


Abstract
Standard pretreatment staging for gastric cancer includes CT of the chest, abdomen, and pelvis; gastroscopy; and laparoscopy. Although 18F-PET combined with CT has proven to be a useful staging tool in many cancers, some gastric cancers are not 18F-FDG–avid and its clinical value is still debatable. Methods: Gastric cancer patients who underwent staging 18F-FDG PET scans from 2002 to 2013 at the Peter MacCallum Cancer Center were retrospectively analyzed, and a systematic review was also conducted using PubMed between 2000 to March 2014 to investigate clinicopathologic parameters associated with 18F-FDG avidity. A pretreatment PET scoring system was developed from predictors of 18F-FDG avidity. Results: Both the retrospective analysis of the patients and the systematic literature review showed similar significant predictors of 18F-FDG avidity, including large tumor size, non–signet ring cell carcinoma type, and glucose transporter 1–positive expression on immunohistochemistry. A PET scoring system was developed from these clinicopathologic parameters that allowed 18F-FDG–avid tumors to be detected with a sensitivity of 85% and a specificity of 71%. Conclusion: A pretreatment PET scoring system can assist in the selection of patients with gastric adenocarcinoma when staging 18F-FDG PET is being considered.
Gastric cancer is the fourth most common cancer and the second leading cause of cancer death worldwide (1). Despite the decline in the incidence of gastric cancer over the past 50 y, the 5-y survival rate still remains low because of the asymptomatic or nonspecific clinical presentation, resulting in advanced disease at the time of diagnosis (1).
Surgery remains the only curative treatment, and thus accurate preoperative staging is essential to select the most effective treatment modality for patients. Current standard staging for gastric cancer includes CT of the chest, abdomen, and pelvis; gastroscopy; and laparoscopy.
18F-FDG PET, now routinely combined with CT as a hybrid imaging modality, is a noninvasive functional imaging modality that has proven to be a useful staging tool in many cancers, including esophageal and lung cancer (2,3). However, its clinical value in gastric cancer remains controversial, as reports indicate that gastric cancer is not 18F-FDG–avid in up to 53% of cases (4–10). This lack of avidity can result in a relatively low sensitivity for the detection of the primary tumor, nodal disease, and, consequently, distant metastatic disease. Such false-negative results decrease confidence in the utility of this technique, and accordingly, it is not currently used as a routine staging tool in gastric cancer.
The recent literature suggests that 18F-FDG avidity correlates with certain clinicopathologic parameters in gastric cancer. The intestinal subtype has appeared to have higher 18F-FDG uptake than the diffuse subtype of gastric cancer (11–13).
We conducted a systematic literature review, as well as a retrospective analysis on gastric cancer patients who underwent staging 18F-FDG PET or 18F-FDG PET/CT at our institution, to evaluate preoperative clinicopathologic parameters associated with high 18F-FDG avidity. Significant predictors of 18F-FDG avidity were used to develop a pretreatment PET scoring system for the selection of gastric cancer patients who may benefit from staging 18F-FDG PET.
MATERIALS AND METHODS
Systematic Literature Review
Selection of Articles
An electronic literature search was conducted using PubMed to select articles from January 2000 to March 2014 evaluating patients who underwent preoperative 18F-FDG PET in the staging of gastric cancer. The search terms were “PET” and “gastric cancer.” Additional database searches of the Cochrane Database of Systematic Reviews, PROSPERO, DARE, and Embase were also performed.
Articles were restricted to those in English with full-text article and detailing clinicopathologic characteristics of the primary tumor with the detection rate of 18F-FDG avidity, which was defined as focally increased 18F-FDG uptake compared with surrounding tissue. Because of the discordance of standardized uptake values among studies, articles were excluded if the study had looked at only the standardized uptake value of the primary tumor. Attempts were made to contact the authors to obtain the detection rate of 18F-FDG avidity from these studies, but these attempts were unsuccessful and these studies were excluded.
Articles were excluded if 18F-FDG PET had been performed for restaging, assessment of treatment response, and detection of recurrence of the disease. Gastroesophageal junction tumors and other gastric malignancies, including gastrointestinal stromal tumor and gastric lymphoma, were also excluded.
Data Extraction and Analysis
The primary investigator reviewed all articles independently and met with the other investigator to arrive at a consensus on the final selected articles. In total, 504 articles were identified from the PubMed database, and after application of our inclusion and exclusion criteria, 18 articles were selected.
The clinicopathologic parameters in these studies were dichotomized into the following: tumor stage (early gastric cancer [EGC] or advanced gastric cancer [AGC]), site of the tumor (proximal one third or distal two thirds), size of the tumor (small [<3 cm] or large [>3 cm]), Lauren classification (intestinal or diffuse), World Health Organization (WHO) classification (signet ring cell [SRC] carcinoma or non-SRC), and glucose transporter 1 (GLUT1) status (GLUT1-positive or GLUT1-negative).
The proportion of 18F-FDG–avid tumors for each clinicopathologic parameter was extracted from the selected studies and combined to obtain the total detection rate of 18F-FDG avidity. Odds ratios with 95% confidence intervals and P values were estimated with a random effects model using the Mantel–Haenszel method to identify parameters significantly associated with 18F-FDG avidity. The level of significance was a P value of less than 0.05.
Retrospective Analysis
Patients
Forty patients with histologically proven gastric adenocarcinoma who underwent pretreatment staging 18F-FDG PET or 18F-FDG PET/CT at Peter MacCallum Cancer Center (PMCC) from January 2002 to December 2013 were examined retrospectively from the PMCC PET database to assess predictors of the 18F-FDG avidity of the primary tumor. Only patients who had undergone gastroscopy or surgery at PMCC were included, so that we could perform immunohistochemistry for GLUT1. This study was approved by the Peter MacCallum Cancer Centre Ethics Committee.
Data Collection
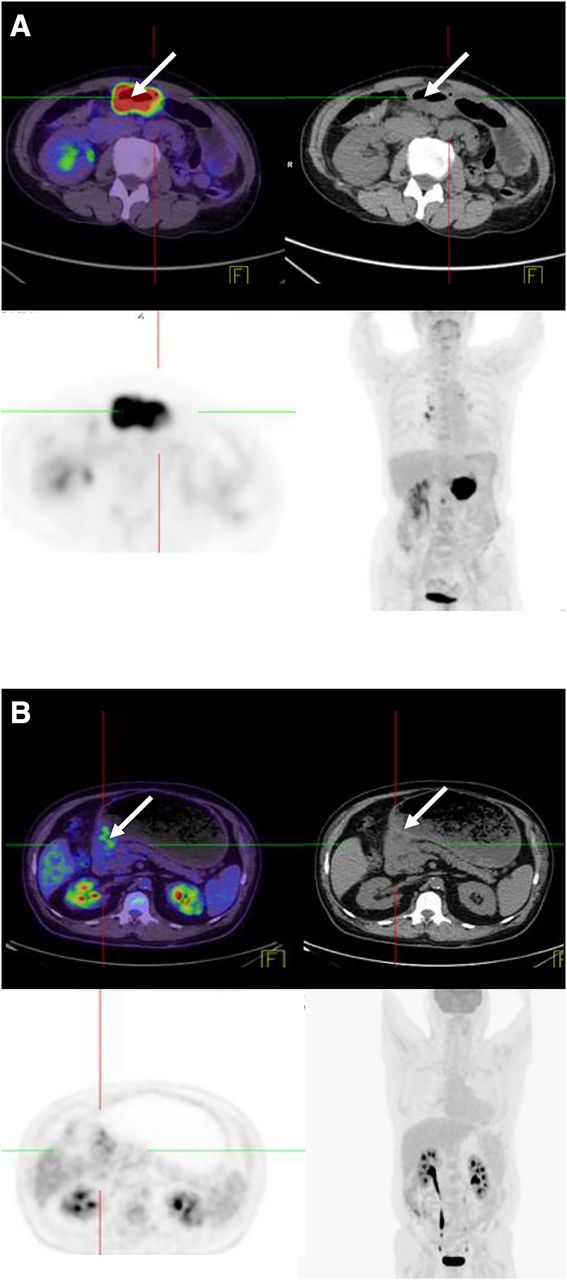
A standard protocol for 18F-FDG PET/CT, including patient preparation and the processing method, has been used and described previously (14). 18F-FDG PET or 18F-FDG PET/CT reports were reviewed to identify whether the primary tumors were 18F-FDG–avid or not. A primary tumor was considered 18F-FDG–avid if the PET report described intensely or moderately increased radiotracer uptake in the stomach relative to the rest of the gastric wall; a primary tumor was considered not 18F-FDG–avid if the PET report did not indicate any evidence of significant metabolic uptake in the stomach. Representative images of an avid and nonavid gastric adenocarcinoma are shown in Figure 1.
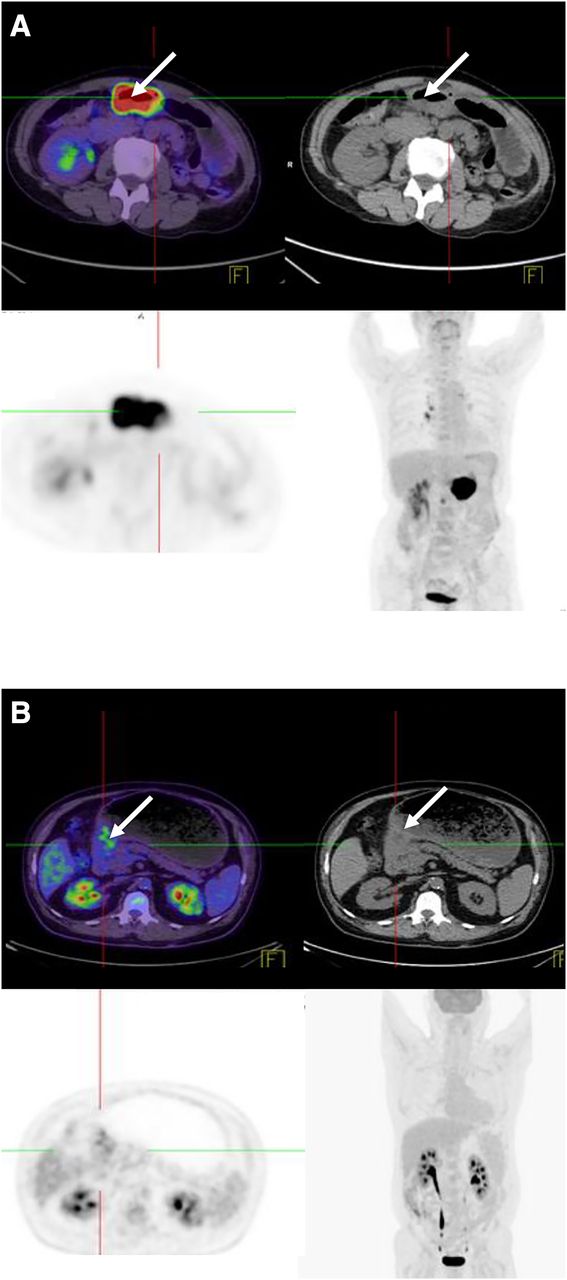
18F-FDG PET/CT image of avid and nonavid gastric adenocarcinoma. (A) Avid gastric adenocarcinoma shows intense uptake in gastric antrum, and corresponding CT image demonstrates thickening of gastric antrum wall (arrow). Nonavid gastric adenocarcinoma (B) shows minimal uptake in pylorus (considered to be physiologic), with marked focal thickening on corresponding CT image consistent with site of known primary tumor (arrow).
Pretreatment clinicopathologic parameters were obtained from the patient’s electronic medical records and included stage, site, and size of the primary tumor and histologic subtype according to the Lauren and WHO classifications. AGC was defined as a bulky or large mass detected on gastroscopy, along with a CT report of a thickened or irregular gastric wall. EGC was defined as slight elevation, no mass, or mucosal abnormality detected on gastroscopy and no evidence of mass on CT.
GLUT1 Immunohistochemistry and Semiquantitative Analysis
GLUT1 staining is not routinely performed on biopsy or resection specimens of gastric cancer in our institute unless requested. Archived formalin-fixed paraffin-embedded tissue blocks from biopsy or resection specimens were retrieved from pathology storage. Tissue blocks were not available for 3 patients, leaving 37 evaluable specimens. Three-micrometer sections were prepared and mounted on positively charged microscope slides. Immunostaining was performed using antihuman GLUT1 antibody (Thermo Fisher Scientific) at 1:200 dilution (v/v) on the automated BenchMark Ultra system (Ventana Medical Systems) using the UltraView detection reagents. The slides were then counterstained using Mayer hematoxylin before scoring. Erythrocytes were used as an internal positive control. Semiquantitative analysis was done by an experienced pathologist who was masked to all clinical data. Previous studies have considered more than 30% GLUT1-positive cells as high GLUT1 expression (15–17) in gastric cancer. In our study, we applied immunoreactive score as described previously, with modification (18). GLUT1 expression was categorized by percentage of positive staining: 0% (0), less than 10% (1), 11%–30% (2), or more than 31% (3). The intensity of staining was categorized as no staining (0), weak staining (1), moderate staining (2), or strong staining (3). The immunoreactive score was obtained by multiplying the level of staining intensity by the percentage of positive tumor cells, resulting in a scale ranging from 0 to 9 and scored accordingly: negative GLUT1 expression (score 0), positive weak GLUT1 expression (1–3 = score 1), positive moderate GLUT1 expression (4–5 = score 2), and positive strong GLUT1 expression (6–9 = score 3). An immunoreactive score above 1 was considered GLUT1-positive expression.
Data and Statistical Analysis
Similar to the systematic literature review, the proportion of 18F-FDG–avid tumors for each clinicopathologic parameter was calculated followed by univariate and multivariate analysis using logistic regression. The multivariate model was determined using backward selection methods. Statistical analysis was conducted using SAS software (SAS Institute). The level of significance was a P value of less than 0.05.
Pretreatment PET Scoring System
Clinicopathologic parameters significantly associated with 18F-FDG avidity were assigned a score obtained from the systematic literature review odds ratio. This scoring system was developed in reference to a similar scoring method described previously (19). Odds ratio was rescaled using a logarithmic scale. The PET scoring model was tested on our retrospective cohort, and the total score was compared between tumors that were 18F-FDG–avid and those that were not. To evaluate the performance of this scoring system, a receiver-operating-characteristic (ROC) curve analysis was performed.
To ascertain the best possible PET scoring model in our study, we developed multiple models with different combinations of clinicopathologic parameters and selected the model that the authors agreed produced the highest area under the ROC curve. The ROC curve was created using SPSS software (IBM Corp.).
RESULTS
Systematic Literature Review
Eighteen articles were selected: 10 retrospective studies and 8 prospective studies, with most (16/18 articles) being from non-Western data. 18F-FDG avidity ranged from 42% to 96%, with a mean of 73%, as summarized in Table 1. The studies are outlined in Supplemental Table 1, and the clinicopathologic parameters and 18F-FDG avidity for each study are described in Supplemental Table 2 (supplemental materials are available at http://jnm.snmjournals.org).
18F-FDG Avidity of Studies Included in Systematic Review
Five clinicopathologic parameters—tumor stage, size, site, WHO classification, and GLUT1 status—were significantly associated with 18F-FDG avidity. AGC had significantly higher avidity (85.6%, 752/878) than EGC (26.8%, 99/370). Similarly, large tumors (70.8%, 209/295), non-SRC tumors (64.5%, 487/755), proximal tumors (75.7%, 134/177), and GLUT1-positive tumors (70.8%, 17/24) were also associated with high avidity. Table 2 summarizes the clinicopathologic parameters and 18F-FDG avidity from the systematic literature review.
Systematic Literature Review Univariate Analysis
Retrospective Analysis of PMCC Cohort
The mean age of the 40 PMCC gastric cancer patients for whom staging 18F-FDG PET or 18F-FDG PET/CT scans were available was 65.7 y (range, 35–89 y). There were 25 men and 15 women. Twenty-six patients (65%) had tumors avid for 18F-FDG, and the remaining 14 had nonavid tumors.
Most GLUT1-positive tumors were 18F-FDG–avid (89%, 16/18 cases). Tumors with a GLUT1 score of 3 were more likely to be avid than those with scores of 0 to 2 (score 3 odds ratio, 5.87; 95% confidence interval [CI], 1.26–27.45; P = 0.0004). Furthermore, higher rates of GLUT1 positivity were observed among patients with non-SRC tumors than among patients with SRC tumors (63% compared with 23%, respectively: P = 0.04).
Most patients had advanced disease (34/40) at the time that imaging was performed. Univariate analysis demonstrated that large tumors (75%, 24/32), non-SRC tumors (84%, 21/25), intestinal tumors (82%, 14/17), and GLUT1-positive tumors (89%, 16/18) had significantly higher 18F-FDG avidity than did small tumors (25%, 2/8), SRC tumors (33%, 5/15), diffuse tumors (50%, 11/22), and GLUT1-negative tumors (42%, 8/19), respectively (Table 3). A non-SRC tumor type and GLUT1 positivity were the only independent predictors for 18F-FDG avidity according to the multivariate analysis (Table 4).
Retrospective Univariate Analysis
Retrospective Multivariate Analysis
Pretreatment PET Scoring System
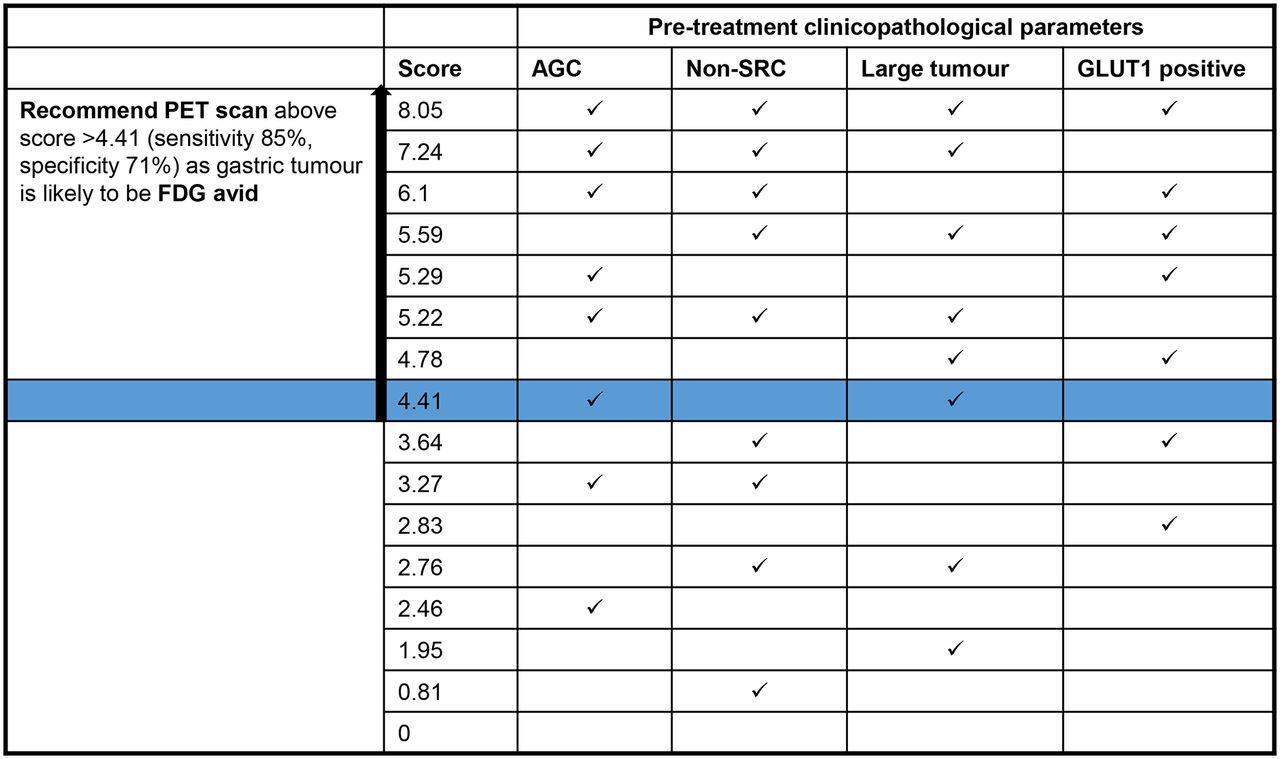
To obtain the best pretreatment PET scoring system, we developed several scoring models using different combinations of clinicopathologic parameters (tumor stage, tumor size, WHO classification, and GLUT1 status) that the systematic literature review indicated were significantly associated with 18F-FDG avidity. The selected model yielded a total of 16 different combinations of parameters with a combined score ranging from 0 to 8.05 (Table 5). When this PET scoring system was tested on our retrospective cohort, the mean total score was significantly higher for 18F-FDG–avid patients than for nonavid patients (6.67 and 3.56, respectively; P < 0.00001). A score above 4.41 could distinguish between avid and nonavid tumors with a sensitivity of 85% and a specificity of 71% (P < 0.001) (Fig. 2).
Clinicopathologic Predictors for Preoperative PET Scoring System

Preoperative 18F-FDG PET scoring system. ROC curve was used to evaluate performance of preoperative PET scoring system. Score above 4.41 distinguished between avid and nonavid tumor with sensitivity of 85% and specificity of 71% with GLUT1 status included (P < 0.001). aUnder nonparametric assumption.
As a result, we propose a checklist containing key prestaging clinicopathologic parameters associated with 18F-FDG avidity in gastric cancer (Fig. 3). This checklist can be used as a guide in selecting which patients should undergo staging 18F-FDG PET.

Proposed checklist to determine whether 18F-FDG PET scanning should be recommended for gastric cancer patient.
DISCUSSION
For 18F-FDG–avid gastric tumors, 18F-FDG PET has been shown to have high clinical value in assessing chemotherapy response (20) and in detecting recurrent disease (21). However, the routine use of 18F-FDG PET in preoperative staging has been suggested to be of limited value because of its low sensitivity for the detection of the primary gastric cancer and lymph node metastases (9,22).
The incidence of 18F-FDG avidity in gastric adenocarcinomas varies greatly in the literature (47%–96%) (4). Selection bias is likely to have contributed to the higher rates of 18F-FDG–avid stomach cancer seen in the systematic review (mean, 73%) and in our own retrospective cohort (65%). At our institution, patients with bulkier tumors and a greater likelihood of having nodal and distant metastases were more likely to have undergone PET.
Differences in cellularity, mucinous content, and GLUT1 expression in the 2 main histologic subtypes of gastric adenocarcinoma can influence cellular 18F-FDG uptake (12,15). Several studies reported that the Lauren intestinal type of gastric cancer had higher 18F-FDG uptake than the diffuse type (12,13,23,24). Low 18F-FDG uptake in some gastric cancers may be explained by high extracellular mucin content and more dispersed and diluted tumor cells. Consistent with the published literature, intestinal gastric cancers were more 18F-FDG–avid in our retrospective-cohort patients. However, in the systematic review, there was no significant difference in 18F-FDG avidity between the 2 subtypes of gastric adenocarcinoma, possibly because most patients in the systematic review were Asian. Previous studies have shown ethnic disparity in etiology and overall survival of gastric cancer (25). Non-SRC gastric tumors were significantly associated with high 18F-FDG uptake in both the systematic literature review and our retrospective cohort analysis. This observation is consistent with reports by Mukai et al. and Yamada et al. that lack of 18F-FDG avidity in gastric cancer is associated with SRC morphology (13,17).
AGC had significantly higher 18F-FDG avidity than EGC. 18F-FDG avidity above 90% in AGC was observed in more than half the studies included in the systematic literature review (5,7,8,26–29). The low spatial resolution of PET and the physiologic uptake of 18F-FDG by benign processes such as gastritis, or simply physiologic uptake in the muscularis mucosae, make it difficult to detect early small-volume gastric cancer through a combination of partial-volume effects and high adjacent background activity. Similarly, greater depth of tumor invasion and the presence of nodal disease have been correlated with tumoral 18F-FDG uptake (13,23,30).
GLUT1 overexpression has been shown to be associated with increased cellular metabolism and glucose utilization (16). Hence, overexpression of GLUT1 may be a marker for higher 18F-FDG uptake by malignant cells. In gastric cancer, the frequency of GLUT1 expression has been reported to vary between 16.9% and 60% (15–17,31). There have been only a few studies on GLUT1 expression and 18F-FDG avidity in gastric cancer (15,17,32). Consistent with our current study, Yamada et al. reported that GLUT1-positive tumor cells were significantly associated with 18F-FDG avidity (17). Similarly, gastric tumors with a high standardized uptake value on PET were shown to correlate with GLUT1 overexpression (15). However, Takebayashi et al. did not find any correlation between the standardized uptake value of primary gastric cancer and GLUT1 expression. Those authors reported hypoxia-inducible factor 1α to be another potential clinicopathologic parameter for 18F-FDG avidity in gastric adenocarcinomas (32).
Currently, there are no clear guidelines on the use of 18F-FDG PET for the staging of gastric cancer. Our study demonstrated that certain clinicopathologic factors such as large tumor size, advanced tumor stage, non-SRC histologic subtype, and GLUT1-positive expression were high predictors of 18F-FDG avidity in gastric cancer. Identifying 18F-FDG–avid predictors in gastric cancer would enable 18F-FDG PET/CT to be used with greater confidence for assessing the extent of disease before planned surgical resection. Given the poor prognosis of gastric cancer, the ability to identify macroscopic distant metastases would have significant management implications by sparing patients futile surgery and allowing earlier initiation of systemic therapy. Conversely, being able to prospectively predict patients with a low likelihood of 18F-FDG avidity could spare the expense of 18F-FDG PET/CT. This is particularly relevant in jurisdictions such as Australia, where 18F-FDG PET/CT for the staging of gastric cancer is not currently reimbursed. In such settings, a low-cost GLUT1 test could be performed rather than outlaying the high cost of a PET scan that may provide no diagnostic benefit. In an era of increasing scrutiny on the costs of imaging and the risks of unwarranted radiation exposure, our data may also provide an economic case for funding of GLUT1 staining in settings where it is not currently reimbursed. Thus, our proposed PET scoring system can be useful in supporting clinical decision making and in selecting patients who may benefit from staging 18F-FDG PET/CT.
The limitations of the current study are the heterogeneity of patient groups in the systematic literature review, as well as the relatively small sample size in our retrospective analysis. Some patients had external CT scans without optimal gastric distension, making assessment of abnormal gastric wall thickening more difficult.
Interobserver variation among pathologists was not formally assessed, because GLUT1 expression scoring was determined by a single experienced pathologist. We plan to assess the reproducibility of the GLUT1 scoring system and to validate our proposed PET scoring system on a larger independent patient cohort from other collaborating institutions.
CONCLUSION
In our study, certain clinicopathologic parameters of gastric cancer could be used to predict tumoral 18F-FDG avidity, and the proposed PET scoring system may aid in the selection of patients who may benefit from staging 18F-FDG PET.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Acknowledgments
We thank Elizabeth Drummond and Annette Hogg for developing and maintaining the PET database.
Footnotes
Published online Mar. 5, 2015.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication December 10, 2014.
- Accepted for publication February 10, 2015.





{kind=link}
{kind=link}
{kind=link}