


Abstract
In this article, we describe an image analysis strategy with improved power for tracking longitudinal amyloid-β (Aβ) PET changes and evaluating Aβ-modifying treatments. Methods: Our aims were to compare the power of template-based cerebellar, pontine, and cerebral white matter reference regions to track 24-mo florbetapir standardized uptake value (SUV) ratio (SUVR) changes; to relate those changes to 24-mo clinical declines; and to evaluate Aβ-modifying treatments in Aβ-positive (Aβ+) and Aβ-negative (Aβ−) patients with probable Alzheimer dementia (pAD), in patients with mild cognitive impairment (MCI), in cognitively normal controls (NCs), and in cognitively normal apolipoprotein E4 (APOE4) carriers and noncarriers. We used baseline and follow-up (∼24 mo) florbetapir PET scans from 332 Aβ+ and Aβ− subjects participating in the multicenter Alzheimer’s Disease Neuroimaging Initiative. Each of the proposed analyses included 31 pAD patients, 187 MCI patients, and 114 NCs. Cerebral-to-white matter, cerebellar, and pontine SUVRs were characterized in terms of their longitudinal variability; their power to track longitudinal fibrillar Aβ increases in Aβ+ and Aβ− subgroups and cognitively normal APOE4 carriers and noncarriers; the sample sizes needed to detect attenuated accumulation of or clearance of fibrillar Aβ accumulation in randomized clinical trials; and their ability to relate 24-mo fibrillar Aβ increases to clinical declines. Results: As predicted, cerebral-to-white matter SUVR changes were significantly less variable and had significantly greater power to detect 24-mo fibrillar Aβ increases and evaluate Aβ-modifying treatment effects in Aβ+ pAD, MCI, and NC subjects and cognitively normal APOE4 carriers. They were also distinguished by the ability to detect significant associations between 24-mo Aβ increases and clinical declines. Conclusion: A cerebral white matter reference region may improve the power to track longitudinal fibrillar Aβ increases, to characterize their relationship to longitudinal clinical declines, and to evaluate Aβ-modifying treatments in randomized clinical trials.
PET ligands (1–15) have made it possible to investigate the fibrillar amyloid-β (Aβ) burden in living people; to clarify its relationship to the dementia, mild cognitive impairment (MCI), and preclinical stages of Alzheimer disease (AD); to characterize the extent to which cross-sectional measurements predict subsequent clinical declines; to track longitudinal changes; and to help evaluate Aβ-modifying treatments.
Researchers commonly compute a semiquantitative cerebral-to-reference region standardized uptake value ratio (SUVR) using PET counts from a cerebral region of interest (ROI) and from a whole cerebellar (2,3), cerebellar gray matter (10), or pontine (8) reference ROI that is thought to be relatively devoid of fibrillar Aβ. Less commonly, researchers compute a cerebral-to-reference region distribution volume ratio or other quantitative measures using longer, dynamically acquired PET scans and the same cerebral and reference ROIs. With conventional reference ROIs, several radioligands have demonstrated a close association between cross-sectional PET SUVR or distribution volume ratio measurements and subsequent postmortem histopathologic measurements of fibrillar Aβ burden and have been used to define relevant thresholds for distinguishing between individuals with and individuals without moderate to severe neuritic plaques (2,8,16,17).
Although longitudinal analyses have the potential to track the progression of fibrillar Aβ deposition over time, to relate this progression to progressive clinical decline, and to evaluate putative Aβ-modifying treatments in therapeutic trials, we and others (18–22) have noted substantial variability in longitudinal florbetapir PET measurements of changes in fibrillar Aβ deposition. Some of this variability appears to exceed that expected on the basis of biologic grounds alone (e.g., SUVR changes of >50%, in either direction, over a matter of weeks).
Among other possible causes, we wondered whether some of the variability in longitudinal Aβ PET measurements might be due to between-session differences in the level or angle of a person’s head in the PET scanner and its differential effects on measurements from the cerebral and more inferior cerebellar or pontine ROIs. For instance, if a person’s head is positioned a shorter distance into the scanner, then the cerebellum and pons are closer to the inferior limit of the field of view. The resulting reference ROI measurements could be noisier because the 3-dimensional reconstruction algorithm would depend on fewer coincidence events; they could also be preferentially affected by scattered radiation from the body or differentially affected by the way in which the data are reconstructed and corrected for attenuation and scatter. Thus, the use of cerebral and reference ROIs located approximately the same in the axial field of view to generate SUVRs could result in reduced variability in longitudinal SUVRs and improve the power to evaluate Aβ-modifying treatments in therapeutic trials. Although we have not yet attempted to clarify whether between-scan differences in scanner head positioning account for the variability in longitudinal florbetapir SUVRs, we were motivated to examine whether a cerebral white matter ROI could reduce the variability in longitudinal florbetapir SUVRs.
In this article, we describe the use of a cerebral white matter reference ROI to reduce the variability in longitudinal florbetapir SUVRs, to improve the sensitivity for detecting corresponding increases, and to improve the power for evaluating Aβ-modifying treatments—an approach that is also being evaluated by other groups (18–22). Although cross-sectional cerebral-to-cerebral white matter SUVRs could be affected by the combined effects of fibrillar Aβ and partial-volume averaging, we surmised that this confound could be at least partly reduced in the assessment of longitudinal data because between-session differences in white matter measurements (including those related to the combined effects of small gray matter Aβ PET changes and partial-volume averaging) would be relatively small.
In this study, baseline and 24-mo florbetapir PET data from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) were used to determine the extent to which the use of a cerebral white matter reference ROI could reduce longitudinal SUVR variability and improve the power to detect longitudinal increases in fibrillar Aβ; to relate longitudinal Aβ deposition and clinical progression; and to estimate the sample sizes needed for the evaluation of fibrillar Aβ-modifying treatments in clinical trials. (In the accompanying report, Landau et al. used baseline cerebrospinal fluid Aβ1–42 levels and longitudinal florbetapir PET data from the ADNI to demonstrate that a cerebral white matter reference ROI was more accurate than a cerebellar ROI in terms of its accuracy in distinguishing subjects who were expected to have longitudinal SUVR increases from those who were expected to have SUVRs that remained stable over time (22). Their data support the use of a white matter reference ROI in the analysis of longitudinal florbetapir PET scans.)
MATERIALS AND METHODS
The ADNI is a longitudinal multicenter study that provides a centralized resource for longitudinal clinical, brain imaging, and fluid biomarker data from patients with probable Alzheimer dementia (pAD), patients with MCI, and cognitively normal controls (NCs). The ADNI was launched in 2003 by the National Institute on Aging, the National Institute of Biomedical Imaging and Bioengineering, the Food and Drug Administration, private pharmaceutical companies, and nonprofit organizations. The ADNI was followed by the ADNI-GO and the ADNI-2. We referred to them collectively as ADNI in this study.
This ADNI study was approved by the institutional review boards of the participating institutions. Signed informed written consent was obtained from all participants. To date, over 1,500 adults, 55 to 90 years old, have participated in the ADNI. Current information can be found at http://www.adni-info.org/. For this study, the most fully processed PET data were downloaded from the repository for 332 participants (31 with pAD, 187 with MCI, and 114 NCs) who had undergone florbetapir PET scans at the baseline and at follow-up (∼24 mo) (between May 2010 and December 2013). For our analyses, each subject group was further stratified into Aβ-positive (Aβ+) and Aβ-negative (Aβ−) subgroups. Twenty-five pAD patients, 73 MCI patients, and 26 NCs were determined to be Aβ+ at the time of the baseline scan with a cerebral-to-whole cerebellar florbetapir SUVR and a threshold of 1.18, which was originally found to distinguish between people with and people without subsequent postmortem evidence of moderate to frequent neuritic plaques. Six pAD patients, 114 MCI patients, and 88 NCs were determined to be Aβ− (2,3). The NCs were also stratified into apolipoprotein E4 (APOE4) carrier (n = 30) and noncarrier (n = 84) subgroups irrespective of their Aβ status.
The Statistical Parametric Mapping software platform (SPM8; http://www.fil.ion.ucl.ac.uk/spm/), the FreeSurfer package (https://surfer.nmr.mgh.harvard.edu/), in-house MATLAB (The MathWorks, Inc.) scripts, and step-by-step quality control procedures were used to align each person’s 24-mo PET scan with his or her baseline scan; to deform the images into the coordinates of the Montreal Neurologic Institute template; to use the template-based ROIs (independent of each person’s own MR imaging) to characterize cerebral target ROI and cerebellar, pontine, and cerebral white matter reference ROI measurements from each scan; and to compute cerebral-to-respective reference region SUVRs.
Cerebral, cerebellar, and pontine ROIs were computed as previously described (2,3). The cerebral white matter ROI was a collection of voxels in the corpus callosum and centrum semiovale, other than those closest to gray matter or to ventricles. The template-based corpus callosum mask was from the WFU_PickAtlas toolbox (http://fmri.wfubmc.edu/software/PickAtlas). The template-based centrum semiovale mask was characterized in our laboratory with FreeSurfer to generate individual MR imaging–based ROIs in 40 randomly selected NCs, to deform the ROIs into Montreal Neurologic Institute coordinates and average them, and to include voxels with a value of at least 0.5. The template-based cerebral, cerebellar, pontine, and cerebral white matter ROIs are shown in Figure 1.
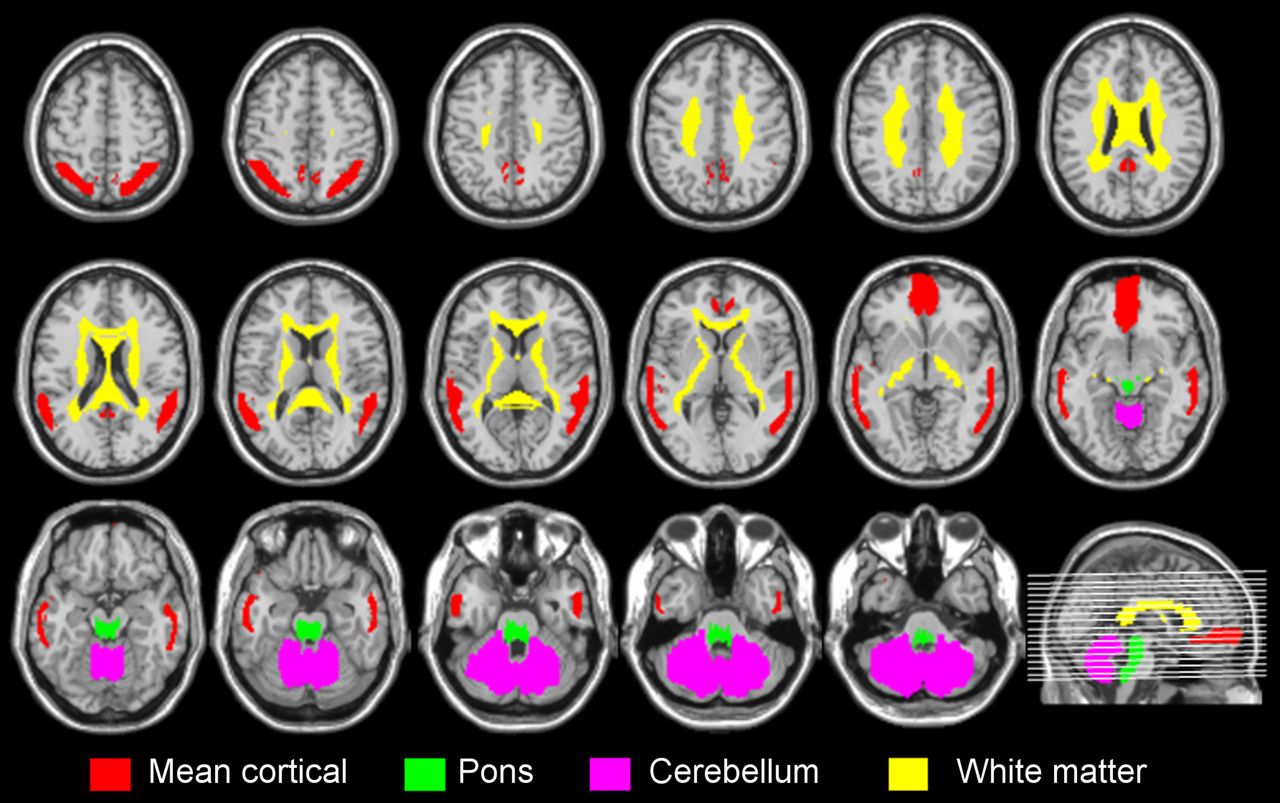
Mean cortical (red), cerebellar (magenta), pontine (green), and cerebral white matter (yellow) ROIs.
For each Aβ+, Aβ−, cognitively normal APOE4 carrier, and cognitively normal APOE4 noncarrier group, we characterized 24-mo declines in 3 commonly used clinical ratings: decreases in scores on the Mini-Mental State Examination (MMSE), increases in ratings on the 13-item version of the AD Assessment Scale Cognitive Subscale (ADAS-Cog13), and increases in scores on the Clinical Diagnostic Rating Sum of the Box (CDR-SB). We examined the within-group 24-mo cerebral-to-cerebellar, pontine, and cerebral white matter SUVR increases and such increase differences between respective Aβ+ versus Aβ− or cognitively normal APOE4 carrier versus noncarrier groups. We characterized relationships between 24-mo SUVR increases and clinical declines using simple Pearson correlation coefficients. P values were computed without correction for multiple comparisons.
For each group, we also estimated the number of participants needed per arm to detect a 25% effect of treatment in a 12-mo placebo-controlled randomized clinical trial with 80% power and a 2-tailed P of 0.05, on the basis of the assumption that SUVR increases were linear. We first estimated the sample sizes needed to detect a 25% attenuation in further SUVR increases (assuming that the treatments could not remove existing Aβ, an assumption that might make sense for the evaluation of a β-secretase inhibitor). We also estimated the much smaller number of participants needed per arm to detect a 25% clearance from the baseline level in the treatment group in comparison with the placebo group (an assumption that might make sense for Aβ immunotherapies).
RESULTS
Demographic characteristics, clinical ratings, and follow-up durations are shown for the Aβ+ and Aβ− subgroups in Table 1 and for the cognitively normal APOE4 carrier and noncarrier subgroups in Table 2.
Demographic Characteristics and Clinical Ratings of Aβ+ and Aβ− Groups*
Demographic Characteristics and Clinical Ratings of Cognitively Normal APOE4 Carrier and Noncarrier Groups
As shown in Table 3, when the cerebral white matter reference ROI was used, there were small but significant SUVR increases (P < 0.005) in the Aβ+ pAD group, the Aβ+ and Aβ− MCI and NC groups, and the cognitively normal APOE4 carrier and noncarrier groups but not in the Aβ− dementia group. In comparison, when the pontine reference ROI was used, there were small but significant SUVR increases only in the Aβ+ NC group (P < 0.005) and the Aβ+ MCI, Aβ− NC, and cognitively normal APOE4 carrier and noncarrier groups (0.005 < P < 0.05), and there was a failure to detect significant SUVR increases in the Aβ+ and Aβ− dementia and Aβ− MCI groups. When the cerebellar reference ROI was used, there were small but significant SUVR increases only in the Aβ− NC group (P < 0.005) and the Aβ+ and cognitively normal APOE4 carrier groups (0.005 < P < 0.05), and there was a failure to detect significant SUVR increases in any of the dementia or MCI groups. For each Aβ+ or Aβ− subgroup in the pAD, MCI, and NC groups and for each cognitively normal APOE4 carrier or noncarrier subgroup, 24-mo cerebral-to-white matter SUVR increases were significantly greater than cerebral-to-pons SUVR increases (P < 0.05), except in the NC Aβ+ group (P = 0.065). The cerebral-to-white matter SUVR increases over 24 mo were also higher than the cerebral-to-cerebellar SUVR increases in the AD Aβ+ and MCI Aβ+ groups (Table 3).
24-Month SUVR Changes with Pontine, Cerebellar, and Cerebral White Matter ROIs*
As shown in Figure 2 for individual Aβ+ and Aβ− pAD patients together, SUVRs generated with the cerebral white matter ROI appeared less variable and were less likely to show paradoxical decreases than those generated with the pontine and cerebellar ROIs. The trend toward changes in cerebral-to-cerebral white matter SUVRs from the baseline to the follow-up at 24 mo seemed more consistent across individual patients (and therefore resulted in reduced variability) (Fig. 2). Similar findings were observed in the other groups.
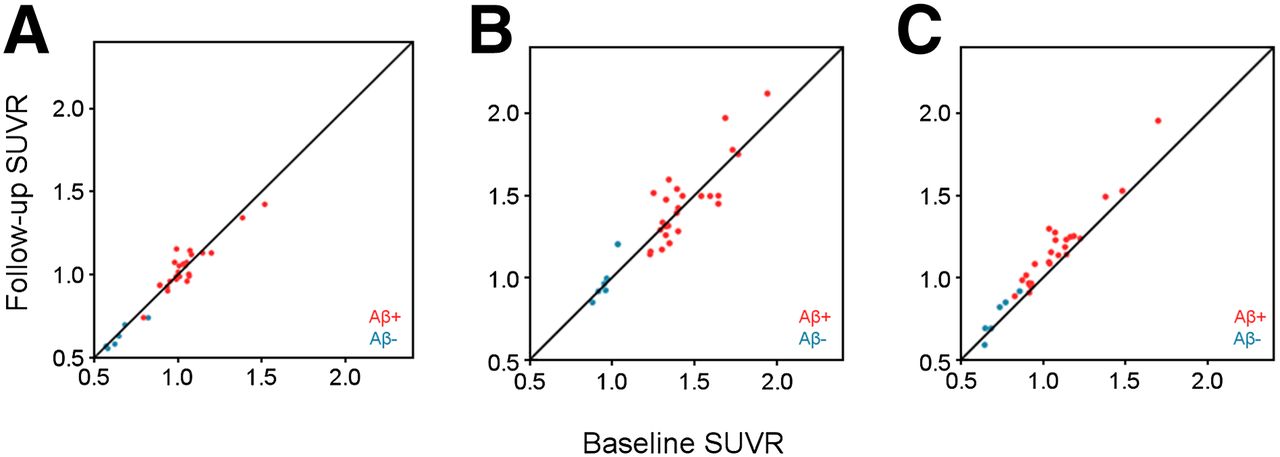
Fewer individual variations in tracking of increases in 24-mo mean cortical SUVRs with cerebral white matter ROI (C) than with pontine ROI (A) or cerebellar ROI (B), illustrated for 31 pAD patients. Red and blue dots are data for Aβ+ and Aβ− pAD patients.
As shown in Table 4, the estimated number of participants needed per arm to detect a 25% effect of treatment on further SUVR increases in a 12-mo placebo-controlled randomized clinical trial with 80% power and a 2-tailed P value of 0.05 was far smaller when the cerebral white matter reference ROI was used than when either the pontine or the cerebellar reference ROI was used, regardless of subject group. Because the power estimates were made for treatments that were not expected to actually clear existing fibrillar Aβ, the number of participants needed was quite high; still, the number was dramatically smaller when the cerebral white matter reference ROI was used.
Number of Participants Needed Per Arm to Detect Aβ-Modifying Treatment Effect in 12-Month Clinical Trial with 80% Power and 2-Tailed P of 0.05
As also shown in Table 4, the estimated number of participants needed to detect a 25% decrease in the SUVR from the baseline to 12 mo was much smaller than that needed to detect attenuation in further SUVR increases. Still, the number needed to detect this treatment effect was smaller when the cerebral white matter reference ROI was used than when either the pontine or the cerebellar reference ROI was used.
Correlations between 24-mo SUVR increases and clinical declines in the aggregate group of 31 pAD patients, 187 MCI patients, and 114 NCs with the different reference ROIs are shown in Table 5. The cerebral white matter reference ROI permitted us to demonstrate significant correlations between 24-mo SUVR increases and 24-mo MMSE score decreases (R = −0.22), ADAS-Cog13 rating increases (R = 0.24), and CDR-SB score increases (R = 0.22) (P < 0.001). Significant correlations in the predicted direction were not observed with either the pontine or the cerebellar reference ROI. (None was able to detect such significant correlations in the individual subject groups, probably because of limited sample sizes.)
Correlations Between 24-Month SUVR Increases and Clinical Declines in All Subjects
DISCUSSION
The present study demonstrated the improved power of florbetapir SUVRs to track longitudinal fibrillar Aβ increases, to characterize their relationship to longitudinal clinical declines, and to evaluate Aβ-modifying treatments with a cerebral white matter reference ROI instead of a cerebellar or pontine reference ROI.
Our decision to test the ability of the cerebral white matter reference ROI to improve power in longitudinal studies was based on the possibility that some of the variability in sequential SUVRs is attributable to the combined effects of differences in between-scan head positioning and the differential impact on measurements in a cerebral ROI (near the center of the field of view) and cerebellar and pontine ROIs (closer to the inferior field of view). We reasoned that measurements from a cerebral white matter reference ROI located approximately in the same plane as the cerebral ROI would be less vulnerable to such effects. We further reasoned that PET measurements from the cerebral white matter ROI would be less likely to be confounded by the combined effects of partial-volume averaging and spillover from cerebral gray matter because fibrillar Aβ measurements are unlikely to change over a relatively limited time.
Although our findings support the use of a cerebral white matter reference ROI for the analysis of longitudinal florbetapir PET scans, additional studies are needed to clarify whether the observed improvements in longitudinal tracking are due to differences in head repositioning in PET scanners or to other factors that influence the reference ROI measure. We are now seeking radiation dose and patient body weight data from the ADNI and other studies to compute SUVs and to clarify the extent to which there is a preferential decline in our white matter ROI SUVs (e.g., because of progressive ventricular enlargement), the extent to which there is a preferential decline in gray matter SUVs (e.g., because of progressive gray matter atrophy), and the extent to which the variability in repeated SUVs differs among white matter, cerebellar, and pontine ROIs. We predict that our white matter ROI may lead to a slight overestimation of SUVR increases, particularly in AD patients, but that this possibility does not solely account for the improvements in the power to track SUVRs. Because Aβ PET radioligands differ in their nonspecific white matter binding, it remains to be determined whether our findings can be generalized to other radioligands and to more quantitative measurements, such as the distribution volume ratio (23). Although we have not yet clarified whether longitudinal changes in white matter integrity or nonspecific binding could increase variability in cerebral-to-white-matter SUVRs, we were still able to detect improvements in precision between baseline and follow-up SUVRs. Finally, we do not believe that the improvements in SUVR variability were due to the size of the reference ROI and improved counting statistics, because the number of voxels (10,482) in our white matter ROI was smaller than that in the cerebellar ROI (13,583) and because we continued to see improved precision in a post hoc analysis of SUVRs with voxels from only the corpus callosum.
In the present study, we used a template-based cerebral white matter ROI consisting of voxels from the corpus callosum and the centrum semiovale. We have also found similar benefits of the cerebral white matter ROI and similar sample size estimates whether one evaluates changes in absolute SUVRs or the percentage change from baseline. Our data are available at the ADNI Web site. Additional studies are needed to compare our findings with those generated from individual MR imaging–based cerebral white matter ROIs. For now, we recommend using our white matter reference ROI for longitudinal analyses, and we have made the template publicly available on the ADNI website. We also recommend the use of a cerebellar or pontine reference ROI in cross-sectional comparisons (e.g., to determine Aβ positivity or negativity).
Using a method with improved power to track longitudinal SUVR increases, we found a relationship between longitudinal SUVR increases and clinical declines in the aggregate group of pAD, MCI, and NC subjects—a possibly novel finding that may provide additional support for the amyloid hypothesis. As mentioned earlier, the use of cerebral white matter ROIs to measure SUVR increases could overestimate longitudinal SUVR increases because of the combined effects of brain atrophy–related ventricular enlargement and partial-volume averaging, such that measurements in the reference ROI are progressively reduced. Although we cannot exclude that possibility, the improved power to characterize longitudinal SUVR increases was similar in the pAD, MCI, and NC groups, despite likely differences in ventricular enlargement rates.
As previously stated, longitudinal florbetapir PET SUVRs were more variable than predicted with a cerebellar or pontine reference ROI, and some of this variability may have been related to technical rather than biologic reasons. Because the technical source of variability could affect the power to detect treatment effects in clinical trials, including some that have already been reported, we recommend a reanalysis of data with a cerebral white matter reference ROI to determine whether any of the Aβ-modifying treatments now in development may have a greater effect than previously realized.
CONCLUSION
Our findings support the use of a cerebral white matter reference ROI to track longitudinal fibrillar Aβ increases with semiquantitative florbetapir PET measurements, to relate those increases to longitudinal clinical declines, and to evaluate Aβ-modifying effects with increased statistical power.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This study was supported by National Institutes of Health grant UF1AG046150, National Institute on Aging grants R01 AG031581 and P30 AG19610, and the state of Arizona (all to Eric M. Reiman). Data collection and sharing were funded by the ADNI (U01 AG024904) and DOD ADNI (W81XWH-12-2-0012) (both to Michael W. Weiner, the primary investigator). The ADNI is funded by the National Institute on Aging, by the National Institute of Biomedical Imaging and Bioengineering, and through generous contributions from the following: Alzheimer’s Association; Alzheimer’s Drug Discovery Foundation; BioClinica, Inc.; Biogen Idec Inc.; Bristol-Myers Squibb Company; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; F. Hoffmann-La Roche Ltd. and its affiliated company Genentech, Inc.; GE Healthcare; Innogenetics, N.V.; IXICO Ltd.; Janssen Alzheimer Immunotherapy Research & Development, LLC; Johnson & Johnson Pharmaceutical Research & Development LLC; Medpace, Inc.; Merck & Co., Inc.; Meso Scale Diagnostics, LLC; NeuroRx Research; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Synarc Inc.; and Takeda Pharmaceutical Company. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. Private-sector contributions are facilitated by the Foundation for the National Institutes of Health (www.fnih.org). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer’s Disease Cooperative Study at the University of California—San Diego. ADNI data are disseminated by the Laboratory for Neuro Imaging at the University of Southern California. No other potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Vivek Devadas for technical assistance. Data used in the preparation of this article were obtained from the ADNI (http://adni.loni.usc.edu/). As such, the ADNI investigators contributed to the design and implementation of the ADNI or provided data but did not participate in the analysis or writing of this report. A listing of ADNI investigators can be found at http://adni.loni.usc.edu/wpcontent/uploads/how_to_apply/ADNI_Acknowledgment_List.pdf.
Footnotes
Published online Mar. 5, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication October 22, 2014.
- Accepted for publication December 26, 2014.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Association of Age-Related and Off-Target Retention with Longitudinal Quantification of [18F]MK6240 Tau PET in Target Regions
- The RSNA QIBA Profile for Amyloid PET as an Imaging Biomarker for Cerebral Amyloid Quantification
- First-in-Humans Evaluation of 18F-SMBT-1, a Novel 18F-Labeled Monoamine Oxidase-B PET Tracer for Imaging Reactive Astrogliosis
- Comparison of 11C-Pittsburgh Compound B and 18F-Flutemetamol White Matter Binding in PET
- The association of age-related and off-target retention with longitudinal quantification of [18F]MK6240 tau-PET in target regions
- An optimized reference tissue method for quantification of tau protein depositions in diverse neurodegenerative disorders by PET with 18F-PM-PBB3 (18F-APN-1607)
- Studying APOE {varepsilon}4 Allele Dose Effects with a Univariate Morphometry Biomarker
- Multi-method investigation of factors influencing amyloid onset and impairment in three cohorts
- Regional Amyloid Accumulation and White Matter Integrity in Cognitively Normal Individuals
- Impact of Reference and Target Region Selection on Amyloid PET SUV Ratios in the Phase 1b PRIME Study of Aducanumab
- White Matter Reference Region in PET Studies of 11C-Pittsburgh Compound B Uptake: Effects of Age and Amyloid-{beta} Deposition
- Optimizing Longitudinal Amyloid-{beta} PET Measurement: The Challenges of Intensity Normalization
- Flortaucipir F 18 Quantitation Using Parametric Estimation of Reference Signal Intensity
- Memory decline accompanies subthreshold amyloid accumulation
- Increased florbetapir binding in the temporal neocortex from age 20 to 60 years
- APOE genotype and early {beta}-amyloid accumulation in older adults without dementia
- Validation of the Semiquantitative Static SUVR Method for 18F-AV45 PET by Pharmacokinetic Modeling with an Arterial Input Function
- Optimal Reference Region to Measure Longitudinal Amyloid-{beta} Change with 18F-Florbetaben PET
- Predicting Regional Pattern of Longitudinal {beta}-Amyloid Accumulation by Baseline PET
- PET Amyloid Analyses
- Optimal Target Region for Subject Classification on the Basis of Amyloid PET Images
- Measurement of Longitudinal {beta}-Amyloid Change with 18F-Florbetapir PET and Standardized Uptake Value Ratios