


Abstract
The objective of this study was to explore the ability of the initial Gleason score (GS) to predict the rate of detection of recurrent prostate cancer (PCa) with 18F-choline PET/CT in a large cohort of patients. Methods: Data from 1,000 patients who had undergone 18F-choline PET/CT because of biochemical evidence of relapse of PCa between 2004 and 2013 were retrieved from databases at 4 centers. Continuous data were compared by the Student t test or ANOVA, and categoric variables were compared by the χ2 test. Univariable and multivariable analyses were performed by logistic regression. Results: The GS at diagnosis was less than or equal to 6 in 257 patients, 7 in 347 patients, and greater than 7 in 396 patients. The results of 645 PET/CT scans were positive for PCa recurrence. Eighty-one percent of the positive PET/CT results were found in patients with a PSA level of greater than or equal to 2 ng/mL, 43% were found in patients with a PSA level of 1–2 ng/mL, and 31% were found in patients with a PSA level of less than or equal to 1 ng/mL; 78.8% of patients with positive PET/CT results had a GS of greater than 7. The results of 18F-choline PET/CT scans were negative in 300 patients; 44% had a GS of less than or equal to 6, 35% had a GS of 7, and 17% had a GS of greater than 7. PET/CT results were rated as doubtful in only 5.5% of patients (median PSA, 1.8 ng/mL). When the GS was greater than 7, the rates of detection of 18F-choline PET/CT were 51%, 65%, and 91% for a PSA level of less than 1 ng/mL, 1–2 ng/mL, and greater than 2 ng/mL, respectively. In univariable and multivariable analyses, both a GS of 7 and a GS of greater than 7 were independent predictors for positive 18F-choline PET/CT results (odds ratios, 0.226 and 0.330, respectively; P values for both, <0.001). Conclusion: A high GS at diagnosis is a strong predictive factor for positive 18F-choline PET/CT scan results for recurrent PCa, even when the PSA level is low (i.e., ≤1 ng/mL).
Prostate cancer (PCa) remains the leading cancer in North American and European men, with annual age-adjusted incidence rates of 85.6 and 59.3 per 100,000, respectively (1). Despite highly successful surgery and radiotherapy treatments, PCa relapses in up to 20%–40% of patients within 10 y of potentially curative local therapy (2–4). This observation suggests that PCa metastasizes relatively early in the course of the disease, probably as a result of genetic instability, including loss of metastasis suppressor genes (5–7).
PET/CT with 11C- or 18F-choline has emerged as a powerful tool for detecting recurrent disease in PCa patients, with a pooled sensitivity of 85.6% (95% confidence interval, 82.9%–88.1%) (8,9). The diagnostic performance of radiolabeled choline PET increases with increasing prostate-specific antigen (PSA) levels, reaching greater than 80% sensitivity in patients with a PSA level of greater than 2–3 ng/mL (9). Moreover, the sensitivity of radiolabeled choline PET is higher in patients with a higher PSA velocity (the rate at which PSA level increases from year to year) or a shorter PSA doubling time (9,10). However, the role of variables other than the PSA level, such as the Gleason score (GS) at diagnosis, in predicting positive radiolabeled choline imaging results remains unclear. In this regard, GS is a well-established predictive risk factor for recurrence (11), but its value in predicting positive radiolabeled choline PET/CT results has been reported to be less robust than that of the trigger PSA (the PSA level before 18F/11C-choline PET/CT) (12,13). However, most patients evaluated in previous reports, such as those by Giovacchini et al. (12) and Castellucci et al. (13), had a low GS (6 or lower). This limitation is important from a clinical point of view. The purpose of the present study was to assess the ability of the initial GS to predict the rate of detection of recurrent PCa with 18F-choline PET/CT in a large cohort of patients.
MATERIALS AND METHODS
Patients
This was a retrospective study based on patients’ files from 4 nuclear medicine centers. Between October 2004 and June 2013, 1,359 men underwent 18F-choline PET/CT scans because of biochemical evidence of recurrence of PCa after potentially curative treatment (a PSA level of ≥0.2 ng/mL in cases of radical prostatectomy and a PSA level above the previous PSA nadir measured at 3 mo after external-beam radiotherapy). Patients were included in this retrospective review if they met predefined inclusion criteria, including the availability of clinical information, such as GS (for the biopsy in cases of no surgery or for the surgical specimen), records of current and past therapies (surgery, radiotherapy, or systemic therapy), and serum PSA level at the time of the PET/CT scan. Moreover, if available, PSA velocity was calculated with the formula (PSA2 − PSA1)/Δ time, where PSA2 corresponds to the PSA level at the time of PET imaging and PSA1 corresponds to the PSA level before a Δ time from PSA2.
According to institutional policies, all patients had given their informed consent for undergoing an 18F-choline PET/CT scan and for subsequent analysis of data in an anonymized manner.
18F-Choline PET/CT Imaging
The integrated PET/CT systems used at the 4 centers were a Discovery LS scanner (GE Healthcare) in Aviano, Italy; a Biograph 16 HT PET/CT scanner (Siemens Medical Solutions) in Padua, Italy; a Biograph mCT PET/CT scanner (Siemens Medical Solutions) in Ljubljana, Slovenia; and a Discovery ST8 scanner (GE Healthcare) in Pisa, Italy. 18F-choline PET/CT included a delayed whole-body PET scan (6–8 bed positions; 2–3 min per bed position) performed 45–60 min after the intravenous administration of 18F-choline (IASOcholine; IASON GmbH) at 3.0–3.5 MBq/kg and a coregistered low-dose CT whole-body scan (140 kV; 80–120 mA) without contrast enhancement.
At each institution, 2 specialists in nuclear medicine independently reviewed the scans by visual assessment. In particular, local relapse (LR) was recorded in the presence of clear focal 18F-choline uptake in the prostate bed; lymph nodes were considered to have positive results (N+) in the presence of focal 18F-choline uptake corresponding to that in abdominal–pelvic lymph nodes (including lymph nodes of <1 cm). However, weak 18F-choline uptake at the inguinal and mediastinal lymph nodes was not considered a pathologic finding but rather was related to prevailing reactive lymphadenitis (14,15). Focal 18F-choline uptake in the skeleton or in soft tissue other than lymph nodes indicated distant metastases (M+).
Doubtful recurrent disease was defined as the presence of mild 18F-choline uptake in the skeleton without structural changes in the corresponding coregistered CT images; similarly, local disease was rated as doubtful when 18F-choline uptake in the prostate bed was weak and irregular. Doubtful interpretations were resolved by consensus between the 2 interpreters.
18F-Choline PET/CT Diagnostic Performance
Positive 18F-choline PET/CT findings were compared with the results of biopsy, surgery performed after PET/CT, and conventional imaging studies (such as CT, MR imaging, or follow-up 18F-choline PET/CT). Follow-up duration ranged from 1 to 12 mo. Positive 18F-choline PET/CT findings were considered true-positive when any of the following 5 criteria were met: confirmation on histology or confirmation on periurethral anastomosis biopsy; increase in number of pathologic 18F-choline uptake sites or increase in uptake intensity on follow-up PET/CT studies; confirmation on conventional imaging either at baseline or during follow-up; disappearance or considerable reduction of 18F-choline uptake on follow-up PET/CT scans after local or systemic treatment; or a decrease in the PSA level after local or systemic treatment. Negative 18F-choline PET/CT findings were considered true-negative in the absence of evidence of disease on periurethral anastomosis biopsy, conventional imaging, or PET/CT during follow-up. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated.
Statistical Analysis
Continuous data are presented as median and interquartile range (IQR), and categoric data are presented as numbers and percentages. Associations for paired samples were assessed with the t test or the Mann–Whitney test for nonnormal data variables, as verified with the Shapiro–Wilk test. An ANOVA was used for comparing 3 or more variables. Comparisons of dichotomized variables were performed with the χ2 test or the Fisher exact test. Sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were calculated by standard methods. Univariate and multivariate logistic regression analyses were performed to identify independent predictors of the rate of detection of 18F-choline PET/CT. Variables were selected with entry and retention set at a significance level of 0.1. Receiver operating characteristic (ROC) analysis was performed by evaluating the area under the ROC curve to assess PSA level and GS as predictors of positive PET/CT findings. Two-tailed P values of less than 0.05 were considered statistically significant. Statistical analysis was performed with SPSS software for Windows (SPSS).
RESULTS
On the basis of the criteria described earlier, a total of 1,000 patients were included in the study (Table 1). In accordance with National Comprehensive Cancer Network guidelines (version 2.2014; www.nccn.org/professionals/physician_gls/f_guidelines.asp), we classified patients as being at low risk (T1 or T2; GS of ≤6; PSA level of <10 ng/mL), intermediate risk (T2b or T2c; GS of 7; PSA level of 10–20 ng/mL), high risk (T3a; GS of 8–10; PSA level of >20 ng/mL), or very high risk (T3b or T4) or as having metastatic disease (any T and N1; any T, any N, and M1). On the basis of these classifications, 29 patients (2.9%) were at low risk, 59 (5.9%) were at intermediate risk, 55 (5.5%) were at high risk, 91 (9.1%) were at very high risk, and 73 (7.3%) had metastatic disease. Histologic data (TNM) were available for 307 patients. At the time of PET/CT, the median PSA level was 3.30 ng/mL (IQR, 1.15–11.0). Concerning the GS at diagnosis, 257 patients (25.7%) had a GS of less than or equal to 6, 347 (34.7%) had a GS of 7, and 396 (39.6%) had a GS of greater than 7. Patients with a GS of less than or equal to 6 were at low to intermediate risk (n = 44; 59.5%). Conversely, 41% of this subset of patients was at high risk or had metastatic disease. As expected, patients with a GS of greater than 7 were at high to very high risk. Most patients with a GS of greater than 7 had received more aggressive treatments (such as a combination of surgery and hormonal therapy, a combination of radiotherapy and hormonal therapy, or combinations of both) than patients with a GS of less than or equal to 7. At the time of PET/CT scanning, 257 patients were receiving hormonal therapy; 21% had a GS of less than or equal to 6, 26% had a GS of 7, and 53% had a GS of greater than 7.
Main Characteristics of the Patients
18F-Choline PET/CT Results
18F-choline PET/CT detected PCa recurrence in 645 of the 1,000 patients, with the following distribution: LR in 275 patients, N+ in 303, and M+ in 335. Moreover, 85 patients had both LR and N+ findings, 136 had both N+ and M+ findings, and 44 had LR and N+ and M+ findings.
Data were available to assess the diagnostic performance of 18F-choline PET/CT in 731 of the 1,000 patients. 18F-choline PET/CT findings were validated with histologic criteria in 26 patients (35.6%) and with imaging and clinical or biochemical criteria in the remaining 705 patients. Accordingly, there were 367 true-positive findings, 307 true-negative findings, 78 false-positive findings, and 9 false-negative findings. Thus, the sensitivity was 97.6%, the specificity was 79.7%, the positive predictive value was 82.5%, the negative predictive value was 97.2%, and the accuracy was 88.6%.
The median PSA level was significantly higher in patients with positive scan results than in those with negative scan results (6.65 vs. 1.20 ng/mL; P = 0.035). Conversely, the statistical significance was lost when the doubtful cases were included in the statistical analysis (median PSA level, 1.8 ng/mL; P = 0.0.73) (Table 2). The median PSA level was significantly higher in patients with N+ disease (2.47 ng/mL [IQR, 0.98–6.87]) than in those who did not have N+ disease (8.04 ng/mL [IQR, 2.55–21.7]) and significantly higher in patients with M+ disease (2.27 ng/mL [IQR, 1–6.07]) than in those who did not have M+ disease (8.11 ng/mL [IQR, 2.96–25]).
Correlations Between Clinical Characteristics of Patients and PET/CT Findings
As expected, increasing PSA levels were associated with increasing PET/CT positivity rates: 31% of patients with a serum PSA level of less than or equal to 1 ng/mL had positive scan results, 43% of patients with a serum PSA level between 1 and 2 ng/mL had positive scan results, and 78.8% of patients with a serum PSA level of greater than or equal to 2 ng/mL had positive scan results. Similarly, when the 18F-choline PET/CT results were stratified according to the GS at diagnosis, the scan results were positive in 49.2% of patients with a GS of less than or equal to 6, 59.4% of patients with a GS of 7, and 79% of patients with a GS of greater than 7. A PSA level of less than or equal to 1 ng/mL was associated with positive 18F-choline PET/CT results at local sites, at lymph nodes, and at distant metastases in 14.1%, 22.4%, and 28.2% of patients with a GS of greater than 7, respectively. On the contrary, a PSA level of greater than 2 ng/mL was associated with distant metastases in 51.7% of the same group of patients. Both of these findings can be useful in clinical practice for determining the best choice of treatment. Table 3 shows the correlations of the clinical characteristics of the study population and PET/CT findings. Moreover, the median value for PSA velocity, available in 505 patients, was significantly higher in patients with positive PET/CT scan results than in those with negative PET/CT scan results (7.04 vs. 1.16 ng/mL/y; P < 0.001) and was significantly higher in patients with a GS of greater than 7 than in those with a GS of less than or equal to 7 (4.86 vs. 2.20 ng/mL/y; P < 0.001).
Univariate and Multivariate Analyses
18F-Choline Detection Rate Based on GS Combined with PSA Levels
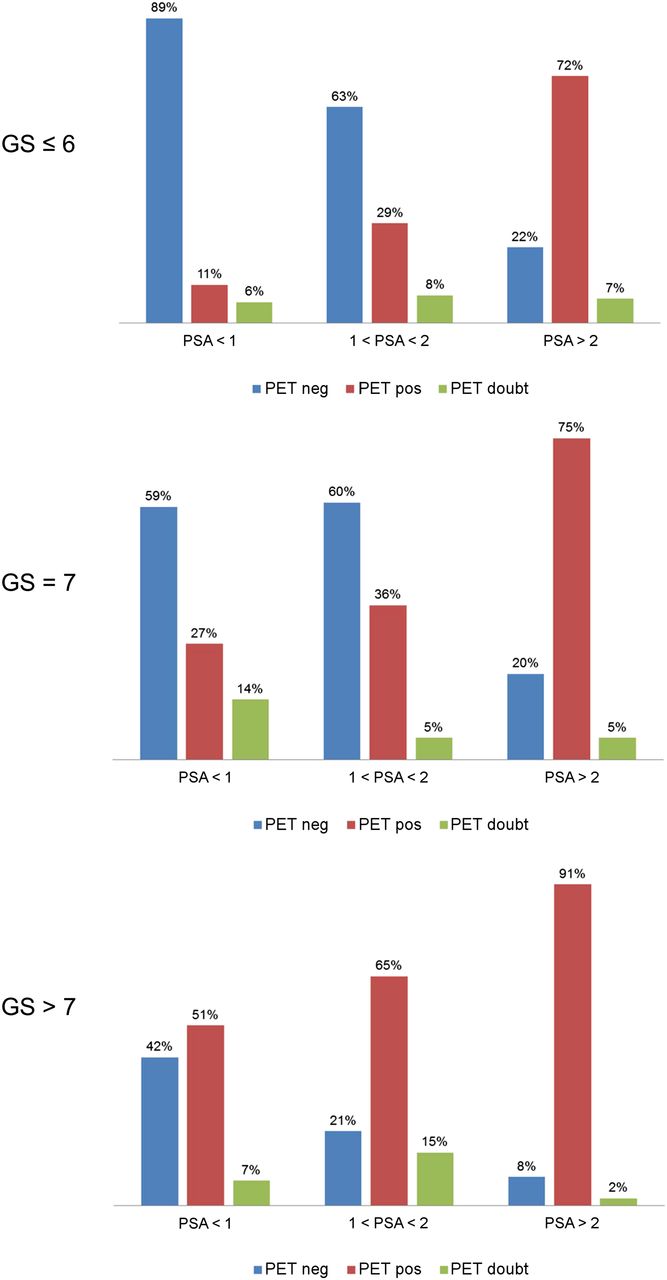
The combination of the GS at diagnosis with the serum PSA level at the time of 18F-choline PET/CT scanning had better discriminating power for positive scan results than either variable alone. In particular, when the serum PSA level at the time of the scan was less than 1 ng/mL, PCa recurrence was detected by 18F-choline PET/CT in 51%, 27%, and 10% of patients with a GS of greater than 7, a GS of 7, and a GS of less than or equal to 6, respectively. When the serum PSA level was between 1 and 2 ng/mL, 18F-choline PET/CT detected PCa recurrence in 65%, 36%, and 29% of patients with a GS of greater than 7, a GS of 7, and a GS of less than or equal to 6, respectively. Finally, when the serum PSA level was greater than 2 ng/mL, PCa recurrence was detected by 18F-choline PET/CT in 91%, 75%, and 72% of patients with a GS of greater than 7, a GS of 7, and a GS of less than or equal to 6, respectively (Fig. 1). For patients undergoing hormonal therapy at the time of the 18F-choline PET/CT scan, recurrent disease was detected in 64%, 74%, and 87.5% of patients with a GS of less than or equal to 6, a GS of 7, and a GS of greater than 7, respectively (Supplemental Table 1) (supplemental materials are available at http://jnm.snmjournals.org).

Distributions of Gleason scores and PSA cutoff values. doubt = doubtful; neg = negative; pos = positive.
ROC Analysis
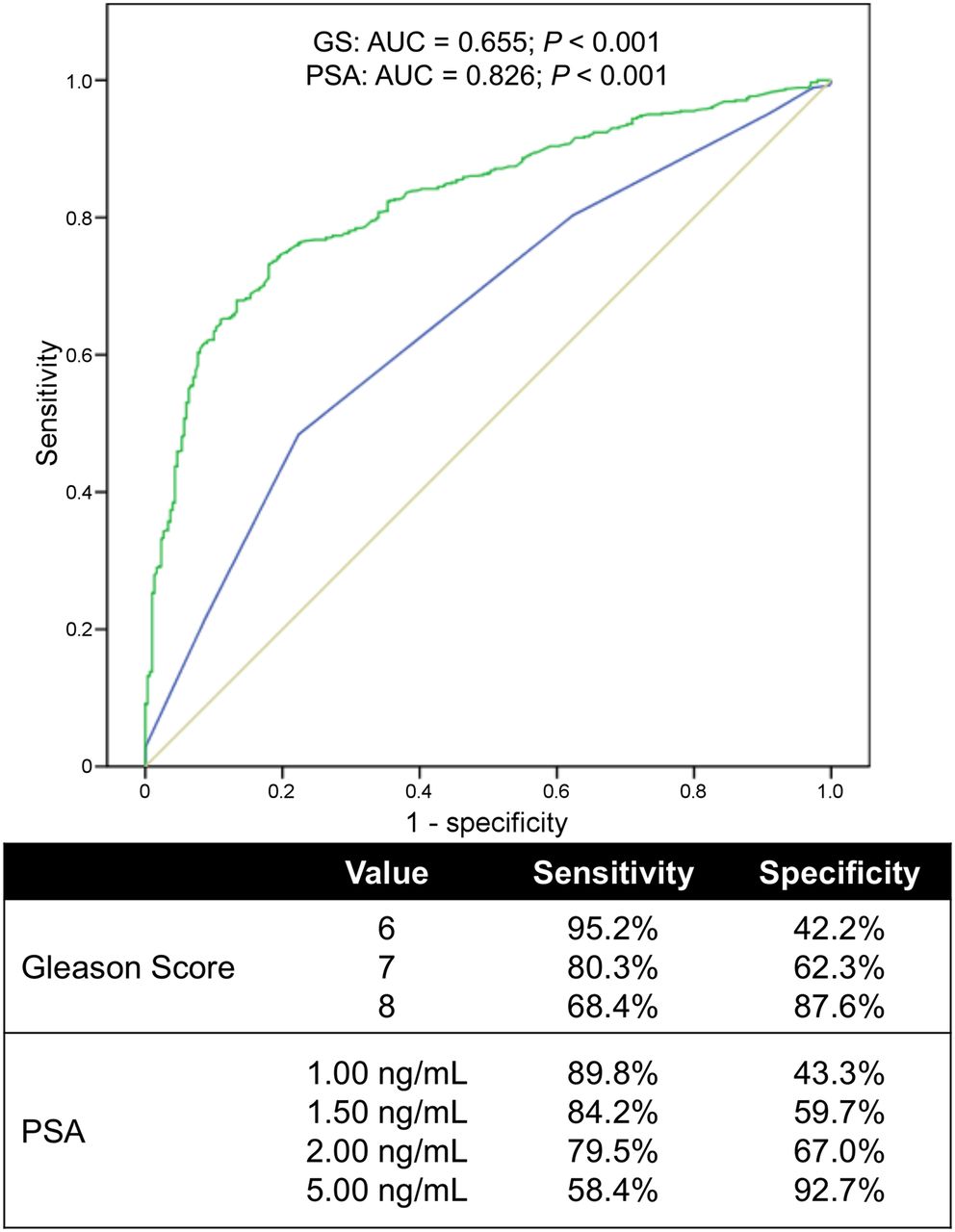
ROC analysis revealed that a GS of 7 was correlated with positive 18F-choline PET/CT results at a sensitivity and a specificity of 80.3% and 62.3%, respectively; the corresponding values for the correlation of a PSA level of 2 ng/mL with positive 18F-choline PET/CT results were 79.5% and 67.0%, respectively. The corresponding area under the curve values were 0.826 for the serum PSA level and 0.655 for the GS, respectively (both with P values of <0.001) (Fig. 2).
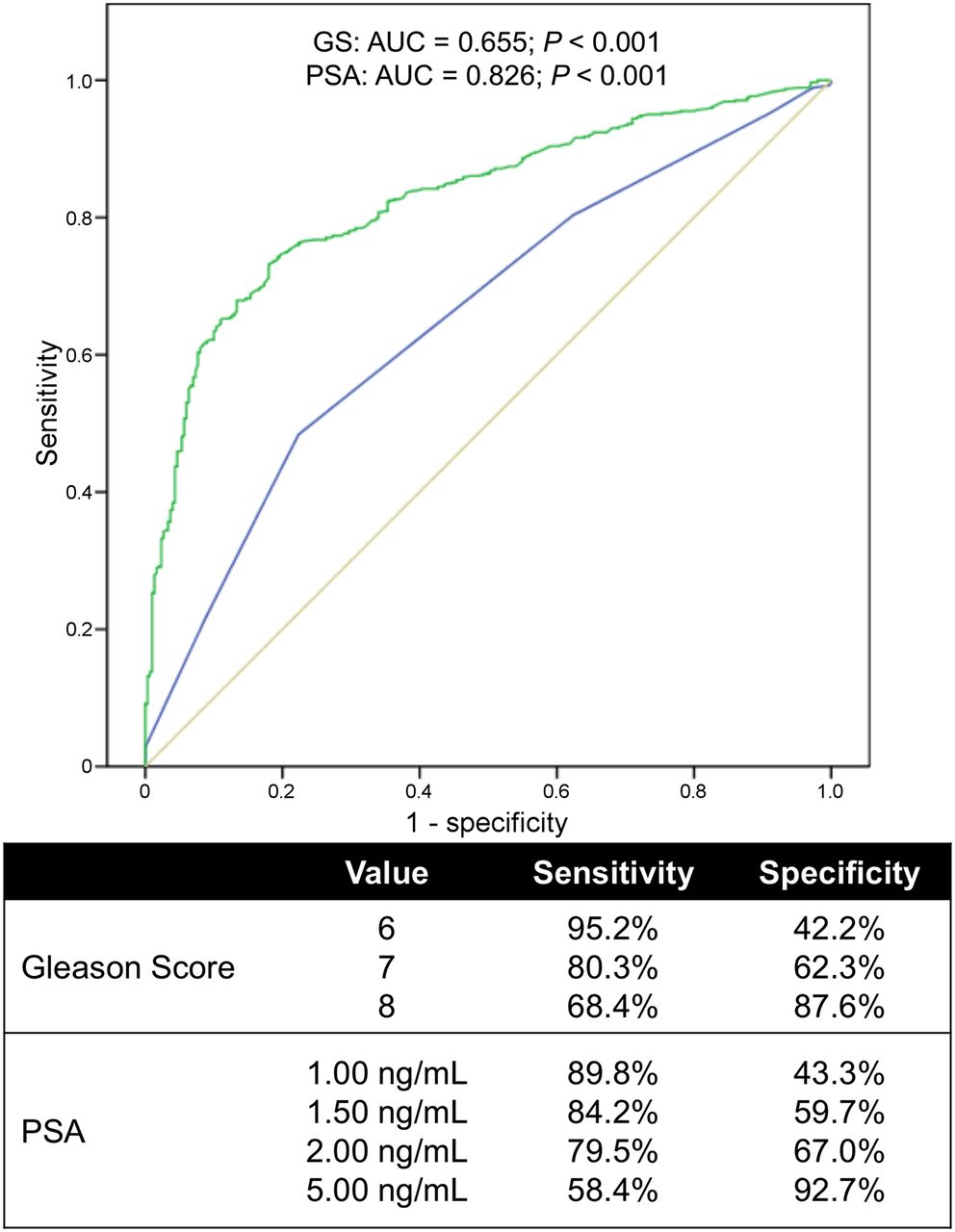
ROC analysis. Values of 1.5 ng/mL for serum PSA and 7 for Gleason score (GS) were defined as best cutoff values for predicting positive 18F-choline PET/CT scan. AUC = area under the curve.
Univariate and Multivariate Analyses
Univariate analysis (Table 3) revealed that clinical and demographic data as well as therapy-related variables were significantly correlated with positive PET/CT scan results (all P values were <0.005). However, multivariate analysis revealed that only older age, a GS of greater than or equal to 7, systemic chemotherapy, and a serum PSA level of greater than or equal to 1 ng/mL were identified as independent predictors of positive 18F-choline PET/CT results in patients with biochemical evidence of recurrence. Similarly, a GS of greater than or equal to 7 and a serum PSA level of greater than or equal to 1 ng/mL were identified as independent predictive variables for the detection of lymph node and distant metastases by 18F-choline PET/CT (all P values were <0.001). Conversely, no logistic relationship was found between the GS and LR detection (P = 0.645 and P = 0.231 for a GS of 7 and a GS of >7, respectively).
DISCUSSION
Imaging of PCa recurrence in patients with biochemical evidence of relapse of the disease remains challenging. Predominantly morphologic imaging modalities, such as CT and MR imaging, have low to moderate sensitivities for the early detection of lymph node metastases (widely ranging at 30%–80%) (16,17) and local cancer recurrence (25%–54%) (18,19). With regard to radionuclide imaging, bone scintigraphy is recommended for assessing patients at a high risk of PCa because of a PSA level of greater than 20 ng/mL or symptomatic patients (i.e., with bone pain or pathologic fracture) because metastatic disease may occur even when PSA is undetectable (20,21). On the other hand, PET with 18F-FDG is generally not recommended for detecting metastatic lesions, likely because of the low glucose metabolic rates (resulting in low tracer uptake) that often characterize PCa; this pattern is linked to the frequently low level of expression of glucose transporters on cell membranes in this type of cancer (22–24). Nevertheless, the sensitivity of 18F-FDG PET for the detection of PCa metastases is higher in patients with a GS of greater than 7, a high serum PSA level, and high PSA velocity (4,25).
The introduction of radiolabeled choline for clinical use has heralded a turning point in the role of PET imaging for patients with PCa, with overall higher sensitivity than 18F-FDG PET imaging (26). After the initial experience with 11C-choline (which requires the availability of an in-house cyclotron and radiochemistry or radiopharmacy facility), most centers have now shifted to the use of the more widely available 18F-choline. In fact, 18F-choline is characterized by a high diagnostic accuracy similar to that of 11C-choline, particularly for patients with a higher serum PSA level, higher PSA velocity, or shorter PSA doubling times (9). As recently reported by Evangelista et al. (9), the pooled sensitivity of 18F-choline PET/CT was 91.8% (range, 64.3%–100%). The sensitivity observed in the present study (97.6%) is at the upper end of this range. Nevertheless, as in most investigations published on this topic, clinical follow-up and conventional instrument examinations were used to confirm the 18F/11C-choline PET findings, making these studies primarily observational.
At variance with the established role of serum PSA in estimating the probability of 18F-choline PET/CT detection of recurrences of PCa, the role of the GS in predicting positive scan results at the time of biochemical relapse (i.e., at diagnosis) remains questionable. Several reports (27–29) confirmed the high value of the GS, which is the most commonly used grading system for PCa and which provides highly meaningful prognostic information (12,13), for predicting the clinical outcomes of PCa patients after no treatment, treatment with radical prostatectomy (with or without pelvic lymph node dissection), or treatment with radiation therapy. For patients receiving neoadjuvant or adjuvant hormonal therapy, the GS was an independent predictor of biochemical failure (30). In a study of 100 consecutive cases, it was found that when the serum PSA level was less than 4 ng/mL, 18F-choline PET/CT was positive in 54% of patients with a GS of greater than 7 but only 8% of those with a GS of less than or equal to 7 (31); these findings are consistent with those of a prior similar report (9). Castellucci et al. (13) explored the role of 11C-choline PET/CT in detecting recurrent disease in 102 patients with a lower trigger PSA level (1.5 ng/mL). Using both univariate and multivariate analyses, they found that only the PSA doubling time and lymph node status, not the initial GS, were significant and independent predictors of positive scan results; however, most of their patients (91/102, or 89%) had a GS of less than or equal to 7. Similarly, for 358 patients who had biochemical evidence of recurrence of PCa and underwent 11C-choline PET/CT, Giovacchini et al. (12) found that the GS was a less robust predictor of positive scan results than the trigger PSA; however, most of the patients (257/358, or 72%) in this series also had a GS of less than or equal to 7.
In the present study, we investigated the role of the GS at diagnosis in predicting positive 18F-choline PET/CT results in a large population that we stratified at different levels of PSA: less than 1 ng/mL, 1–2 ng/mL, and greater than 2 ng/mL. All of the scans were performed with a delayed PET protocol acquisition, and strict interpretation criteria for positive results were adopted. This comprehensive analysis showed that most patients with a serum PSA level of greater than or equal to 1 ng/mL (n = 579) had positive 18F-choline PET/CT scan results. Moreover, the rates of detection of recurrent PCa were especially high in patients with more aggressive tumors at diagnosis, that is, 59.4% and 79% in patients with a GS of 7 and a GS of greater than 7, respectively. Multivariate analysis revealed that both a GS of 7 and a GS of greater than 7 appeared to be independent predictors of positive 18F-choline PET/CT results in patients with biochemical failure of PCa (odds ratios, 0.226 and 0.330, respectively; P values for both, <0.001).
In contrast to prior studies, the present analysis involved stratification of patients into subgroups with low risk, intermediate risk, and high risk of recurrence according to the GS at diagnosis, that is, a GS of less than or equal to 6, a GS of 7, and a GS of greater than 7, respectively. In prior studies (9,12,13), patients were generally grouped together regardless of the GS-based risk of recurrence and almost exclusively on the basis of PSA-related parameters. In particular, regardless of the GS, the rates of detection of PCa recurrence with 18F/11C-choline PET/CT were reported to range widely, from 7.6% to 36% for a PSA level of less than 1 ng/mL (9,12) and from 43% to 100% for a PSA level of less than or equal to 2 ng/mL (9–11,16). In the present study, the rate of detection of 18F-choline PET/CT when the PSA level was less than 2 ng/mL was 13.2% in the overall patient population; however, it exhibited a rising trend when it was associated with the GS, that is, 13.6% for a GS of less than or equal to 6, 30.3% for a GS of 7, and 56.1% for a GS of greater than 7. As a consequence of this trend, most patients with a GS of greater than 7 and a PSA level of greater than or equal to 2 ng/mL had positive 18F-choline PET/CT scan results (n = 238, or 91.8%); nevertheless, 56.1% of patients with a GS of greater than 7 and a PSA level of less than 2 ng/mL also had positive 18F-choline PET/CT scan results. Therefore, the probability of positive 18F-choline PET/CT scan results is greater than 50% in patients with a GS of greater than or equal to 7, even with a relatively low PSA level (<1 ng/mL). Conversely, a similar rate of positive 18F-choline PET/CT scan results can be found in patients with a GS of less than or equal to 6 only when the PSA level is greater than 1 ng/mL. ROC analysis confirmed that a GS of 7 was the optimal cutoff, with a high sensitivity (80.3%) for predicting the detection of PCa recurrence with 18F-choline PET/CT; this sensitivity was similar to that in patients with a PSA level of greater than 2 ng/mL (79.5%). Taken together, these observations can serve as the basis for selecting patients for 18F-choline PET/CT scans because of suspected PCa recurrence.
As extensively reported in the literature (9), a PSA level of greater than 1 ng/mL is one of the strongest predictors of positive radiolabeled choline PET or PET/CT in patients with suspected disease relapse. We found that PSA thresholds at 1 ng/mL and 1.5 ng/mL had good sensitivity (89.8% and 84.2%, respectively) in the ROC analysis but low specificity (Fig. 2). Nevertheless, this type of analysis is somewhat problematic if the standard of reference is not histopathology in all patients. Therefore, the results of the present study emphasize the notion that the selection of patients for 18F-choline PET/CT scans should not be limited to the PSA level because a high initial GS can be associated with positive PET/CT scans even when the serum PSA level is less than 1 ng/mL.
A potential limitation of this study is that for most patients, the kinetic pattern of serum PSA was not available for analysis. In this regard, Partin et al. demonstrated that the combination of PSA velocity, GS, and lymph node status was helpful for distinguishing local recurrence from distant metastases in patients who had undergone radical prostatectomy (31). Also, a more recent reappraisal indicated that PSA alone is not an accurate indicator of tumor recurrence and that multiple diagnostic tests are necessary to stage disease recurrence (9). Finally, although the retrospective nature of the present study in principle could have introduced some bias, to our knowledge, this was the first analysis of the role of 18F-choline PET/CT in a large population of patients with suspected recurrent PCa.
CONCLUSION
For suspected PCa recurrence, a high GS at diagnosis can be associated with positive 18F-choline PET/CT scan results, regardless of the serum PSA level at the time of imaging. Therefore, the GS can be considered a robust predictive factor for positive 18F-choline PET/CT results, even at a very early stage of biochemical failure of PCa, that is, when the PSA level is less than 1 ng/mL.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. No potential conflict of interest relevant to this article was reported.
Footnotes
Published online Dec. 31, 2014.
- © 2015 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication April 18, 2014.
- Accepted for publication October 16, 2014.





{kind=link}
{kind=link}