-nine of the patients (89/728, 12.2%) imaged because of clinical suspicion of NETs were proven, either histopathologically or at serial radiologic follow-up, to have no disease. For 160 of 728 patients (22%) with known previous NET or proven disease after the 68Ga-DOTATATE PET/CT scanning, histopathologic data were lacking.
68Ga-DOTATATE PET/CT Results and Impact on Patient Management
Most patients (490/728, 67.3%) had only 1 68Ga-DOTATATE PET/CT scan whereas 32.7% (238/728) underwent more than 1 scan, for reassessment after treatment, detection of suspected recurrence, or follow-up. The time interval between the 68Ga-DOTATATE PET/CT scans ranged from 1 to 77 mo (mean, 14.75 ± 12.75 mo).
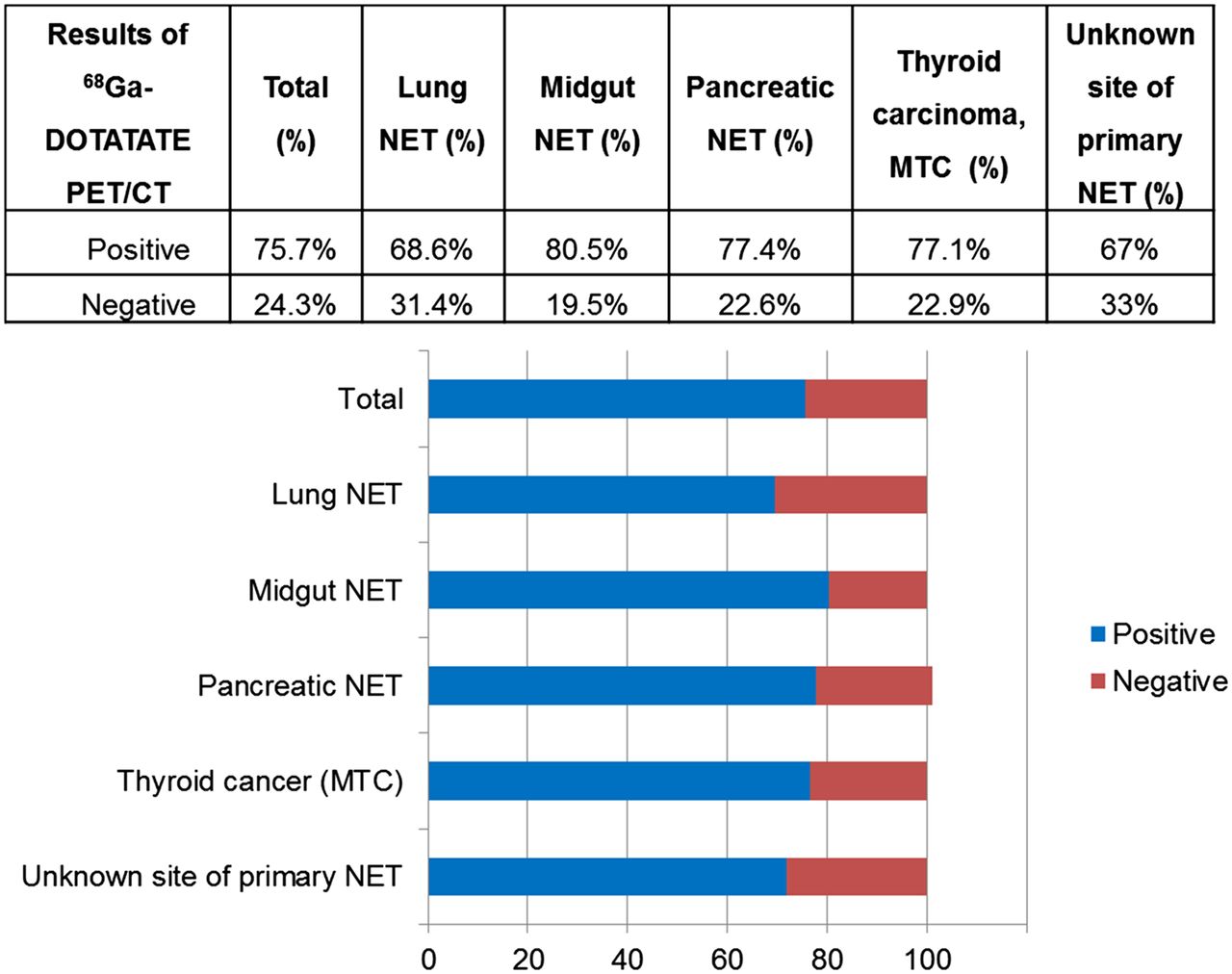
Of the 1,258 68Ga-DOTATATE PET/CT scans completed, 952 (75.7%) were positive and 306 (24.3%) negative. Positive scans were most frequently observed in midgut tumors (280/348 scans, 80.5%), whereas negative scans occurred most often in cases with an unknown site of primary NET (73/221, 33%) and in cases with lung NETs (37/118, 31.4%) (Fig. 2). Thirty-three of 37 of these lung NET patients were free of disease, and the remaining 4 had G2 lung carcinoid (atypical) with negative 68Ga-DOTATATE PET/CT scans. Of the 73 patients with unknown site of primary NET but suspected disease, 68 patients had no disease on any imaging modality; the remaining 5 had histopathologically proven NET (3 G3 and 2 G1).
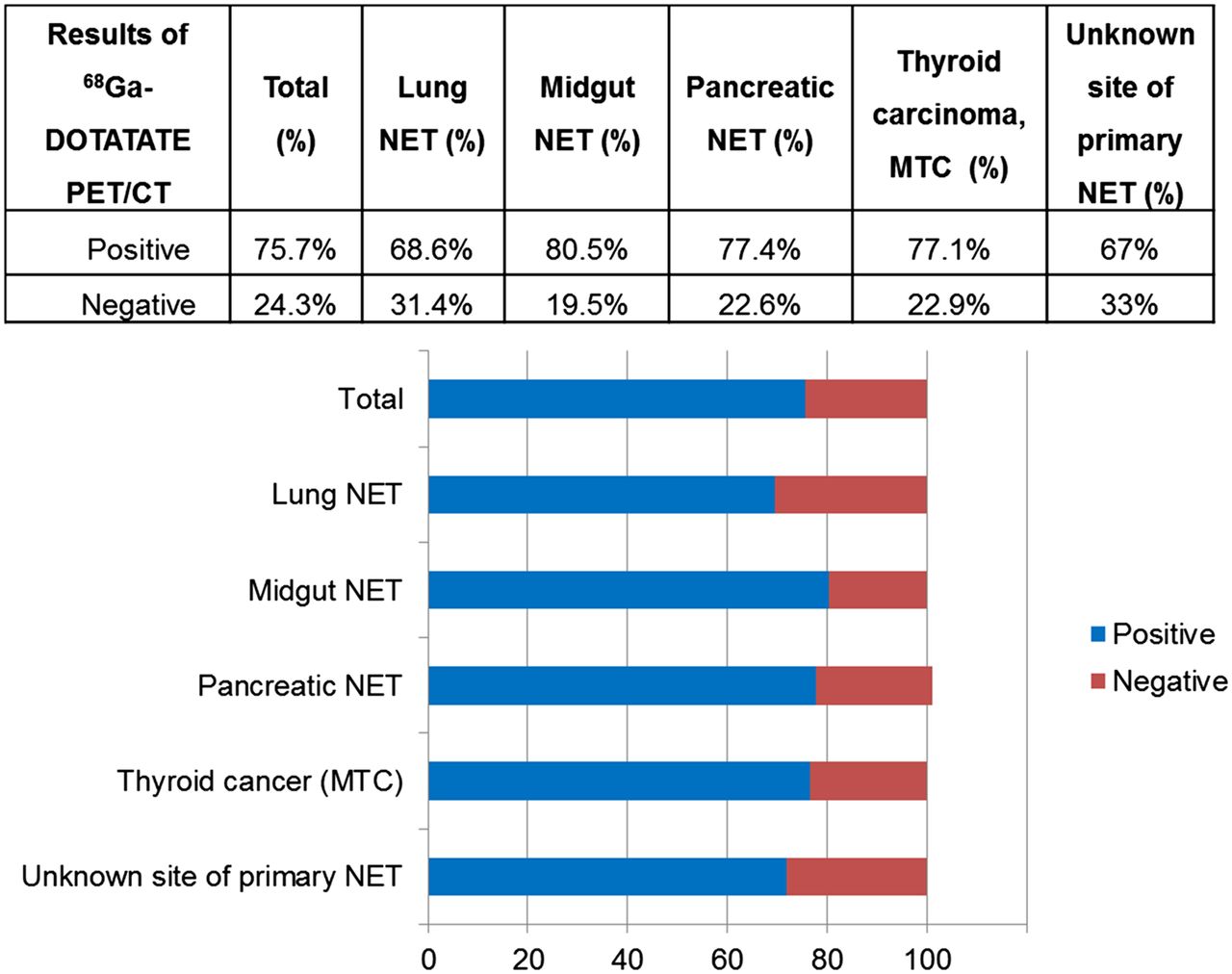
Results of 68Ga-DOTATATE PET/CT scans, overall and in most frequent NETs. MTC = medullary thyroid cancer.
The most common sites of 68Ga-DOTATATE uptake due to primary, recurrent, or metastatic disease are shown in Figure 3.

Findings in keeping with primary, recurrent, or metastatic lesions, in all positive 68Ga-DOTATATE PET/CT scans (percentage of all lesions).
When the results were analyzed, there were 941 true-positive, 274 true-negative, 14 false-positive, and 29 false-negative scans. With regard to the false-positive scans, in 5 cases there was 68Ga-DOTATATE uptake because of inflammatory changes; in 6 there was uptake in normal SSTR2-expressing organs, mainly the pancreas (4 in the pancreas, 1 in an adrenal gland and 1 in the small bowel); and in 3, there was uptake in other nonneuroendocrine neoplasms (2 benign, 1 malignant). In most of the false-negative cases, NETs found either histopathologically or using other imaging methods were of high or intermediate grade whereas in 1 case the false-negative result was due to a duodenal carcinoid less than 1 cm in diameter. Nevertheless, in 8 cases (8/29, 27.6%) the NETs were of low grade, that is, G1. The sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of 68Ga-DOTATATE PET/CT were 97%, 95.1%, 96.6%, 98.5%, and 90.4%, respectively.
Among the most common sites of primary tumors, 68Ga-DOTATATE PET/CT had much higher sensitivity, specificity, PPV, and NPV for midgut NETs than lung or pancreatic NETs, or cases with unknown site of primary NET (Table 2).
Diagnostic Values of 68Ga-DOTATATE PET/CT Scanning for Different Primary NETs
The treatment plan was changed after 515 (40.9%) of the 1,258 68Ga-DOTATATE PET/CT scans because of new, unexpected findings, whereas it remained unchanged in 740 cases (58.8%). The final influence of the scan on management remained unknown in 3 patients (0.2%) from overseas. Management change was most frequently observed in patients with medullary thyroid cancer (50%) or lung NETs (45.8%) (Fig. 4).
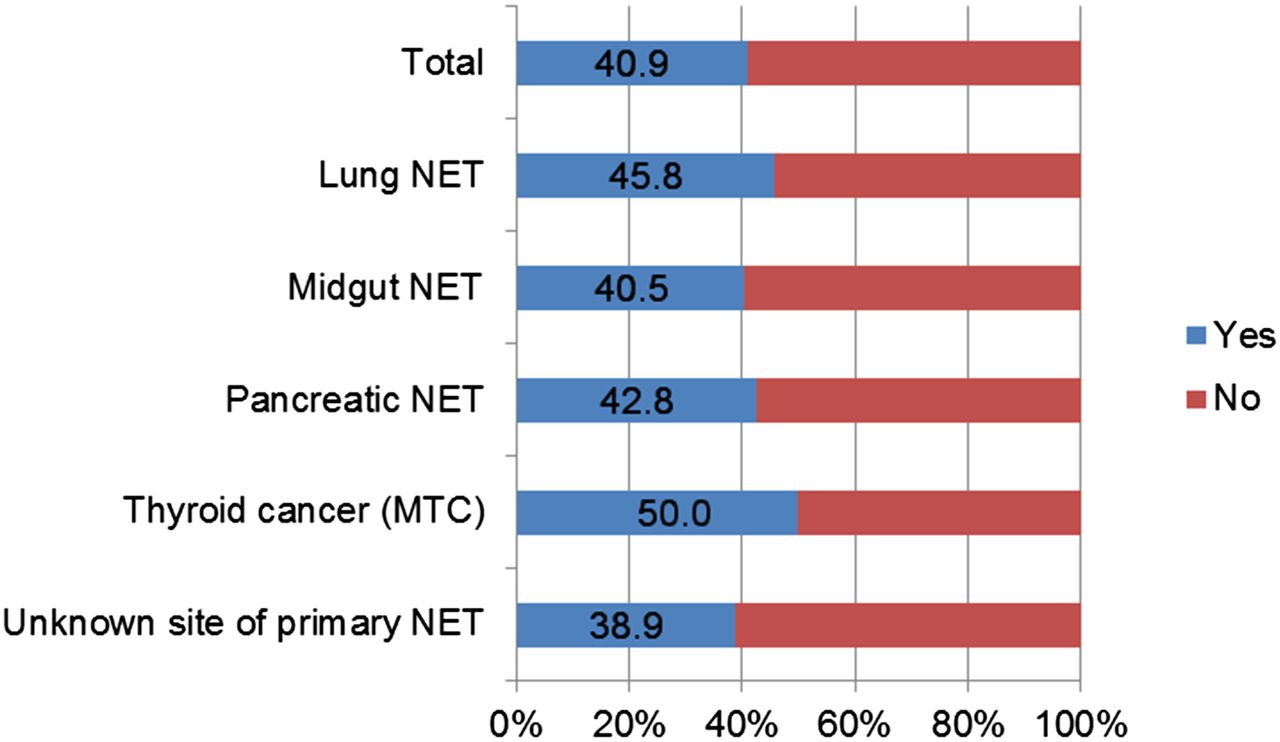
Change in therapy after 68Ga-DOTATATE PET/CT, overall (1,246 scans) and in most frequent NETs. MTC = medullary thyroid cancer.
Regarding the change in treatment plan, in most instances the new treatment comprised chemotherapy or peptide receptor radionuclide treatment (PRRT) (362/515, 70.3%). In 10.1% (52/515), resection of the primary NET was decided on, as 68Ga-DOTATATE PET/CT either localized an unknown site of primary NET (31 cases) or confirmed the suspected site (21 cases). Furthermore, in 13.8% (71/515), 68Ga-DOTATATE PET/CT showed progression of disease after the end of treatment administration, and another chemotherapy regimen was provided, whereas in 1% (5/515) a negative scan excluded a suspected NET. In the remaining patients, 68Ga-DOTATATE PET/CT results led to cessation of previous treatment (2/515) or rejection of PRRT (2/515) or revealed candidates for liver transplant (2/515), by excluding extrahepatic disease. In 19 patients the precise management change was unclear from the records.
Overall Survival Analysis
The median follow-up from the time of the 68Ga-DOTATATE PET/CT scan (or first scan if there was more than 1) was 38.4 mo (interquartile range, 53.2 mo).
Of the 728 patients, 206 had less than a year of follow-up, including 50 who died during the first year of follow-up. Of the remaining 522 patients with more than 12 mo of follow-up, 379 were followed up for more than 36 mo and 201 for more than 60 mo. Up to the present, 167 patients have died during follow-up. Most deceased patients had either an unknown site of primary NET (45 patients; 28.1% of all patients with unknown site of primary NET) or a primary NET located in the midgut (44 patients; 22.9% of all patients with midgut NETs).
Of the 167 patients who died, 137 had a positive and 30 a negative first 68Ga-DOTATATE PET/CT scan. Of these negative scans, 7 were false-negative (4 patients had G2 and 3 G3 NET), 5 patients were proven to have nonneuroendocrine malignancy, and 18 were truly free of NET disease.
Kaplan–Meier curves for postscan survival are shown in Figure 5. The mean survival for patients with true-negative scans was 100.5 mo (95% confidence interval [CI], 94–107 mo) versus 79.4 mo (95% CI, 75–84 mo) for those with true-positive scans (log rank, P = 0.000) (Table 3). For patients with true-positive 68Ga-DOTATATE PET/CT scans, overall survival after the scan was 89.6% at 1 y, 75.5% at 3 y, and 65% at 5 y, compared with 99.1%, 95% and 89%, respectively, for those with true-negative scans (Table 4).
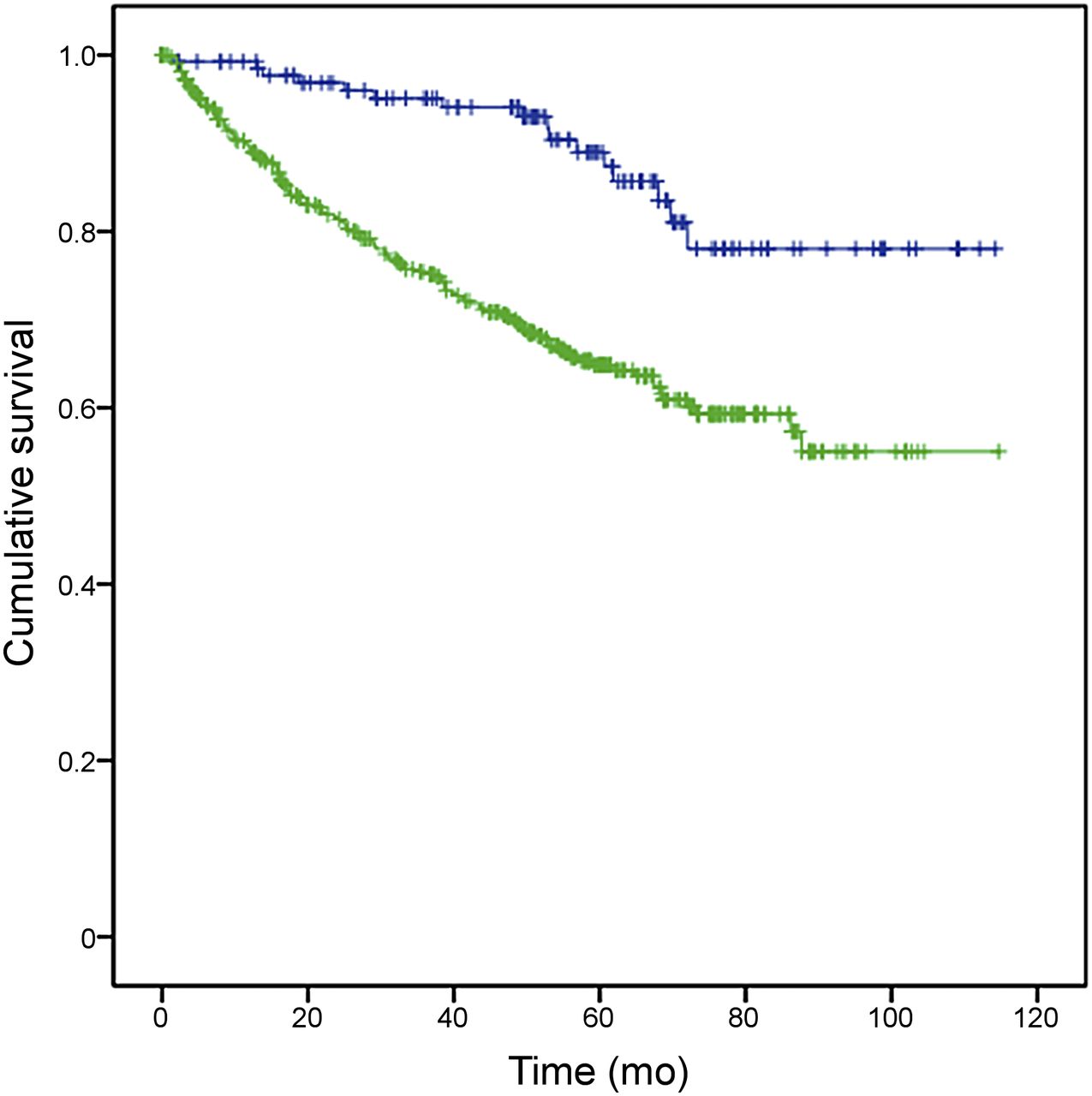
Kaplan–Meier curves for overall survival (in mo) of patients with true-positive (green) and true-negative (blue) 68Ga-DOTATATE PET/CT scans.
Mean Survival in Months for Patients after 68Ga-DOTATATE PET/CT Scanning
The 1-, 3-, and 5-Year Survival Rates After 68Ga-DOTATATE PET/CT Scanning
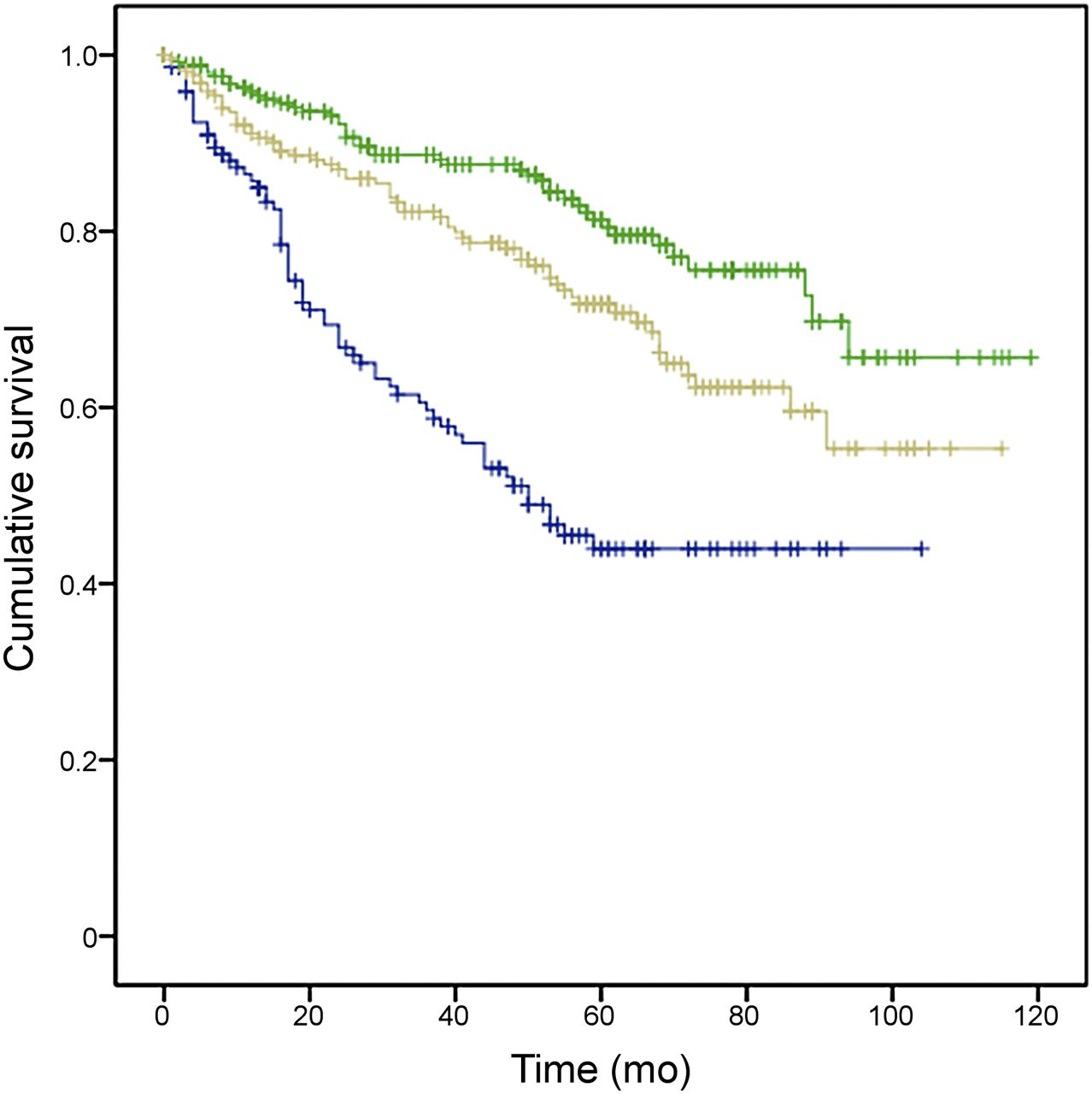
Further analysis of the survival data based on tumor grading revealed a statistically significant difference in survival between patients with G1, G2, and G3 grade tumors (P < 0.0001) (Fig.6; Table 5). This difference was maintained after dividing the cases into true-positive and true-negative scans (Table 6).

Kaplan–Meier curves for survival (in mo) of patients with histologic grade 1 (blue), grade 2 (green), and grade 3 (beige) NETs.
1-, 3-, and 5-Year Survival Rates After 68Ga-DOTATATE PET/CT Scanning for G1, G2, and G3 NETs and Results of Log-Rank Test for Difference in Mean Survival Regarding Grading
1-, 3-, and 5-Year Survival Rates After 68Ga-DOTATATE PET/CT Scanning for G1, G2, and G3 NETs in Patients with True-Positive and True-Negative Scans
Effect of Metastasis on Survival
68Ga-DOTATATE PET/CT identified soft-tissue metastasis (in the liver or lymph nodes) on the first scan of 368 patients (50.5%) and bone metastasis in 164 patients (22.5%); 127 patients (17.4%) were found to have both soft-tissue and bone metastasis.
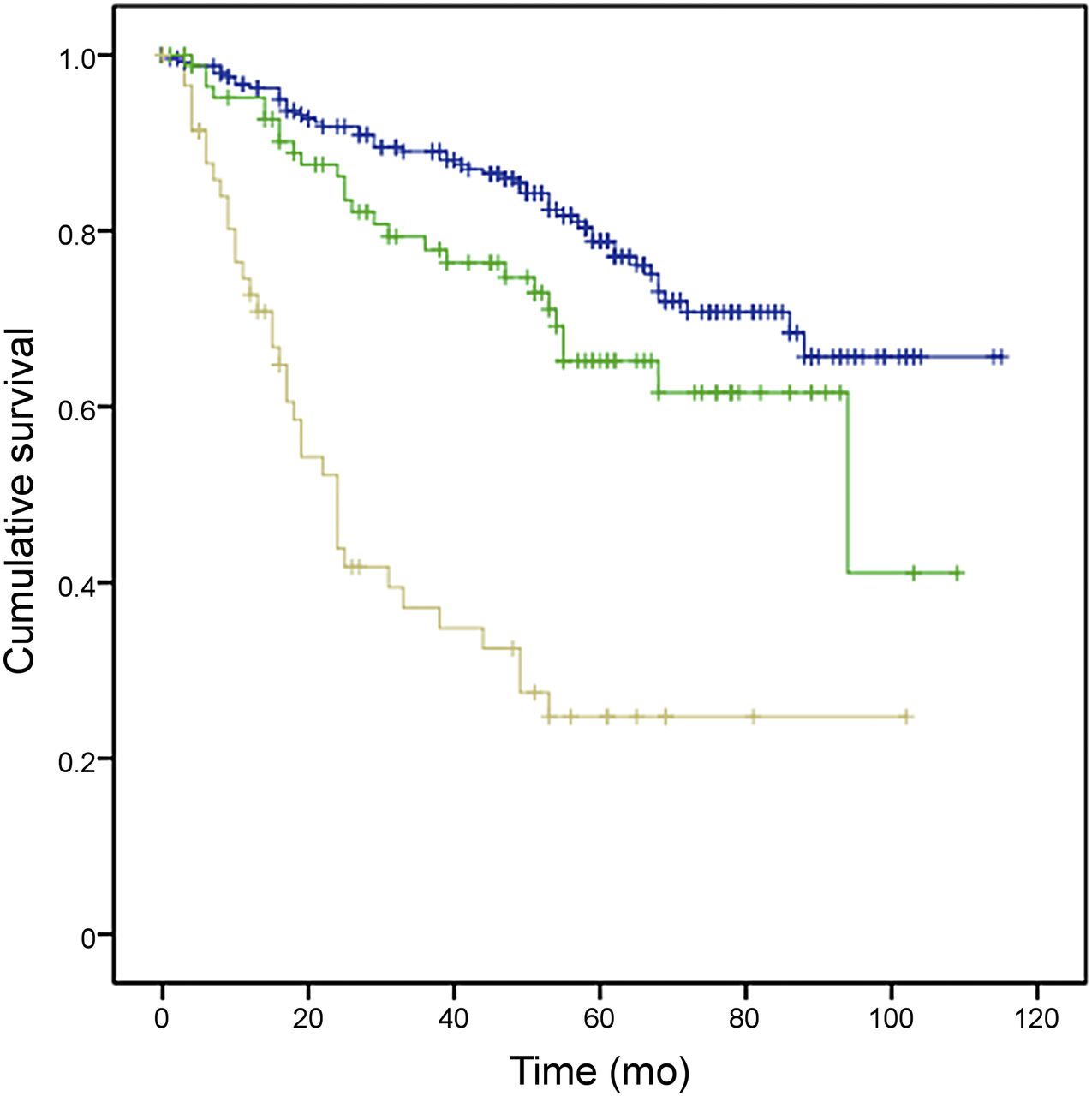
The effect of metastatic disease on patient survival was assessed using Kaplan–Meier analysis (Fig. 7). Mean survival after 68Ga-DOTATATE PET/CT for patients without metastatic disease was 96.7 mo (95% CI, 91–103 mo). For patients with soft-tissue metastasis, the median survival decreased to 84.1 mo (95% CI, 78–90 mo). There was a dramatic decrease in survival for patients with bone metastasis, with a median value of 59.6 mo (95% CI, 52–67 mo). This difference in overall survival between patients with bone metastasis versus patients with soft-tissue metastasis was found by the log-rank test to be statistically significant (P < 0.0001). Specifically, for patients without signs of metastasis on 68Ga-DOTATATE PET/CT, overall survival was 95.7%, 88.6%, and 81.3% at 1, 3, and 5 y, respectively, compared with 90.5%, 82.3%, and 71.7% for patients with soft-tissue metastasis and 85.6%, 60.5%, and 44.1% for patients with bone metastasis (Table 7).
Kaplan–Meier curves for overall survival (in mo) of patients with no metastatic disease (green), soft-tissue (liver and/or lymph node) metastasis (beige), or bone metastasis (blue) on their first 68Ga-DOTATATE PET/CT scan.
1-, 3-, and 5-Year Survival Rates in Patients with Soft-Tissue Metastasis, Bone Metastasis, or No Metastatic Disease on Their First 68Ga-DOTATATE PET/CT Scan
DISCUSSION
This study analyzed 1 of the largest cohorts of patients to be examined with 68Ga-DOTATATE PET/CT for imaging of confirmed or suspected NETs. Of the 728 patients, 388 (53.3%) were women. The median age of 57 y and the male–to–female patient ratio of about 0.9 were in agreement with previously published demographic data (8,9). In our study, the most common sites of the primary NET were the midgut (192, 26.4%), pancreas (142, 19.5%), and lung (88, 12.1%), whereas in 160 patients (22%) the primary site was unknown. In published epidemiologic studies, gastroenteropancreatic NETs have accounted for a higher proportion (54.5%–63%), whereas there have been fewer cases with unknown primary sites (4%–11%) (8,10,11). In our data, the observation of a high percentage of patients with unknown NET primary site was expected, given that 68Ga-DOTATATE PET/CT scanning was performed when conventional imaging yielded negative or equivocal results.
Several studies with small numbers of patients have confirmed the diagnostic role of 68Ga-DOTATATE PET/CT in identifying primary NETs and distant metastases (2). In 1 study, this modality detected 27% more lesions than previous conventional imaging, whereas in another, 68Ga-DOTATATE PET/CT findings resulted in stage modification in 28.6% of cases (2,12). For suspected NETs, the first published study to evaluate the role of 68Ga-DOTATATE PET/CT found it to be highly accurate and able to identify NETs with a sensitivity of 81% and to exclude them with a specificity of 90% (5). In addition, a recent study showed that 68Ga-DOTATATE PET/CT can detect NET recurrence and exclude its presence with quite high sensitivity (90%), specificity (82%), and accuracy (86%) (13).
In this study, the sensitivity, specificity, NPV, and PPV of 68Ga-DOTATATE PET/CT are much higher for midgut NETs (99.3%, 100%, 97.6%, and 100%, respectively) than for lung NETs (91.8%, 92.6%, 83.3%, and 96.6%, respectively) and are in accordance with published data (4,14). It is interesting that in the 14 cases with atypical lung carcinoid (G2), the sensitivity and NPV were much lower (63.6%, and 42.9%, respectively), whereas specificity and PPV were 100%. It is known that tumor uptake of 68Ga-DOTATATE is dependent on the tumor grading (2). Higher-grade NETs tend to have absent or low SSTR expression (11).
In our study, lymph nodes, liver, and bones were the most frequent sites of 68Ga-DOTATATE–avid metastatic lesions (25.3%, 23.8%, and 16.6%, respectively). Although NETs can metastasize to any organ, published surveys have shown that the liver is the most commonly involved organ when metastases occur (40%–93%), followed by bone (12%–20%) and lung (8%–10%) (3,15).
Analysis of our data revealed that 68Ga-DOTATATE PET/CT led to a change in the scheduled treatment plan in 40.9% of patients. Management change was most frequently observed in patients with medullary thyroid cancer (50%) and lung NETs (45.8%), whereas it was quite low in patients with unknown site of primary NET (38.9%). These results are in agreement with previous studies involving fewer patients (3,4,16,17). In 1 of those studies, 68Ga-DOTATATE PET/CT affected therapeutic management in 38% of patients (17) whereas in another it resulted in a change in clinical management in 70.6% (3). In another study in which management impact was classified as high (intermodality change), moderate (intramodality change), or low, the respective percentages were 47%, 10%, and 41% (2% of patients were not assessable) (16). A more recent prospective study evaluating the impact of 68Ga-DOTATATE PET/CT on management of NETs drew similar conclusions and showed that 68Ga-DOTATATE PET/CT affected the intended management in 60% of patients (18).
In our study, analysis of the survival data showed a statistically significant difference in survival between patients with G1, G2, and G3 grade NETs. These results are in accordance with previously published data regarding the prognostic value of the World Health Organization grading system in NET patients (19,20). Furthermore, regarding the correlation between the 68Ga-DOTATATE PET/CT results and patient survival, our study revealed statistically significant differences (P = 0.000) in 1-, 3-, and 5-y survival, as expected, between patients with true-negative and true-positive scans. There are small published reports regarding the prognostic value of the SUVmax on 68Ga-DOTA-peptide PET scanning in patients with NETs (21,22) and the change in tumor-to-spleen SUV ratio as an independent predictor of progression-free survival after PRRT (23). In our study, we did not attempt to correlate the SUV, as a semiquantitative marker of SSTR expression, with survival, as it is part of a separate study.
Bone metastases were once considered exceedingly rare in patients with NETs but more recent studies have shown that they may be detected in 12% of overall NET populations and approximately 25% in some subgroups (24). In the present study a significant difference in median survival was observed between patients with bone metastases and those with soft-tissue metastases (59.6 vs. 84.1 mo, P < 0.0001); median survival for those without metastatic disease was 96.7 mo. Our findings are in agreement with a recent study in which median survival for patients with both liver and bone metastases from NETs was 15.4–62.1 mo, compared with 18.2–166.3 mo in patients with liver metastases and no detected bone metastases (P < 0.0001), the variations depending on histologic subtype and grade of differentiation (24).
Finally, the fact that no severe adverse effects were reported after the injection of 1,258 doses of 68Ga-DOTATATE indicates 68Ga-DOTATATE PET/CT to be a safe procedure for patients.
Our study has several limitations. First, this was a retrospective study. To minimize potential associated errors relating to selection bias, information bias, and record-keeping, a unified database was defined early in the study. Second, differences in interpretation of findings between individual reviewers (all experienced) could not be accounted for. Furthermore, some patients were lost to follow-up, mainly due to the wide referral area. Finally, the patients received a wide variety of treatment regimens depending on the scan results, and this could not be controlled for in survival analysis.
CONCLUSION
Irrespective of the location of the primary, 68Ga-DOTATATE PET/CT findings affect management in a large proportion of patients with NETs, the most frequent change being a switch from surgery to chemotherapy or PRRT. Survival is predictable based on tumor grade. The presence of bone metastasis significantly shortens survival, compared with metastasis in the liver or lymph nodes (P < 0.0001).
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. The work presented was undertaken at UCLH/UCL, who received a proportion of funding from the Department of Health's NIHR Biomedical Research Centres funding scheme. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Rob Shortman for his help in gaining regulatory approvals required for commencement of this work.
Footnotes
Published online Oct. 15, 2015.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 24, 2015.
- Accepted for publication October 5, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A Self-Assembling and Disassembling (SADA) Bispecific Antibody (BsAb) Platform for Curative Two-step Pretargeted Radioimmunotherapy
- Evaluating the Role of Theranostics in Grade 3 Neuroendocrine Neoplasms
- Most of the Intended Management Changes After 68Ga-DOTATATE PET/CT Are Implemented
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- The Impact of Somatostatin Receptor-Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis
- Association between neuroendocrine tumors biomarkers and primary tumor site and disease type based on total 68Ga-DOTATATE-Avid tumor volume measurements
- MIB-1 Index-Stratified Assessment of Dual-Tracer PET/CT with 68Ga-DOTATATE and 18F-FDG and Multimodality Anatomic Imaging in Metastatic Neuroendocrine Tumors of Unknown Primary in a PRRT Workup Setting