


Abstract
High interstitial fluid pressure (IFP) in colorectal cancer metastases may decrease the uptake and, thus, the effects of antitumor drugs. Imatinib, a selective inhibitor of platelet-derived growth factor receptors, and anakinra, an interleukin-1 receptor antagonist, respectively, increase drug uptake or decrease IFP in preclinical models of carcinoma. Drug-induced decrease in IFP in human metastases has not been objectively shown but should be reflected by an increase in water-perfusable tissue fraction (PTF) or tumor blood flow (TBF) using 15O-water PET/CT and kinetic modeling. Hence, the aim of this study was to assess the effects of imatinib and anakinra on PTF and TBF in colorectal cancer metastases in patients. Methods: Nine patients with documented progressive disease despite all established therapy underwent 15O-water PET/CT at baseline and at 2 d and 6–7 d after the start of oral administration of imatinib (400 mg/d). After a washout period of 1 wk, the protocol was repeated with anakinra (100 mg/d) subcutaneously. Six patients underwent a second baseline scan on the same day to assess reproducibility of PTF and TBF measurements. Volumes of interest were drawn over liver metastases and aorta. PTF and TBF were calculated using the standard single-tissue-compartment model. Results: Imatinib administration during 6–7 d increased PTF from 0.62 ± 0.12 to 0.69 ± 0.13, compared with baseline and day 2 (P = 0.02, Wilcoxon test). No significant changes were found in TBF. PTF values were no longer significantly different from baseline 1 wk after the last imatinib dosage. Anakinra induced no significant change in PTF or TBF. The repeatability coefficients of PTF and TBF in liver lesions were 22% and 28%, respectively. Conclusion: Imatinib increases PTF of colorectal cancer metastases in patients and hence may increase the delivery of antitumor drugs. 15O-water PET/CT and kinetic modeling provide insights into the microenvironment of human cancers.
- interstitial fluid pressure
- metastatic colorectal cancer
- positron emission tomography
- water-perfusable tissue fraction
- tumor blood flow
High interstitial fluid pressure (IFP) in experimental solid tumors results in poor drug penetration and is, thus, a potential resistance factor for chemotherapy (1–3). Imatinib (Gleevec; Novartis), a selective tyrosine-kinase inhibitor, including that of platelet-derived growth factor receptor (PDGFR), is used in the treatment of gastrointestinal stromal tumors and chronic myeloid leukemia (4). It decreases tumor IFP and increases the efficacy of chemotherapy in animal cancer models (5–7). These effects of imatinib on experimental carcinoma are most likely mediated through an antagonistic effect on the PDGFR because a PDGF type B receptor–specific aptamer mimics the effects of imatinib (6). Similarly, interleukin-1 receptor (IL-1R) inhibition has reduced IFP in a cancer model, probably through effects on the tumor stroma (8). Anakinra (Kineret; SOBI), which is an IL-1R antagonist, is clinically approved for the treatment of rheumatic arthritis and thus possible to use in the clinic.
The concept of IFP-lowering by imatinib combined with chemotherapy has been tried in early noncomparative clinical trials but is difficult to evaluate because of the design of the trials (9,10). Whether the pharmacodynamic effect on tumor microenvironment from PDGFR or IL-1R inhibition is possible to achieve also in cancer patients has, to our knowledge, not been objectively documented. Repetitive direct measurements of IFP cannot be performed in patients because of the invasiveness of the procedure, and no validated noninvasive method exists.
PET with 15O-labeled water (15O-water) is the gold standard for the quantitative measurement of tumor blood flow (TBF) in units of milliliters of blood per minute per gram of perfused tissue. In addition, the kinetic model used for TBF measurements also calculates a parameter known as the water-perfusable tissue fraction (PTF) in units of gram of perfused tissue per milliliter of total tissue. Because of the complexity of the method, 15O-water PET has mainly been used as a reference tool in clinical research, with high accuracy and reproducibility (11,12). However, recent progress in image analysis provides accurate parametric images with high reproducibility, permitting more direct clinical use (13). We therefore chose to use 15O-water PET as a surrogate for IFP in the current study. Hypothetically, and based on preclinical findings (14), a reduction in IFP in response to treatment in clinical cancers is expected to increase PTF because of more homogeneous diffusion. Changes in IFP could potentially also cause changes in TBF.
The aim of the present pilot clinical study was, therefore, to assess the effect of imatinib and anakinra on PTF, as an index of fluid penetrance, and TBF in colorectal cancer metastases. These metastases are often visualized radiologically with a poorly perfused core associated with elevated IFP. The study was performed to establish a basis for further studies investigating the efficacy and safety of the combination of anticancer drugs with a drug that lowers IFP.
MATERIALS AND METHODS
Patients included in the study had metastatic colorectal cancer with at least 1 metastasis greater than 3 cm according to diagnostic CT in the liver or lung; progressive disease despite all established therapy and no experimental treatment or clinical trial protocol available; no on-going anticancer therapy and at least 4 wk since last therapy; essentially normal bone marrow, liver, and kidney function; and a World Health Organization performance status of 1 or less. Nine patients with metastases in the liver (n = 6) or lung fulfilled these criteria and were included. The study was performed in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board at the Department of Oncology. All patients received oral and written study information and provided written informed consent. For logistic reasons or drug adverse effects, all patients did not complete the entire protocol (see below). If an indication of a substantially lowered IFP was to be observed in an individual patient, the plan was to treat that patient with the IFP-lowering drug combined with the cytotoxic drug considered optimal in light of previous therapy.
Drug Administration
The day after the baseline PET scan, patients started imatinib (400 mg) orally once daily in the morning for a total of 6 or 7 d, adjusted to allow for the measurements as detailed below. After a minimum 1-wk washout, patients started anakinra (100 mg) subcutaneously in the morning for a total of 6 or 7 d. Imatinib and anakinra were used at the doses approved for the treatment of gastrointestinal stromal tumors and rheumatoid arthritis, respectively, as these doses have biologic effects yet are reasonably well tolerated. Ideally, the order of administration of the 2 drugs should have been balanced. However, the low number of patients in the study would not allow a direct comparison and because imatinib was expected to provide a rapid onset and stop of effect on IFP, all patients started with this drug.
Data Acquisition and Analysis
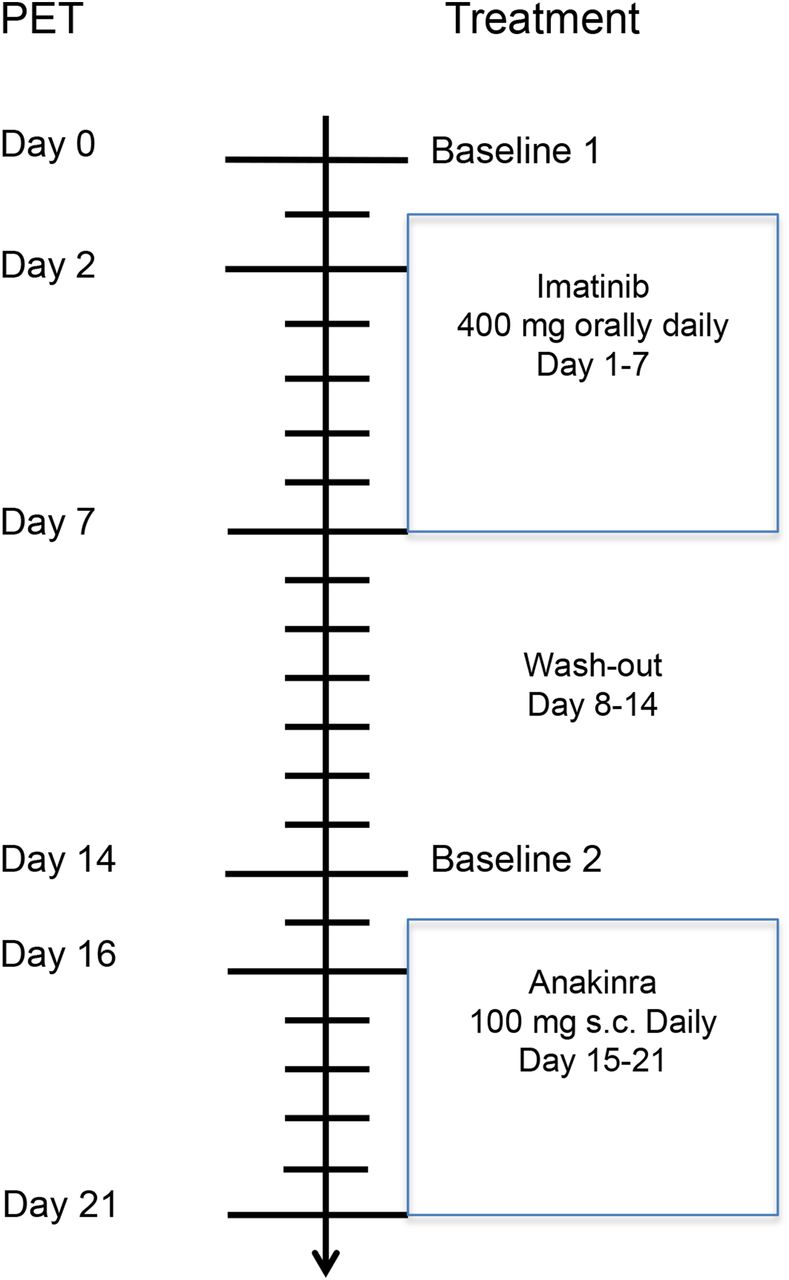
Each patient underwent 15O-water PET scans at baseline—that is, within 24 h before the start of either drug (n = 9) and after 2 (n = 8) and 6 or 7 d (n = 7) after the start of drug administration. Six of the patients also underwent an additional 15O-water scan on 1 of the study days to assess reproducibility of TBF and PTF measurements in liver lesions. Hence, up to seven 15O-water scans were obtained per patient. The protocol is outlined in Figure 1. Data were acquired on a Discovery ST PET/CT scanner (GE Healthcare) in 2-dimensional acquisition mode. After a low-dose CT scan to correct for attenuation, 1 GBq of 15O-water was administered simultaneously with the start of a 10-min dynamic PET scan (time-frame sequence: 1 × 10, 8 × 5, 4 × 10, 2 × 15, 3 × 20, 2 × 30, and 6 × 60 s). Images were reconstructed using ordered-subsets expectation maximization (2 iterations, 21 subsets) with a 4.3-mm gaussian postprocessing filter, applying all appropriate corrections for normalization, dead time, random coincidences, scatter, and attenuation.
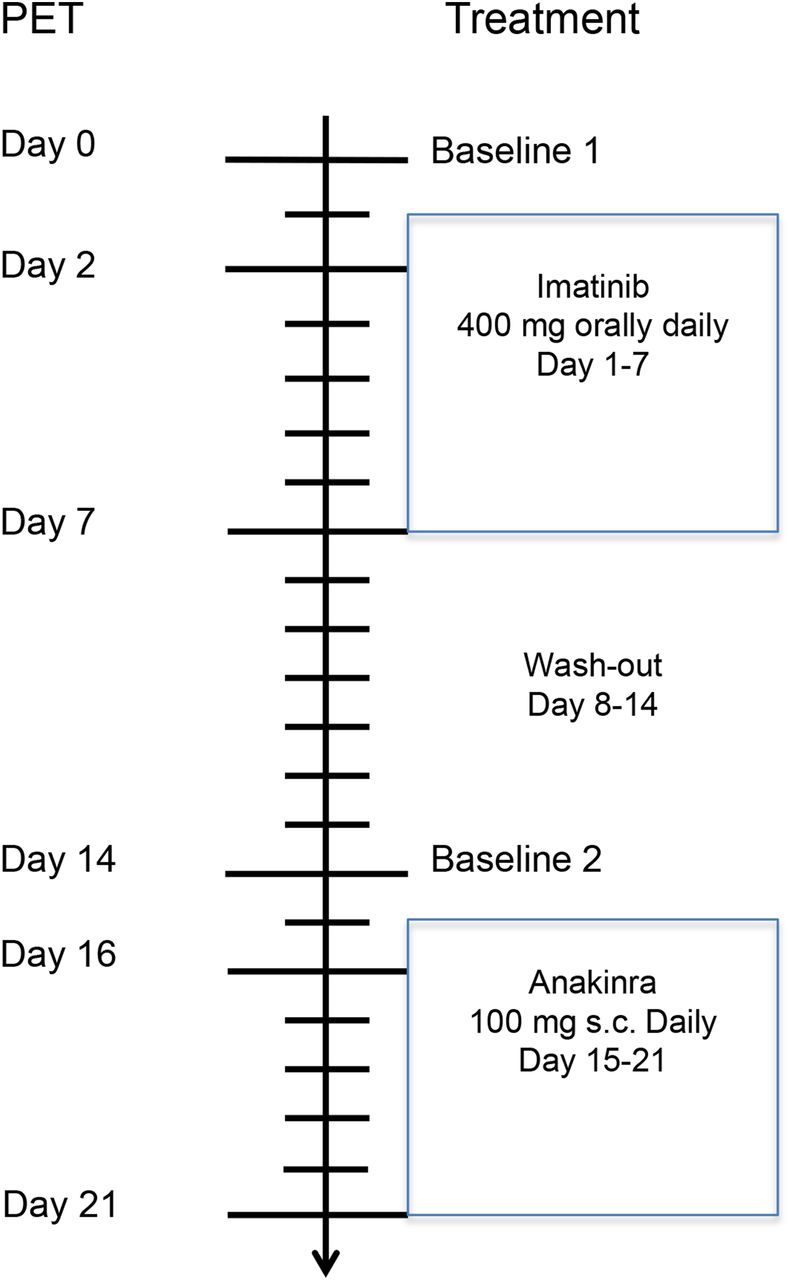
Outline of study design. Six patients were scanned twice at baseline 1 to assess repeatability of 15O-water PET measurements in liver metastases. s.c. = subcutaneously.
For definition of the arterial input function, 1-cm-diameter circular regions of interest were drawn over 10 consecutive planes over ascending (lung metastases) or descending (liver metastases) aorta and combined to a single volume of interest (VOI). Parametric TBF, PTF, and blood volume (VA) images were computed as described previously (13), assuming that liver metastases were perfused by branches of the hepatic artery. Lung lesion VOIs were drawn automatically at a 50% isocontour on parametric blood flow images using the NEDPAS software (VU University Medical Centre) (15). Liver metastasis VOIs were drawn manually at a 50% isocontour level on TBF images using a fusion PET/CT display in the Voiager software (GE Healthcare).
Liver metastases were first identified on the simultaneously acquired and fused CT scans. For each patient, parametric blood flow images at later time points were coregistered to baseline images using Vinci (Max Planck Institute), and VOIs were transferred to coregistered images. Then, all VOIs were transferred to the corresponding dynamic images, and TBF and PTF were calculated using nonlinear regression of the operational equation of the single-tissue-compartment model to the measured time–activity curves: Eq. 1Here, CPET(t) is the time–activity curve as measured by PET; CA(t) is the arterial time–activity curve; VA is a fractional arterial blood volume; F is blood flow; and VT is distribution volume, which was fixed at 0.96 mL cm−3. The fitted parameters were VA, k2 = F/VT, and K1 = PTF × F. Since VT was fixed, F was consequently directly determined from the clearance parameter k2, and PTF was then calculated as K1/F.
Eq. 1Here, CPET(t) is the time–activity curve as measured by PET; CA(t) is the arterial time–activity curve; VA is a fractional arterial blood volume; F is blood flow; and VT is distribution volume, which was fixed at 0.96 mL cm−3. The fitted parameters were VA, k2 = F/VT, and K1 = PTF × F. Since VT was fixed, F was consequently directly determined from the clearance parameter k2, and PTF was then calculated as K1/F.
Statistical Analysis
TBF and PTF values at different time points were compared using Wilcoxon matched-pairs signed-ranks tests. Repeatability coefficients for TBF and PTF in liver lesions were calculated as 1.96 times the SD of the differences between test and retest scans.
RESULTS
Nine patients participated in the study (5 men and 4 women with a mean age of 54 y). Patient characteristics are presented in Table 1. No serious adverse events related to the administration of imatinib and anakinra or to the PET assessments were observed, but 1 patient stopped imatinib after 3 d because of nausea and vomiting and 1 patient was excluded because of logistic reasons (cyclotron failure). No other dose adjustments of study drug doses were done. PET assessments are shown in Table 1. Eleven metastases could be clearly identified and were suitable for measurements, of which 7 were in the liver.
Patient Characteristics
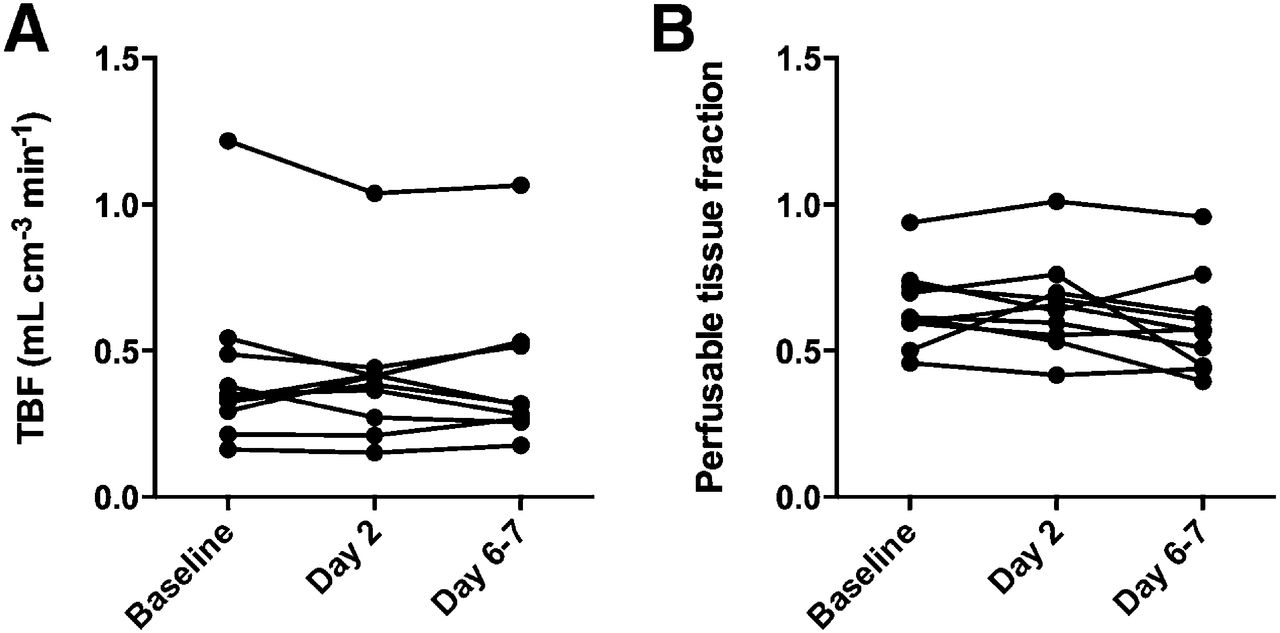
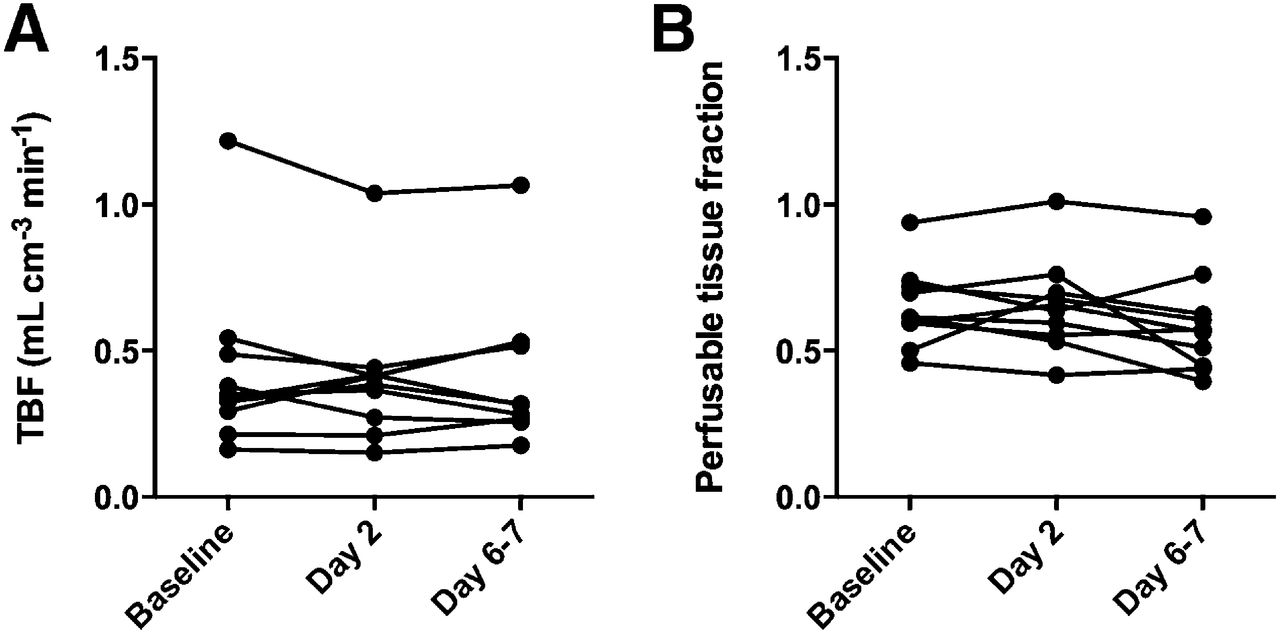
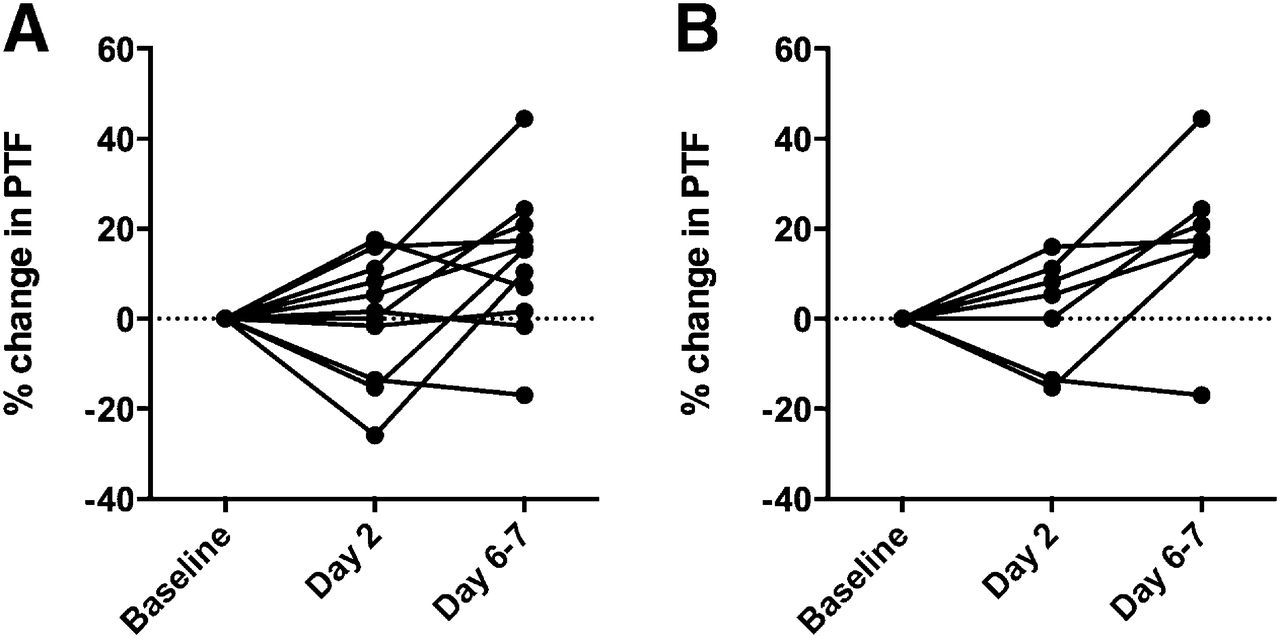
Figure 2 shows parametric TBF and PTF images of a patient with liver metastases. Figures 3 and 4 show TBF and PTF values for all metastases for imatinib and anakinra, respectively. Individual data are given in Supplemental Table 1 (supplemental materials are available at http://jnm.snmjournals.org). After 7 d of imatinib, PTF of liver lesions increased from 0.61 ± 0.15 to 0.71 ± 0.17 (P = 0.02, Wilcoxon test), compared with baseline and similarly compared with day 2 as well as for all lesions (Table 2; Fig. 3). As shown in Figure 5, relative changes in PTF ranged between −20% and +40% between baseline and 7 d of imatinib treatment. No significant changes were observed in TBF during imatinib treatment. Anakinra administration during 6–7 d led to a small but nonsignificant decrease in TBF, whereas no changes in PTF were observed (Table 3; Fig. 4). Repeatability coefficients in liver lesions were 22% and 28% for PTF and TBF, respectively.

Parametric images of PTF (mL of perfused tissue/mL of total tissue; top) and TBF (mL of blood/mL of perfused tissue/min; bottom) before (left) and after 7 d of treatment with imatinib (400 mg) daily (right). Parametric images are constructed using voxelwise kinetic modeling of dynamic 15O-water PET data. PET images of liver are shown, fused with simultaneously acquired CT. Arrows indicate metastases. PTF in metastases is increased after treatment, whereas TBF is relatively unchanged.

Plots of changes in microcirculation in colorectal cancer metastases during 1 wk of treatment with imatinib, a selective inhibitor of PDGF receptors. (A) TBF (mL of blood/min/mL of tissue). (B) PTF (mL of perfused tissue/mL of total tissue). *P < 0.05.
Plots of changes in microcirculation in colorectal cancer metastases during 1 wk of treatment with anakinra, an antagonist of IL-1Rs. (A) TBF (mL of blood/min/mL of tissue). (B) PTF (mL of perfused tissue/mL of total tissue).
TBF and PTF Values for Imatinib

Changes in PTF (mL of perfused tissue/mL of total tissue) in colorectal cancer metastases during 1 wk of imatinib treatment. Values at day 2 and days 6–7 of treatment are normalized to baseline measurement. (A) All analyzed metastases. (B) Liver metastases.
TBF and PTF Values for Anakinra
The VA coefficient used to fit arterial blood volume was below 0.01 in all cases, with an absolute repeatability coefficient in liver metastases of 0.004, and the uncertainty in VA did not contribute to any relevant extent to uncertainty in measurements of PTF or TBF.
None of the patients was treated with an IFP-lowering drug combined with chemotherapy because at the time IFP data were obtained, patient performance status had deteriorated or there were signs of disease progression precluding a therapeutic intervention.
DISCUSSION
To the best of our knowledge, this is the first study to document that imatinib introduces significant changes in the metastatic microenvironment in cancer patients. These changes were shown as increased fluid penetrance in colorectal cancer metastases. Tumor blood flow, however, was not increased. IL-1R inhibition with anakinra, on the other hand, produced no similar effects on the tumor microenvironment. Seemingly, our findings support the coadministration of chemotherapy with imatinib as a way to improve the chemotherapy effect in patients with liver metastases of colorectal cancers.
In 2 lesions (liver metastases), the increase in PTF after 1 wk of treatment with imatinib was larger than 22%, which is the threshold for a significant effect within a single lesion (i.e., the increase for which there is a probability of >95% that the observed increase is a true increase in PTF). The repeatability coefficients of 22% for PTF and 28% for TBF can be compared with previously published values of 37% and 20%, respectively, for lung cancer using the same technique (13). If 15O-water and PET were to be used for selection of patients who are suitable for chemotherapy combined with imatinib, then a 22% increase in PTF relative to baseline could be used as a cutoff value for further treatment.
No effect on PTF or TBF after treatment with anakinra was observed in the present study (Table 3; Fig. 4). This finding suggests that inhibition of IL-1R does not change the hydrodynamic properties in the metastases. The lack of effect by anakinra could, however, be due to the experimental design in which anakinra was always given after a treatment cycle with imatinib, the 1-wk washout period between the drugs was too short, and that the imatinib effect somehow blocked a potential effect by anakinra. Because the baseline PTF and TBF values before the start of anakinra were essentially similar to those before the start of imatinib, this possibility seems less likely. It may also be that inhibition of IL-1R, compared with PDGFR, needs a longer time of exposure to produce an effect or that the dose of anakinra associated with treatment of rheumatoid arthritis and used here was too low. In fact, in previous preclinical experiments, a far higher dose, in the order of 100 times more, was needed to lower IFP (8).
TBF measurements integrate the metabolic needs of the tumor tissue and flow capacity of the vasculature. 15O-water, being 100% diffusible, specifically measures the nutritive perfusion through tissues. In metastases of colorectal cancer, the metabolic needs generally exceed flow capacity, resulting in hypoxic cores. In several tumor types, an inverse relationship between perfusion and glucose metabolic activity has been described (16). Still, treatments aiming at decreasing the IFP might unintentionally improve nutritive perfusion and reestablish viability and proliferation in near-necrotic parts of the tumor. The current results, however, indicate that short-term treatment with imatinib exerts an effect on the tumor microenvironment with minimal effect on the mean perfusion rate.
In this study, most metastases investigated were located in the liver. Physiologically the liver has dual blood supplies from the hepatic artery and the portal vein, but the compartmental model used to assess PTF and TBF with 15O-water accounts only for arterial blood. Generally, liver metastases receive their blood supply from the arterial side only (17), a phenomenon routinely used in diagnostic imaging using contrast-enhanced CT in which optimal scanning of liver metastases includes arterial-phase image acquisition. Similarly, embolization of liver metastases also uses the arterial route.
Technically, quantitative PET imaging requires dynamic imaging for several minutes with normal tidal breathing, during which the metastases move 2–3 cm. Therefore, TBF and PTF values are potentially affected by the kinetics of 15O-water in the normal liver tissues surrounding a metastasis and nurtured primarily by portal blood. To minimize the effect of this confounder, only metastases larger than 3 cm were analyzed and only central portions of the metastases were graphically included in the VOIs. Perfusion measurements using 15O-PET in liver tumors, including liver metastases of colorectal cancer, have been reported previously for small patient numbers, and the values for TBF in the current study are in the same range (18).
Further, to the best of our knowledge, the current study is the first attempt to apply PET technology for measuring the PTF in liver metastases. Methodologically, PTF describes the fraction of a given tissue volume in which fluid flux takes place. PTF was originally investigated as an indicator of scarring in chronic myocardial infarction (19,20) but has also been used to show reversible changes with high precision in interstitial myocardial fluid penetrance due to edema after revascularization in acute infarcts (21).
Measurements of PTF and TBF using 15O-water PET/CT rely on kinetic modeling. Considering the methodology, there are alternative conclusions available. Assuming a constant PTF instead of a constant intratumoral distribution volume of water (VT in Eq. 1), the volume of distribution of water was increased by imatinib. Because both the amplitude and the clearance rate of the exponential function include F, PTF and volume of distribution cannot be estimated simultaneously and either one of these parameters has to be assumed constant. However, because PTF and VT are essentially interchangeable in Equation 1, relative changes in VT can always be interpreted as identical relative changes in PTF.
This study has obvious limitations. It was a pilot feasibility study recruiting only a few patients, which lowers the statistical power. The study included only 4 lung metastases from 2 patients, too few for a separate statistical analysis of lung measurements to be relevant. We therefore cannot rule out that the effect of imatinib on tumoral fluid penetrance is unique to liver metastases. Thus, the observed findings are in need of corroboration. Furthermore, when it comes to a future clinical application of the findings—that is, the combination of chemotherapy with imatinib as an adjunct to provide therapeutic synergy—we do not know about the long-term effects of imatinib on the fluid penetrance (i.e., whether the effect would be attenuated with repeated cycles or continuous administration of imatinib).
We also do not know if the observed change in PTF provided by imatinib would correspond to a biologically significant increase in tumor uptake of chemotherapeutic drugs or whether such increase would kill considerably more tumor cells. A next step to address this issue would be PET studies with labeled drug to allow for measurements of tumor drug concentrations with and without imatinib.
CONCLUSION
Imatinib increases fluid penetrance or water-perfusable fraction of tumor tissue, but not tumor blood flow, and hence may increase delivery of antitumor drugs to colorectal cancer metastases in the liver.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Mimmi Lidholm, Annie Bjurebäck, Maj Wiberg, and Lars Lindsjö for scanning and technical support and Annika Lidén for taking care of the patients. Thanks also to Johan Lilja, MSc, for coding the Voiager software package used for region-of-interest analysis.
Footnotes
↵* Contributed equally to this work.
Published online Jun. 11, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 4, 2014.
- Accepted for publication May 28, 2015.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}